
Abstract
Background
Chitosan-dextran gel has been used as an antihemostatic agent and antiadhesive agent after endoscopic sinus surgery. Because Staphylococcus aureus biofilms have been implicated in recalcitrant chronic rhinosinusitis, this study aimed to further investigate the (i) anti-inflammatory, (ii) bacterial biofilm inhibition, (iii) antiproliferative effects, and (iv) wound-healing properties of chitosan and chitosan-dextran gel.
Methods
Fibroblasts were isolated from human nasal tissue and were used to determine the effects of chitosan and chitosan-dextran gel on (i) cell proliferation, (ii) wound healing, (iii) inflammation in fibroblast cultures challenged with superantigens S. aureus enterotoxin B (SEB) and toxic shock syndrome toxin (TSST), and (iv) on S. aureus biofilms.
Results
Chitosan was highly effective at reducing IL-8 expression after TSST and SEB challenge. Chitosan was also effective at reducing IL-8 expression of nonchallenged fibroblasts showing its anti-inflammatory effects on fibroblasts in a diseased state. Chitosan-dextran gel showed strong antibiofilm properties at 50% (v/v) concentration in vitro. Dextran, on its own, showed antibiofilm properties at 1.25% (w/v) concentration. Chitosan, on its own, reduced proliferation of fibroblasts to 82% of control proliferation and chitosan-dextran gel reduced proliferation of the fibroblasts to 0.04% of control proliferation. Relative to the no treatment controls, chitosan-dextran gel significantly delayed the wound-healing rate over the first 48 hours of the experiment.
Conclusion
Chitosan-dextran gel reduced fibroblast proliferation and wound-healing time, showing a possible mechanism of reducing adhesions in the postsurgical period. Chitosan reduced IL-8 levels, showing its anti-inflammatory properties. Chitosan-dextran gel and dextran treatment showed antibiofilm properties in our model.
In addition, its ability to dampen proinflammatory Th2 cytokine expression5,6 and its novel antimicrobial properties 7 have encouraged further investigation into its use in the treatment of bacterially stimulated chronic inflammatory diseases. As shown by Aziz et al., chitosan–dextran (Chitodex; University of Otago, New Zealand) hydrogel is efficacious against a broad range of Gram-positive and -negative pathogens, viz., Staphylococcus aureus, Streptococcus pyogenes, Escherichia coli, and Clostridium perfringens. 8
Chronic rhinosinusitis (CRS) patients who are unresponsive to medical intervention may require sinus surgery as their ultimate treatment option. They may present with nasal polyps (NPs) and/or eosinophilic mucus and highly edematous and inflamed sinonasal mucosa. A significant number of recalcitrant patients in this subgroup were found to have S. aureus–related biofilm adhering to their sinonasal mucosa. In addition, a significant proportion of these patients had a poorer postoperative outcome requiring multiple office visits and prolonged antibiotic and corticosteroid use. 9
Significant damage to the respiratory mucosa caused by chronic inflammation is attributed to the continued expression of TNF-α, IL-1α, IL-6, and interferon (IFN)-γ, cytokines that are normally secreted as part of the host defense mechanism against aeropathogens. This innate immune response is heightened by the presence of bacterial biofilms that trigger ongoing secretion of proinflammatory cytokines. IL-6 plays a significant role as a local inflammatory mediator in CRS. 10 Nasal fluid from 30 CRS with NP (CRSwNP) patients showed a positive correlation between expressed elevated IL-6 and eosinophilia in their NP tissue. Sachse et al. went further to report that intracellular S. aureus located in the epithelial layer of NPs could strongly induce IL-6 expression. 11
S. aureus enterotoxin B (SEB) has emerged as one of a suite of superantigens capable of triggering the release of proinflammatory cytokines from sinonasal tissue. 12 The potency of superantigens lies in their ability to cross-link MHC class II molecules expressed by antigen-presenting cells with the T-cell receptor β-chain variable region on lymphocyte surfaces to trigger T-cell activation.
Significant increases in IL-1β, TNF-α, IFN-γ, IL-2, IL-4, IL-5, IL-10, and IL-13 expression were elicited from NPs but not healthy inferior turbinate tissue challenged with SEB over a 24-hour period. A similar effect was observed when significantly higher IL-8 secretions were detected from asthmatic patients but not healthy derived epithelial cells after 24-hour SEB challenge. 13
IL-8 is a chemokine secreted by macrophages, fibroblasts, and endothelial cells. During the early inflammatory phase of pathogen invasion it recruits circulating neutrophils to the site of infection that degranulate to release lactoferrin. 14 In chronic respiratory conditions increased IL-8 levels during inflammation are correlated with elevated levels of three major antibacterial molecules, i.e., sIgA, lysozyme, and lactoferrin. 15
In the context of CRS with eosinophilia pathogenesis, IL-8 plays a significant role as an eosinophil chemoattractant. Erger and Casale 16 observed that eosinophils isolated from peripheral blood of allergic rhinitis patients were able to transmigrate across A549 (epithelial) and human umbilical vein endothelial cell coated Transwells with 8-μm-diameter pores in a time- and dose-dependent manner, toward the lower chambers spiked with IL-8. Its chemoattractant property was confirmed when the researchers were able to show that eosinophils did not migrate toward the lower wells when the upper Transwell chambers had higher IL-8 concentrations.
In this study we investigated the (i) anti-inflammatory, (ii) bacterial biofilm inhibition, (iii) antiproliferative effects, and (iv) wound-healing properties of chitosan, dextran, and CD hydrogel using an in vitro human fibroblast model.
Materials and Methods
Primary Fibroblast Cell Isolation
Sinonasal tissue was harvested from three CRSwNP patients at the time of surgery and immediately stored in DMEM (Invitrogen, Sydney Australia) and transported to the laboratory for fibroblast isolation and culture. Patients had given informed consent before the procedure. S. Paramasivan and D. Jones contributed equally to this work.
Tissue was washed twice in phosphate-buffered saline (PBS) containing penicillin at 500 U/mL and streptomycin and amphotericin B (Sigma-Aldrich, St. Louis, MO) at 0.5 mg/mL. The tissue was dissected into 1 x 1-mm2 pieces and incubated at 37°C 5% CO2 in 6-well plates for 2–4 weeks in DMEM containing penicillin at 500 U/mL and streptomycin and amphotericin B at 0.5 mg/mL. This tissue was used as the source of fibroblast and epithelial cell proliferation. Media were replaced every 48 hours during this time. The tissue fragments were removed when cells had grown to form a new confluent monolayer.
The mixed cell population was trypsinized, pelleted, and resuspended in PBS before pure fibroblast cell lines were isolated by immunomagnetic bead separation (Epithelial Enrich Dynabeads; Invitrogen) to remove the contaminating epithelial cells.
Cells that did not adhere to the Dynabeads were cultured and grown to near confluence and the epithelial cell subtraction process was repeated.
The almost 95% pure fibroblast population was confirmed by staining for a fibroblast-specific marker (prolyl 4-hydroxylase subunit antibody purchased from Chemicon, Melbourne Australia).
Alamar Blue Fibroblast Proliferation Assay
Fibroblasts were seeded at a density of 2 x 10 4 cells/well in 96-well plates (Nunc, Sydney Australia) and cultured at 37°C 5% CO2 for 24 hours.
Media was aspirated and the following were added to the cells:
No treatment control (NTC)–Airway Media (Sigma-Aldrich, St. Louis, MO).
Five percent chitosan.
Three percent dextran.
Chitodex hydrogel (two aforementioned products combined to form a gel).
Using the same protocol, a separate 96-well plate without fibroblasts was run as the negative control.
Readings were taken at 4, 24, 48, 72, and 96 hours; for each time point reading media was removed and fresh media containing 10% Alamar Blue (Invitrogen) was added.
After a 4-hour appropriate incubation time at 37°C, the plate was read at 570 and 595 nm according to the manufacturer's instructions.
Fibroblast Wound-Healing Protocol
Fibroblasts were seeded at a density of 1 x 10 5 cells/mL in 12-well plates (Nunc) and allowed to grow to confluence. Media was aspirated and three uniform wounds of 2-mm diameter using a punch biopsy were created in each well. Wells were washed with PBS to remove any cells still attached to the wound edge and the wound area was examined by microscopy to ensure a clear area had been created.
Treatments in four replicates were as follows:
NTC–Airway Media only.
Chitodex hydrogel was placed within the wound area and allowed to set (∼1 minute) before adding Airway Media to each well. Media were replaced every 48 hours.
Reduction in wound areas were digitally recorded every 24 hours for 10 days (Nikon Eclipse TE 2000-V; Nikon, Tokyo, Japan) and calculated using the software provided (Nis Elements [Basic Research] 3.00, Nikon, Tokyo, Japan).
S. aureus Enterotoxin Challenge and Chitosan Modulation
Fibroblasts were seeded at a density of 2 x 10 5 cells/well in 24-well plates (Nunc) and grown at 37°C 5% CO2 in airway medium with the constituents per liter as follows:
DMEM 1:1 nutrient mixture F12 HAM (15.6 g), sodium bicarbonate (1.1 g), ITS liquid media supplement 100 x (3 mL), bovine pituitary extract (25 mg), sodium pyruvate (0.11 g), retinoic acid (2 x 10−8 moles), endothelial cell growth supplement (15 mg), hydrocortisone (2.5 μg), epidermal growth factor (10 μg), and 5% fetal calf serum. All media constituents were purchased from Sigma-Aldrich except bovine pituitary extract (Invitrogen, Carlsbad, CA).
After 24 hours media were removed, cells were washed twice with PBS, and the cells were treated as follows:
Four sets of triplicate wells containing Airway Media as NTCs.
Four sets of triplicate wells in Airway Media were primed with IFN-γ at 10 ng/mL (R&D Systems, Minneapolis, MN) at 37°C 5% CO2 for 24 hours.
Media were removed and cells were washed twice with PBS.
Each of the four sets of triplicate wells (either primed with IFN-γ or not primed) were then treated as follows:
NTC–Airway Media only.
Fifty microliters of 5% chitosan (University of Otago, New Zealand) + Airway Media.
SEB or toxic shock syndrome toxin (TSST) at 1 μg/mL in Airway Media.
SEB or TSST at 1 μg/mL in Airway Media and 50 μL of 5% chitosan.
After a 24-hour incubation, conditioned media were collected and stored at -80°C for cytokine profile analysis. Experiments were repeated on two separate occasions. Cells were trypsinized, pelleted, and stored in RNA later (Ambion Inc., Austin, TX) at -80°C.
Cytokine Expression Assay
Conditioned media were centrifuged at 15,600 x g (5415R; Eppendorf, Hauppauge, NY) to remove any precipitate and were adjusted to a concentration of 100 μg of total protein before analysis. Each treatment was analyzed in duplicate using the Human Cytokine 8 plex Panel (Bio-Rad Laboratories, Hercules, CA) according to the manufacturer's instructions. The cytokines in this panel were IL-2, IL-4, IL- 6, IL-8, IL-10, IFN-γ, granulocyte macrophage colony-stimulating factor, and TNF-α.
In Vitro Bacterial Biofilm Inhibition Assay
Bacterial Strains
Three clinical isolates of S. aureus obtained from patients with severe CRS as well as reference strain American Type Culture Collection (ATCC 25923; Manassas, VA), a known biofilm former, were used for this aspect of the study. Clinical isolates were obtained from the nasal passages of patients undergoing functional endoscopic sinus surgery in a tertiary hospital setting within the previous 2 years. The biofilm-forming capacity of these strains were confirmed previously by confocal scanning laser microscopy examination and isolates then stored at -80°C in 80% glycerol.
The clinical characteristics of the three CRS patients from whom clinical isolates were obtained are represented in Table 1.
Characteristics of CRS of clinical patients
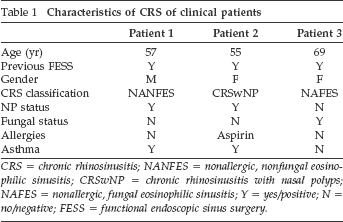
CRS = chronic rhinosinusitis; NANFES = nonallergic, nonfungal eosinophilic sinusitis; CRSwNP = chronic rhinosinusitis with nasal polyps; NAFES = nonallergic, fungal eosinophilic sinusitis; Y = yes/positive; N = no/negative; FESS = functional endoscopic sinus surgery.
Biofilms were grown and the antibiofilm-forming effects of chitosan, dextran, and Chitodex gel were tested using a modified version of the Calgary Biofilm Device Model. 17 Briefly, the steps are outlined in the following sections.
Biofilm Formation
Glycerol stock cultures were defrosted in 2 mL of cerebrospinal fluid (CSF) broth (Oxoid, Adelaide, Australia) overnight before being transferred onto Columbian horse blood agar plates (Oxoid). The plates were incubated at 37°C for 24 hours, at which point 1–2 single colony-forming units were inoculated in 2 mL of 0.45% saline to make up a 1 McFarland standard solution; 0.4 mL of this was added to 5.6 mL of CSF to make up 6 mL of bacterial solution. A sterile pegged 96-well plate (Innovotech, Calgary, Canada) was used as the reservoir for biofilm growth. The central wells of the plate were seeded with 150 μL of bacterial solution. Wells on the periphery were filled with 250 μL of PBS to reduce evaporation during the incubating process. The pegged lid was then placed onto the seeded wells, and the plate was incubated for 30 hours at 37°C. The plate was mounted on a gyro-rotator platform (Ratek, Melbourne, Australia) revolving at 70 rpm to provide shear stresses and encourage biofilm formation on immersed pegs.
Antibacterial Exposure
After 30 hours of biofilm growth, pegged lids were immersed into challenge plates consisting of either chitosan only, dextran only, or combined Chitodex gel. All solutions were prepared immediately before use.
Stock solutions of chitosan (5%) was serially diluted (ratio of 1:2) in CSF broth to provide adequate nutrients for potential biofilm growth. Three hundred fifty milligrams mg of dextran aldehyde was dissolved into 10 mL of buffer solution to produce stock solutions (3.5% w/v) that are subsequently diluted in CSF as per chitosan. Chitodex gel is formed by the combination of stock chitosan and dextran. The gel was serially diluted in CSF promptly, before setting of the gel.
To form the challenge plates, fresh 96-well plates (Nunc) were seeded with 200 μL of serially diluted chitosan, dextran, or Chitodex gel. Chitosan was tested at 2.5, 1.25, 0.625, 0.313, or 0.156% concentration Dextran concentrations used were 1.75, 0.875, 0.438, 0.219, or 0.109%. Chitodex gel (made up of chitosan 5% and dextran 3.5%) was tested at concentrations of 50, 25, 12.5, or 6.25%. Neat solutions of chitosan, dextran, and Chitodex with no CSF dilution were not tested as the thickness of the gel precludes the use of culture medium and therefore the nutrients for adequate biofilm growth would be unavailable. Challenge plates consisting of CSF alone served as negative controls.
The pegged lid from the 30-hour incubated plate was removed, washed with sterile PBS for 1 minute, and replaced within one of the challenge plates. These fresh plates were incubated for 24 hours at 37°C on the gyro-rotary platform.
Sonication and Analysis
After 24-hour exposure to the challenge plates, the pegged lids were removed, washed with PBS for 1 minute, and then placed in a new 96-well plate containing 150 μL of CSF. This plate was placed in a sonication bath for 5 minutes to ensure any biofilms attached to the pegs were dislodged into the CSF broth. After sonication, the pegged lids were carefully removed and discarded. This lid was replaced with a standard plate lid. These plates were then incubated for an additional 24 hours at 37°C, without the use of a rotator to allow any surviving bacteria to divide and multiply.
Turbidity reflected bacterial growth within the wells and hence there was no antibiofilm effect. To quantify this assessment, the plates were also read using a microplate spectrophotometer (Bio-Rad Laboratories) at 595 nm. Optical densities of <0.01 represented minimal turbidity and hence measurable antibiofilm activity.
Statistical Analysis
All statistical analyses were performed using GraphPad Prism, Version 5.04 (GraphPad Software, San Diego, CA). A one-way comparison of variance was used across all concentrations with Bonferroni adjustment at a value of p < 0.05 significance level. The mean was considered when comparing results. The experiments were repeated on two separate occasions.
Results
Anti-Inflammatory Effects of Chitosan
IL-8 Expression
Fibroblasts were preprimed with IFN-γ (10 ng/mL) for 24 hours to stimulate MHC class II molecule expression before enterotoxin challenge. We did not detect any significant increase in IL-8 response in the preprimed fibroblast when compared with untreated cells.
TSST-1 Challenge
The fibroblasts derived from sinonasal tissue harvested from three patients were subjected to the treatment schedule as detailed in the Materials and Methods sections. Experiments were repeated on two separate occasions and data were pooled for statistical analyses.
Chitosan was highly effective in significantly reducing IL-8 expression (mean ± SD pg/mL): IFN-γ + TSST-1 (799.7 ± 284.2) versus IFN-γ + TSST-1 + chitosan (371.6 ± 104.2) (p < 0.001). The use of chitosan on its own was also effective in lowering IL-8 on fibroblasts even without IFN-γ priming or TSST-1 stimulation, which reflects the already inflamed state of tissue from CRSwNP patients as already sensitive to enterotoxins: control (698.1 ± 240.3) versus chitosan (358.6 ± 198.5) (p < 0.01; Fig. 1).
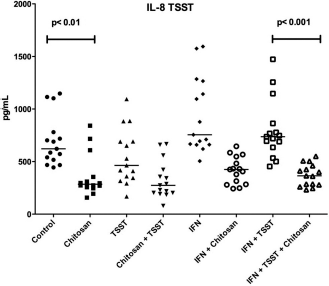
IL 8 expression in fibroblasts exposed to toxic shock syndrome toxin (TSST) and in fibroblasts with prior priming with interferon (IFN) γ.
SEB Challenge
Similarly, a reduction in IL-8 (mean ± SD pg/mL) was also detected after a 24-hour SEB challenge:IFN-γ + SEB (2536 ± 1592) versus IFN-γ + SEB + chitosan (1229 ± 552.7) (p < 0.05). Although the application of chitosan on its own reduced IL-8 levels, its effect was not statistically significant: control (1691 ± 1178) versus chitosan (946 ± 700.1) (Fig. 2).
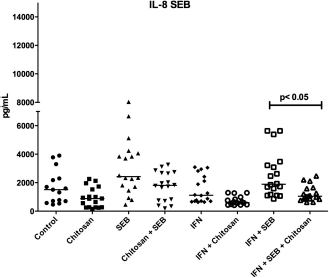
IL-8 expression in fibroblasts exposed to Staphylococcus aureus enterotoxin B (SEB) and in fibroblasts with prior priming with interferon (IFN) γ.
Expression of other Cytokines
We did not observe any ameliorating effect of chitosan on the expression of the other cytokines tested (data not shown).
Anti–S. aureus Biofilm Activity
The effect of chitosan, dextran, and Chitodex hydrogel as inhibitors of bacterial biofilm was tested on S. aureus clinical isolates from three CRS biofilm-positive patients and a known S. aureus biofilm-forming reference strain ATCC 25923.
Chitosan alone had no significant effect as an antibiofilm agent on the clinical isolates (Table 2). Chitodex hydrogel at 50% (v/v) showed significant antibiofilm activity in vitro. Dextran (at >0.875% w/v) accounted for all of the observed antibiofilm activity of the gel. Lower concentrations of dextran did not inhibit biofilm formation.
Antibiofilm activity of chitosan, dextran, and Chitodex gel
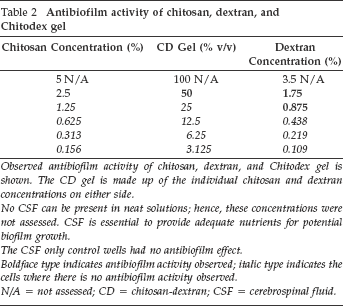
Observed antibiofilm activity of chitosan, dextran, and Chitodex is shown. The CD gel is made up of the individual chitosan and dextran concentrations on either side.
No CSF can be present in neat solutions; hence, these concentrations were not assessed. CSF is essential to provide adequate nutrients for potential biofilm growth.
The CSF only control wells had no antibiofilm effect.
Boldface type indicates an film activity observed; italic type indicates the cells where there is no antibiofilm activity observed.
N/A = not assessed; CD = chitosan-dextran; CSF = cerebrospinal fluid.
AntiProliferative Effects
We measured fibroblast proliferation using Alamar Blue reduction assay where the amount of dye reduced is proportional to the number of and, hence, viability of cells. Chitosan alone was able to reduce fibroblast proliferation and viability (82% reduction in Alamar Blue) when compared with NTCs (p < 0.0001). This was evident within the first 24 hours of treatment (Fig. 3).
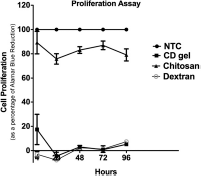
Fibroblast proliferation as a percentage of Alamar Blue reduction.
However, we found dextran to be extremely effective, reducing fibroblasts to <0.04% (p < 0.0001); its potency remained unaffected when used in combination with chitosan as the Chitodex gel mix (reduced to <4.4%; p < 0.0001).
Wound-Healing Properties
Relative to NTCs, Chitodex gel (3 μL) significantly delayed the wound-healing rate within the first 24 (day 1; p < 0.05) and 48 hours (day 2; p < 0.001; Fig. 4).

Chitodex gel effect on wound closure.
Similarly, Chitodex gel (5 μL) also showed the same pattern of delaying wound healing on day 1 (p < 0.05) and day 2 (p < 0.001). No significant differences were detected in wound healing of either the 3 and 5 μL volumes of Chitodex hydrogel.
Discussion
Chitodex hydrogel has been widely used in sinus surgery both as an antihemostatic and as an antiadhesive agent. However, the anti-inflammatory, wound healing, antiproliferative, and antibiofilm effects of Chitodex and its individual components dextran and chitosan have not been tested using a common human sinus fibroblast model until now.
Our results indicated that chitosan, dextran, and Chitodex hydrogel has partial mitigating effects on the superantigen-driven immune response by acting as anti-IL-8, anti-inflammatory, and antiproliferative agents on human fibroblasts. Also, its antibiofilm activity on known biofilm-forming S. aureus clinical isolates positions the use of Chitodex as a treatment modality for S. aureus–associated CRS in the postoperative setting. As an antiadhesive, Chitodex delayed wound healing by 24 hours as measured by the rate of fibroblast migration required for a 50% wound recovery.
SEB is a potent stimulator of Th2 proinflammatory cytokines such as IL-1β, TNF-α, IFN-γ, IL-2, IL-4, IL-5, IL-10, and IL-13 in NPs derived but not healthy inferior turbinate tissue 12 and IL-8 in THP-1 cell lines, 18 respectively. Our results indicated that SEB was able to elicit IL-8 expression from fibroblasts derived from our CRSwNP patients. We showed that chitosan significantly dampened the level of IL-8 cytokine release in fibroblasts after SEB and TSST-1 enterotoxin challenge. In a clinical context, the delivery of chitosan in Chitodex hydrogel form to the diseased sinonasal mucosa may potentially reduce leukocyte migration and degranulation normally associated with chronic mucosal inflammation. 16
It is now understood that fibroblasts (in addition to dendritic cells) behave as nonprofessional antigen-presenting cells during a host pathogen immune reaction. Chitosan exhibited an antiproliferative effect by reducing fibroblast growth by 20% relative to NTCs, with dextran and Chitodex hydrogel reduces fibroblasts by almost 100% relative to NTCs. Dextran and Chitodex gel effectively stopped all proliferation within 4 hours of treatment with any renewed cell growth and was almost negligible for the duration of the assay (96 hours).
Fibroblasts are a major producer of extracellular matrix during wound healing, which is a major contributor in adhesion formation. 19 The antiproliferative and wound repair properties displayed by chitosan may suggest one possible mechanism to the observed reduction in adhesion formation clinically.
Complete eradication of biofilm-causing bacteria after sinus surgery remains a challenge despite current treatment regimes. 9 Therefore, by targeting the remnant biofilm communities from recolonizing the mucosal surface, an insidious source for reinfection can be neutralized.
Our observations that Chitodex gel (50% v/v) expressed strong antibiofilm activity further complemented a recent work by Aziz et al. on the bactericidal activity of Chitodex against Gram-positive pathogens such as aureus and S. pyogenes. 8 Similarly, we found that dextran and not chitosan was the active component in the observed antibiofilm activity of the gel. Although our study did not examine its antisurface adhesion property, Busscher reported that pretreatment of glass slides with chitosan reduced the adherence of Streptococcus mutans and Streptococcus oralis, two common oral bacteria, after 2-hour exposure. 20
The variability of responses by biofilm-positive CRSwNP patients to medical and surgical intervention has resulted in the investigation of novel treatment to manage this recalcitrant patient group. We have shown that Chitodex gel has properties beyond that of an antiadhesive having both anti-inflammatory and antibiofilm properties, which may benefit the patient in the postoperative period. Future studies are required to fully delineate the mechanism of action of Chitodex gel as well as its potential clinical applications.