
Abstract
Background
Herbal remedies predate written history and continue to be used frequently for many common ailments. The essential oil mixture standardized is a phytopharmaceutical with a distillate of a mixture of rectified essential oils of eucalyptus, sweet orange, myrtle, and lemon as active ingredients used to treat respiratory diseases such as bronchitis and rhinosinusitis. We evaluated the pharmacologic effects of a distillate of rectified essential oils standardized on primary human upper respiratory epithelial cultures specifically addressing electrolyte transport, cilia beat frequency (CBF), airway surface liquid (ASL) hydration, and mucus transport velocity.
Methods
Well-differentiated primary human sinonasal epithelial cultures grown at an air–liquid interface were treated on the apical or basolateral surface with varying concentrations of a distillate of rectified essential oils standardized. Changes in CBF were determined using the Sissons-Ammons Video Analysis system while changes in chloride flux were determined using the fluorescent dye 6-methoxy-N-(3-sulfopropyl)quinolinium. ASL hydration was quantified using Texas red dextran and mucociliary transport velocity was measured using fluorescent microspheres and time lapse photography.
Results
When applied to the basolateral surface, a distillate of rectified essential oils standardized activated chloride efflux and ciliary beat in a dose-dependent fashion, increasing ASL height and accelerating mucociliary transport velocity. The ancillary apical application of a distillate of rectified essential oils standardized had minimal effects on the CBF.
Conclusion
Basolateral application of a distillate of rectified essential oils standardized stimulates both chloride efflux and cilia beat frequency resulting in a synergistic effect dramatically augmenting mucociliary transport velocity. These in vitro data support the clinical efficacy of this phytopharmaceutical in respiratory inflammatory disorders.
Several in vivo studies have shown accelerated nasal mucociliary transit time and nasal patency after systemic administration of Myrtol®.3,4 Additionally, ex vivo studies of rat trachea have shown that Myrtol® stimulates ciliary beat frequency (CBF) and mucociliary clearance (MCC). 5 However, one study, although showing a significant shortening in human in vivo saccharin transit time, failed to establish effects of Myrtol® in a very low concentration on cilia function using human sinonasal explants grown in submersion. 4 In another ex vivo study with nasal epithelium of healthy subjects as well as patients with chronic obstructive pulmonary disease or bronchiectasis a significant increase of CBF was established in all groups. 6 This is in accordance with results of a study in nasal explants from patients with chronic rhinosinusitis. 7 Thus, the objective of our study was to attempt to resolve this discrepancy and investigate the effects of Myrtol® on the MCC apparatus using primary human sinonasal cultures grown at an air–liquid interface (ALI).
Methods
Solutions
Myrtol® was supplied in pure form by the sponsor of the study, G. Pohl-Boskamp (Hohenlockstedt, Germany). The stock solution was diluted 1:1 with 100% ethanol to solubilize the product and then appropriate dilutions were attained in Hank's balanced salt solution. Initial dilutions were performed to 0.5 and 0.1% and physiological efficacy evaluated. Serial dilutions were performed until no effect was seen in comparison with the vehicle control.
Sinonasal ALI Cultures
Cultures were prepared as previously described.8–10 Briefly, patients were recruited from the Division of Rhinology of the Department of Otorhinolaryngology–Head and Neck Surgery at the University of Pennsylvania and the Philadelphia Veterans Affairs Medical Center with full approval of both institutional review boards. Informed consent was obtained during the preoperative clinic visit or in the preoperative waiting room. Y. Lai and D. Dilidaer contributed equally to this work. Selection criteria for recruitment were patients undergoing sinonasal surgery. Exclusion criteria included a history of systemic diseases such as Wegener's, sarcoid, cystic fibrosis, immunodeficiencies, and use of antibiotics, oral corticosteroids, or antibiologics (e.g., omalizumab) within 1 month of surgery. Initial experiments to determine dilutions with physiological sequelae were performed in ALI cultures from non-CRS patients. Then, direct comparison of CRS versus non-CRS ALI cultures showed no difference in cilia stimulation; thus, ensuing experiments did not differentiate disease status of source material. Additionally, our prior work has indicated that cilia dynamics are not anatomically distinct 11 and, thus, location within the sinonasal cavity of the source material was not maintained. Sinonasal mucosal specimens were acquired from residual clinical material obtained during sinonasal surgery and transported to the laboratory in saline placed on ice. ALI cultures were established from human sinonasal epithelial cells enzymically dissociated human tissue and grown to confluence in tissue culture flasks (75 cm2) with proliferation medium consisting of DMEM/Ham's F-12 and bronchial epithelial basal medium (Clonetics; Cambrex, East Rutherford, NJ) supplemented with 100 U/mL of penicillin and 100 μ/mL of streptomycin for 7 days. Cells were then trypsinized and seeded on porous polyester membranes (6∼7 X 10 4 cells/membrane), in cell culture inserts (Transwell-Clear, diameter 12 mm, 0.4-μm pores; Corning, Acton, MA) coated with 100 μL of coating solution (bovine serum albumin [0.1 mg/mL; Sigma-Aldrich], type I bovine collagen [30 μ/mL; BD, St. Louis, MO], fibronectin [10 μ/mL; BD] in Laboratory of Human Carcinogenesis basal medium [Invitrogen, Grand Island, NY]) and left in a tissue culture laminar flow hood overnight. Five days later, the culture medium was removed from the upper compartment and the epithelium was allowed to differentiate by using the differentiation medium consisting of 1:1 DMEM (Invitrogen) and bronchial epithelial basal medium (Clonetics; Cambrex) with the Clonetics complements for human epidermal growth factor (0.5 ng/mL), epinephrine (5 g/mL), bovine pituitary extract (0.13 mg/mL), hydrocortisone (0.5 g/mL), insulin (5 g/mL), triiodothyronine (6.5 g/mL), and transferrin (0.5 g/mL), supplemented with 100 UI/mL of penicillin, 100 g/mL of streptomycin, 0.1 nM of retinoic acid (Sigma-Aldrich), and 10% FBS (Sigma-Aldrich) in the basal compartment.
CBF was performed as previously described.8,10 In brief, images of beating cilia from mature cultures were visualized using a 20x objective on an inverted microscope (Leica Microsystems, Inc., Bannock-burn, IL). Image data were captured using a Model A602f-2 Basler area scan high-speed monochromatic digital video camera (Basler AG, Ahrensburg, Germany) at a sampling rate of 120 frames/s with a resolution of 640 X 480 pixels. The video images were analyzed using the Sisson-Ammons Video Analysis (SAVA) system Version 2.1 (Ammons Engineering, Mt Morris Township, MI). 12 For each experiment, a large area of beating cilia on the ALI cultures was detected with the inverted microscope. The digital image signal was then routed from the camera directly into a digital image acquisition board (National Instruments) within a Dell XPS 710 Workstation running Windows XP Professional operating system (Microsoft, Redmond, WA). Images were captured, compressed, and stored to disk. Files were reloaded and analyzed with virtual instrumentation software highly customized to perform CBF analysis. All of the recordings for the proposed experiments were made at 200x magnification. Experiments were all performed at ambient temperature (22°C). Whole field analysis was performed with each point measured representing one cilia. For each sample, the reported frequencies represent the arithmetic means of these values, followed by standard deviations. Because the data include thousands of individual points (cilia), very small changes in CBF result in a “statistical” significance because of the high power of the analysis methods. Thus, statistical analysis of the arithmetic means derived from each culture was performed using two-tailed unpaired t-tests to ensure reproducibility. Once a stable baseline was obtained, the test solution or control solution was added at varying doses to the basolateral media or apical surface and CBF was recorded every 15 minutes for the 1st hour and then every 30 minutes for the 2nd hour. Cultures were then placed back in the incubator and analyzed again at 6 hours.
Mucociliary transport velocity was measured using 2-μm polystyrene fluorescent microspheres (0.0025% by weight in 30 μL) that were added to the apical surface of the cultures after copious washing with PBS to remove mucus clumps as previously described.9,10 Beads were imaged using an inverted Nikon TE2000E epifluorescence microscope (20 X 0.5 NA PlanFluor objective; Nikon, Tokyo, Japan) equipped with a 12-bit QImaging camera (Q Imaging, Surrey BC, Canada) and computer running ImageJ (Wayne S. Rasband, National Institutes of Health, Bethesda, MD) and μManager. 13 A streak had to have a visible beginning and ending, within the field of view, to be included in the statistical analysis of the data. Either an ND4 or ND8 filter was used for bead-tracking experiments, depending on the thickness of the individual epithelial culture and resulting brightness of the beads.
Transepithelial potential (TEP) was measured using the EVOM handheld module (World Precision Instruments, Sarasota, FL) per the manufacturer's guidelines and as previously described. 14 Briefly, the apical and basolateral sides of the Costar transwell were bathed in Hank's balanced salt solution, the electrodes were inserted into the two compartments, and the TEP was taken after reaching the steady state. Myrtol® was added to the basolateral medium at the designated concentration and TEP was reobtained 45 minutes later. TEP is reported with the basolateral as the ground side (i.e., a negative TEP equals a net lumen-negative potential).
Apical chloride permeability was measured indirectly by loading the cells with the fluorescent dye 6-methoxy-N-(3-sulfopropyl)quinolinium and replacing the apical chloride with NO3− as previously described. 9 Because Cl− channels have a near equal permeability for Cl− and NO3−, replacement of apical Cl− with NO3− results in electroneutral Cl−/NO3− exchange across the apical membrane. SPQ is quenched by Cl− but not NO3−; thus, the relative rates of SPQ fluorescence increase during NO3− substitution can be used to determine the relative rates of anion permeability. NO3− substitution experiments were performed with control Dulbecco's phosphate buffered saline containing 138 mM of NaCl for a total apical [Cl−] of ∼147 mM. The low Cl− Dulbecco's phosphate buffered saline contained 5 mM of NaCl and 133 mM of NaNO3 for a total apical [Cl−] of ∼14 mM (-10-fold reduction). SPQ was loaded by 24 hours incubation in 20 mM of SPQ at 37°C. Images were acquired with a 4′,6′-diamino-2-phenylindole filter set on an inverted Nikon TE2000E microscope (20 X 0.5 NA PlanFluor objective). SPQ fluorescence was normalized to fluorescence at time 0 (F/F t = 0) as previously described. 17
Measurement of Airway Surface Liquid Height
Airway surface liquid (ASL) was labeled with 10 μL of Texas red dextran (10,000 MW; 2 mg/mL) in PBS followed by 48 hours incubation at 37°C in a humidified incubator to allow ALIs to absorb excess fluid and reach ASL homeostasis as previously described. 9 On removal from the incubator, cultures were immediately overlaid with 100 μL of perfluorocarbon (PFC-77) to prevent ASL evaporation. The apical side of the cultures was otherwise unmodified; drug additions were made basolaterally. Confocal images were taken using a 60 x (1.0 NA) water immersion objective with a 0.33-μm step size. Three slices (three regions each) were analyzed and averaged for each culture used.
Data Analysis and Statistics
Data were analyzed in SAVA, Fluoview and/or ImageJ. Statistical analyses were performed in Excel and/or GraphPad Prism (GraphPad Software, Inc., La Jolla, CA) with p < 0.05 considered statistically significant. For multiple comparisons with one-way ANOVA, Bonferroni posttest was used when preselected pairwise comparisons were performed, Tukey-Kramer posttest was used when all values in the data set were compared, and Dunnett's posttest was used when all values were compared with a control value.
Results
Ciliary Beat Frequency
Initial experiments focused on determining effects of Myrtol® on CBF. The sinonasal epithelium is composed of polarized cells with the apical surface exposed to the airways and the basolateral surface attached to a basement membrane and the adjacent epithelial cells. Typical nutrients are supplied to these cells via the basal surface from the vascular system. Thus, we interrogated whether there was differential effects based on the apical versus basolateral application of Myrtol®. As shown in Fig. 1, basolateral application resulted in a dramatic increase in CBF in a dose-dependent manner with a maximum stimulation at 30 minutes of 48 ± 7%.
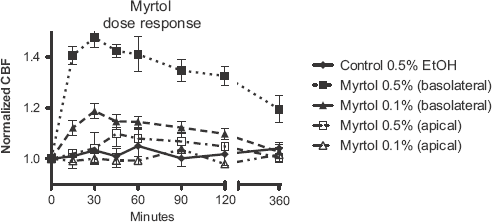
Myrtol® stimulates ciliary beat frequency (CBF). Basolateral versus apical application of Myrtol to well-differentiated human sinonasal air-liquid interface (ALI) cultures (n = 4 ALI cultures each from different patient per concentration). All points for 0.5% basolateral application were significantly elevated compared with vehicle. For 0.1% basolateral application only 15- to 120-minute time points were significantly elevated compared with vehicle.
Basolateral application yielded persistent elevation of CBF at 0.5% for at least 6 hours (p < 0.01 for all points tested) and at 0.1% for at least 2 hours (p < 0.05). Furthermore, at the higher concentration (0.5%), apical application trended to also increase CBF but with a longer onset of action (1 hour).
Because we had previously demonstrated that nonpolypoid CRS tissue (explant) had blunted ciliary responses to purinergic, adrenergic, and cholinergic stimulation,16,17 we wanted to make sure that ALI cultures derived from CRS patients did not show an altered ciliary response to basolateral application of Myrtol®. Thus, cultures derived from control and CRS without polyps patients were investigated. As expected from our prior studies showing reversibility of blunted ciliary responses in CRS, the cultures derived from the CRS patients demonstrated increases in CBF comparable with cultures derived from control patients (Fig. 2). That is to say, that the source of the material, CRS versus non-CRS did not affect the cilia function in mature ALI cultures.
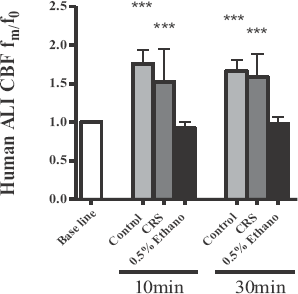
Control and chronic rhinosinusitis CRS) air—liquid interfaces (ALIs) increase ciliary beat frequency (CBF) with Myrtol. ALI cultures derived from CRS and control patients show comparable ciliary responses to Myrtol®. Mature ALI cultures (4–5 weeks) derived from the designated patients were stimulated with 0.5% Myrtol or 0.5% ethanol on the basolateral chamber and CBF quantified at 10 an 0 minutes (n = 3 ALIs from three patients in each category). Ethanol (0.5%) was used for control cultures. A t-test was performed against the control (***p < 0.05).
Mucociliary Transport Velocity
Recent work in rat trachea has established an increase in MCC at exceedingly small concentrations (0.01%). 5 Thus, we investigated the effects of basolateral application of Myrtol® on MCC as measured by fluorescent bead transport velocity.9,18 Although 0.1% Myrtol® had approximately a 20% increase in CBF, we found a significantly more robust effect at this concentration on MCC. As shown in Fig. 3, 0.1% Myrtol® applied to the basolateral surface of the human sinonasal ALI cultures yielded a 46% increase (±16%) in mucus transport velocity whereas dilution of Myrtol® to 0.05% had no demonstrable effects on mucus transport velocity.
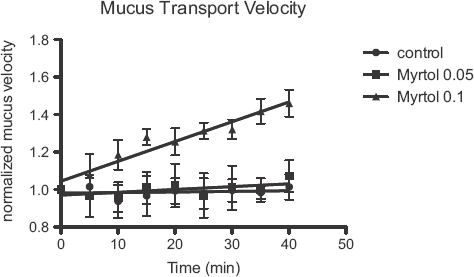
Myrtol® stimulates mucociliary clearance (MCC) velocity; 0.1% Myrtol® applied to the basolateral surface yielded a rapid and significant increase in MCC (n = 3).
Transepithelial Potential
Because the effects of Myrtol® on MCC were dramatically more effective than on CBF, we questioned whether Myrtol® may be altering the ASL viscosity via hydration. A rapid way in which to assess this possibility is with measurement of TEP. As shown in Fig. 4, 45 minutes after 0.5% Myrtol® basolateral application, the apical surface of the cells became significantly more negative. A potential explanation is either chloride efflux or sodium absorption. However, because MCC increased (Fig. 3), we assumed this was caused by efflux of Cl−resulting in a transepithelial voltage that draws sodium across the epithelium via paracellular pathways, with the resulting osmotic gradient drawing water both through paracellular and through transcellular (aquaporin) pathways. The other possibility, i.e., sodium absorption, would cause dehydration of mucus and result in decreased transport velocity.
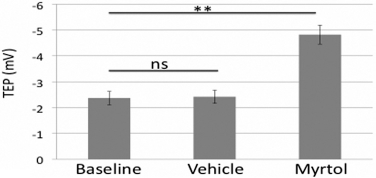
Myrtol® alters transepithelial potential (TEP). Basolateral application of Myrtol alters TEP driving the apical side more negative (baseline, 2.366 ± 0.261 mV; vehicle, 2.417 ± 0.255 mV; and Myrtol®, ±4.817 ± 0.366 mV; n = 3 per condition).
Apical Chloride Permeability
To confirm that mucociliary transport increased due to chloride efflux, we used the fluorescent dye SPQ. 9 In unstimulated sinonasal epithelial ALIs, replacement of apical chloride with nitrate did not result in any change in SPQ fluorescence, suggesting that resting apical chloride conductance is very low (Fig. 5 A). However, addition of Myrtol® to the basolateral chamber caused SPQ fluorescence to increase (0.10 ± 0.02 U/min; Fig. 5 B), suggesting that apical membrane anion permeability was activated. Addition of Myrtol to the apical surface had no effect (Fig. 5, D and E). To show that the SPQ was truly measuring chloride flux, we stimulated cystic fibrosis transmembrane conductance regulator (a cAMP driven chloride channel) with forskolin, which drastically increased SPQ fluorescence (Fig. 5 F). These results (summarized in Fig. 5 G) suggest that basolateral application of Myrtol stimulates fluid secretion by activating chloride flux.
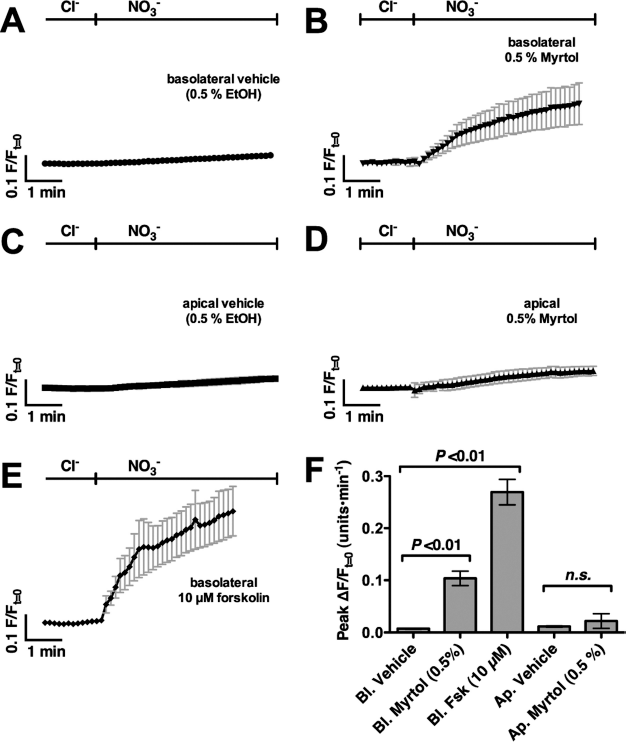
Myrtol stimulates chloride efflux. (A–D) Average traces of normalized SPQ fluorescence during (A and C) NO3− substitution with 0.5% ethanol or (B and D) 0.5% Myrtol. (E) Forskolin was used as a positive control. (F) Peak SPQ fluorescence (mean ± SEM) of raw traces from panels A–H (three ALIs each).
ASL Height
To confirm that the SPQ results reflected Myrtol activating epithelial fluid secretion, we directly measured sinonasal ALIs fluid secretion using techniques previously developed to measure ASL homeostasis. 19 ASL was stained with Texas red dextran before depth measurement via confocal imaging; a decrease in ASL height reflects a decrease in fluid volume whereas an increase in ASL height reflects an increase in fluid volume. Resting ASL height in human sinonasal ALIs was 11 ± 2 μm (Fig. 6 A). Cultures exposed to basolateral Myrtol exhibited significantly higher ASL after 45 minutes (24 ± 3 μm; Fig. 6 B). ASL heights are shown in Fig. 6 C.
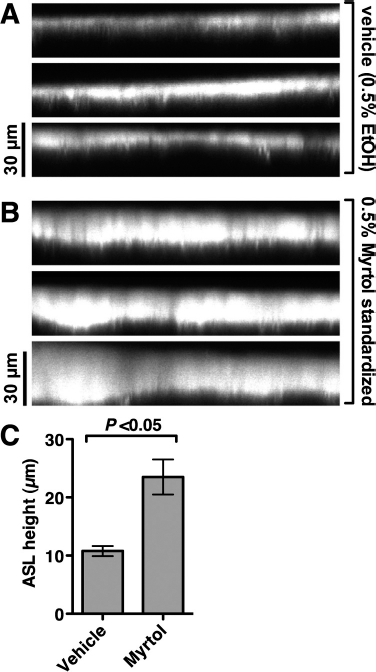
Myrtol activates fluid secretion in sinonasal epithelial cells. (A and B) Confocal Z-section images of Texas red dextran–labeled airway surface liquid (ASL) from (A) 0.5% ethanol and (B) Myrtol-stimulated (45 minutes) air–liquid interfaces (ALIs; n = 3 each). (C) Graph of mean ASL heights ± SEM.
Discussion
The ALI culture is a state-of-the-art epithelial model that has been used for extensive studies of the upper 20 and lower airways. 21 Importantly, this model maintains the polarity of the respiratory epithelium that is lost when cells are grown in submersion. Additionally, many physiological facets important in respiratory cell physiology can be analyzed in the ALI culture including CBF, mucus transport time, and transepithelial resistance, as well as electrolyte flux. Thus, this culture system is ideal for in vitro pharmacologic evaluation.
Myrtol is dosed at 300 mg/70 kg, which results in 4.1 μg/mL (serum) after calculating the bioavailability (95.6%) 7 ; however, the exact concentration in the respiratory epithelium is not known. In our in vitro studies we detected a 20% increase in CBF when 0.1% Myrtol (1 mg/mL) was applied to the basolateral surface of the cultures (Fig. 1), which is in agreement with prior studies. 5 However, using rat tracheal rings, Begrow et al. 5 showed modest but significant effects on CBF at Myrtol concentrations as low as 100 μg/mL, which we were not able to replicate (data not shown). This may be caused by differences in species or in cell preparation (ex vivo tracheal rings versus primary sinonasal cultures). Interestingly, in one study, human sinonasal explants grown in submersion showed no effects of Myrtol in concentrations lower than the therapeutic concentration (up to 300 ng/mL) on CBF. 4 In our studies, application of Myrtol to the apical surface of the cells, which may replicate cultures grown in submersion, did not indicate any significant effects on CBF (Fig. 1). However, in clinical settings the basolateral pathway is clinically more relevant, because it mirrors the hematogenic distribution of Myrtol; in these terms the apical application has merely ancillary value. This further accentuates the importance of maintaining polarity in studying epithelial cell physiology.
Mucus hydration is paramount for normal MCC. In addition to stimulating CBF we show in the human sinonasal ALI model that Myrtol is a potent stimulant of respiratory epithelial fluid secretion as evident by the increase in ASL height (Fig. 6). We further show that this hydration is most likely caused by chloride efflux (Fig. 5). However, the exact target of Myrtol is still unknown. As was evident in the CBF experiments, only basolateral application of Myrtol altered chloride permeability, suggesting that the target may be found on the basolateral membrane. It is important to note that the dual effect of Myrtol on fluid secretion and CBF yields a synergistic effect on mucociliary transport. Although 0.5% Myrtol yielded robust changes in CBF (Fig. 1) and ASL height (Fig. 6), 0.1% resulted in dramatic changes in mucus transport velocity (Fig. 3).
The majority of respiratory disorders involve airway inflammation, mucus hypersecretion, and mucostasis. Thus, fluid hydration with subsequent mobilization of inspissated and infected secretions is essential in managing most respiratory pathologies. The sequelae of too much fluid secretion in the upper airways would most likely only yield rhinorrhea. Thus, the combined effect of basolateral application of Myrtol on fluid hydration and stimulation of CBF explains the clinical efficacy of this oral phytomedicine.
Conclusions
From these experiments we conclude that Myrtol stimulates human sinonasal MCC by both acting as a cilia stimulant and a secretagogue. Additionally, Myrtol is not effective when applied apically (i.e., as a topical medication) but is highly effective when applied to the basolateral side of the ALI culture. The results of these experiments are consistent with the clinical observations that Myrtol aids in mobilizing respiratory secretions.