
Abstract
Background
There may be substantial variation in paranasal sinus pneumatization across patients and between right and left sides. Patients with extensive sinus aeration, especially of the sphenoid sinus and along the skull base, often have protrusion of critical structures into the pneumatized sinus cavities, which potentially places these structures at risk during sinus surgery.
Objective
To evaluate associations between anatomic markers of increased paranasal sinus aeration along the skull base and to determine whether the presence of certain markers predicts other critical anatomic variants.
Methods
Submillimeter axial computed tomography (CT) scans and associated triplanar reconstructions from 100 subjects were reviewed for the presence of 22 anatomic variants by two separate evaluators. Twelve of these variants were selected as markers of increased pneumatization. Average numbers of markers were compared with t-tests; associations between markers were evaluated by logistic regression analyses. The Holm-Bonferroni method was used to correct for multiple tests.
Results
Five anatomic variants were associated with increased paranasal sinus pneumatization as define by total number of markers of pneumatization: anterior ethmoid artery below the skull base, dehiscent/protruding internal carotid artery (ICA), dehiscent/protruding optic nerve (ON), pneumatized pterygoid recess, and middle turbinate (MT) concha bullosa (all p < .02). Significant associations were found between pneumatized pterygoid recesses and dehiscent or protruding ONs (odds ratio [OR] 3.06, p = .0120), dehiscent or protruding ICAs (OR 6.64, p < .0001), and anterior ethmoid arteries below the skull base (OR 2.65, p = .0189). Significant association was also found between dehiscent or protruding ONs and dehiscent or protruding ICAs (OR 3.57, p = .0047).
Conclusion
The markers of increased pneumatization and anatomic associations identified is study have important implications for surgeons planning and undertaking operative approaches in and around the sinuses.
Although substantial data exists outlining the prevalence of variant sinus anatomy in various populations,2,8–37 few studies have evaluated correlations between or among them. In a small study of 47 children with chronic sinusitis, Sivasli et al demonstrated weak associations between presence of agger nasi cells and pneumatization of superior turbinate (ST) and MT, presence of large ethmoid bulla and pneumatized ST and secondary MT, and presence of Haller (infraorbital ethmoid) cell and pneumatization of ST. 12
This study aims to determine correlations among paranasal sinus anatomic variations in adults. Special attention is paid to markers of increased aeration and pneumatization along the ethmoid roof, sphenoid sinus, and skull base that either expose or lie in close proximity to vital structures along the paranasal sinus bony walls.
Methods
The medical records of all patients presenting to a single rhinologist (S.K.W.) at the Emory University Sinus, Nasal and Allergy Center in Atlanta, GA, from January 2011 to February 2013 were reviewed. Patients who had a CT scan of the paranasal sinuses in submillimeter axial slices with triplanar reconstructions obtained at an Emory University radiology facility were retained in the initial dataset. Subjects with radiologic evidence of trauma, prior sinus surgery, nasal polyposis, tumor distorting sinus anatomy, or greater than minimal sinus mucosal disease were excluded. The target dataset was 100 subjects based on estimated prevalence of key anatomic variants including Onodi cell and pneumatized MT.
Two separate evaluators reviewed each sinus CT scan for the presence of anatomic variants along the skull base (aerated crista galli, gross ethmoid roof asymmetry, and cephalocele), ethmoid region (agger nasi cell, Haller cell, pneumatized uncinate process, presence of middle ethmoid artery, and any ethmoid artery in a mesentery below the skull base), sphenoid sinus (Onodi cell, dehiscent or protruding ON, dehiscent or protruding ICA, pneumatized pterygoid recess, and sphenoid dominance), turbinates (pneumatized MT, ST, or other turbinate; paradoxically curved turbinate), and nasal septum. Variants were classified as “absent” or “present,” except for sphenoid dominance and nasal septal deviation, which were classified as “left” or “right.” Dehiscence was defined as absence of bony margin over part or all of the nerve or artery. Protrusion was defined as extension of greater than 50% of the circumference of the nerve or artery into the air space with or without intact bony covering.23,24 These criteria are illustrated in Fig. 1.
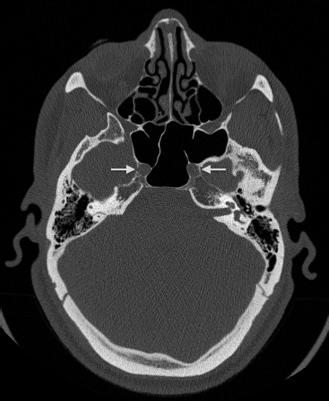
Dehiscent and protruding internal carotid arteries. Axial CT scan in bone algorithm demonstrating bilateral dehiscent and protruding internal carotid arteries (arrows). Dehiscence is defined as absence of bony margin and protrusion is defined as extension of greater than 50% of circumference of artery into sphenoid air space.
Twelve of the 22 anatomic variants were selected as markers of increased pneumatization: Onodi cell, Haller cell, dehiscent or protruding ON, dehiscent or protruding ICA, anterior or posterior ethmoid artery below the skull base, pneumatized pterygoid recess, aerated crista galli, pneumatized uncinate process, pneumatized MT, ST, or other turbinate. Examples of these markers are illustrated in Figs. 2–4. Student t-tests were applied to evaluate individual markers as predictors of overall pneumatization with the Holm-Bonferroni correction for multiple tests. Logistic regression analyses were used to evaluate associations between markers with frequency greater than 10%. All analyses were performed with SAS version 9.3. Significance level was set at 0.05. The Institutional Review Board of Emory University approved the protocol for this study (IRB00058752).
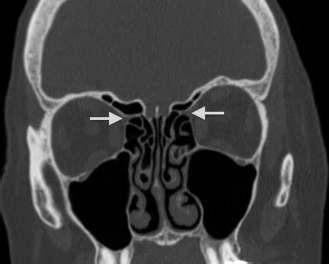
Anterior ethmoidal arteries below the skull base. Coronal CT scan in bone algorithm demonstrating bilateral anterior ethmoidal arteries in bony mesentery below the skull base (arrows).
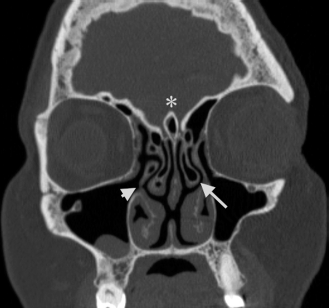
Aerated crista galli, pneumatized uncinate process, and concha bullosa of the middle turbinate. Coronal CT scan in bone algorithm demonstrating an aerated crista galli (asterisk), pneumatized uncinate process (short arrow) and concha bullosa of the middle turbinate (long arrow).
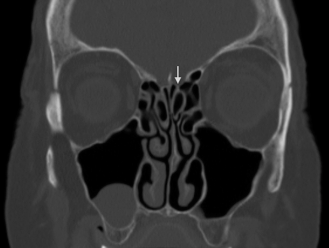
Concha bullosa of the superior turbinate. Coronal CT in bone algorithm demonstrating bilateral concha bullosa of the superior turbinate (arrow).
Results
One-hundred paranasal sinus CT scans (200 sides) were included for analysis. Mean age of the subjects at time of scan was 52.5 years with a SD of 15.8 years; 31 subjects were male and 69 were female. Frequency of the 22 anatomic variants is presented in Table 1. The mean number of markers of increased pneumatization was 5.3 with total number of markers ranging from 0 to 15. The percent of subjects with each total number of markers of pneumatization is presented in Fig. 5.
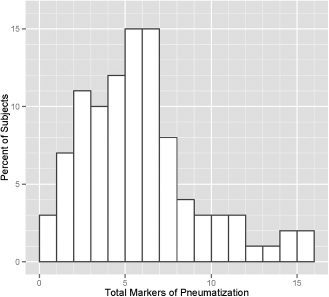
Distribution of markers of increased pneumatization. The mean markers of increased pneumatization was 5.3 with standard deviation of 3.4. 97% of subjects had at least one marker of pneumatization, and 90% had multiple markers.
Frequency of anatomic variants of paranasal sinuses (%)
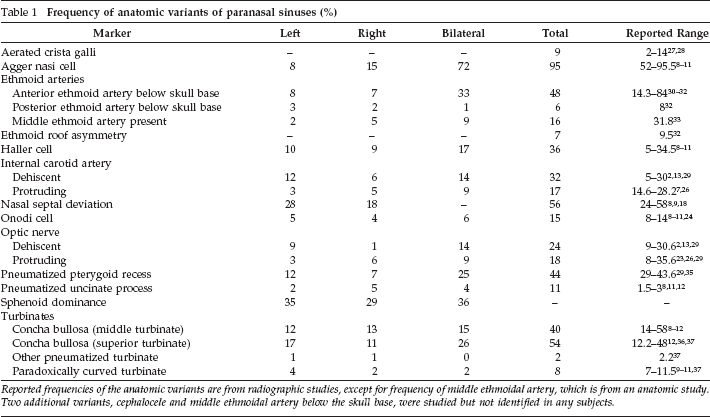
Reported frequencies of the anatomic variants are from radiographic studies, except for frequency of middle ethmoidal artery, which is from an anatomic study. Two additional variants, cephalocele and middle ethmoidal artery below the skull base, were studied but not identified in any subjects.
Five anatomic variants were associated with increased paranasal sinus pneumatization, as defined by total number of markers of pneumatization: anterior ethmoid artery below the skull base (p = .0012), dehiscent/protruding ICA (p = .0012), dehiscent/protruding ON (p = .0012), pneumatized pterygoid recess (p = .0012), and MT concha bullosa (p = .0120) (Table 2). Of these, a dehiscent or protruding ICA was associated with the greatest overall markers of pneumatization. Subjects with this variant had an average of 7.64 markers of increased pneumatization, whereas subjects without this variant had an average of 4.04 markers of increased pneumatization.
Specific markers as predictors of increased aeration
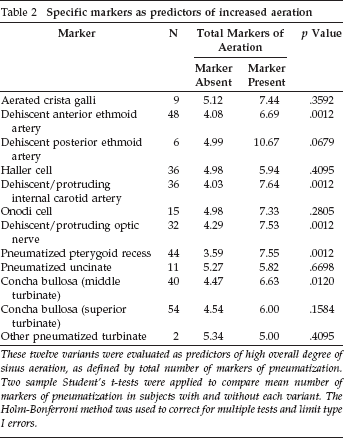
These twelve variants were evaluated as predictors of high overall degree of sinus aeration, as defined by total number of markers of pneumatization. Two sample Student's t-tests were applied to compare mean number of markers of pneumatization in subjects with and without each variant. The Holm-Bonferroni method was used to correct for multiple tests and limit type I errors.
Logistic regression analyses were performed to examine associations between nine variants with frequency greater than 10%. Significant associations were found between pneumatized pterygoid recess and dehiscent or protruding ON (odds ratio [OR] 3.06; p = .0120), dehiscent or protruding ICA (OR 6.64; p < .0001), and anterior ethmoid artery below the skull base (OR 2.65; p = .0189). An additional association was found between dehiscent or protruding ON and dehiscent or protruding ICA (OR 3.57; p = .0047) (Table 3). The association between pneumatized pterygoid recess and protruding ON is illustrated in Fig. 6.

Pneumatized pterygoid recesses and protruding optic nerves. Coronal CT in bone algorithm demonstrating bilateral protruding optic nerves (arrows) and pneumatized pterygoid recesses (asterisks). These variants were significantly associated.
Associations between markers of increased pneumatization
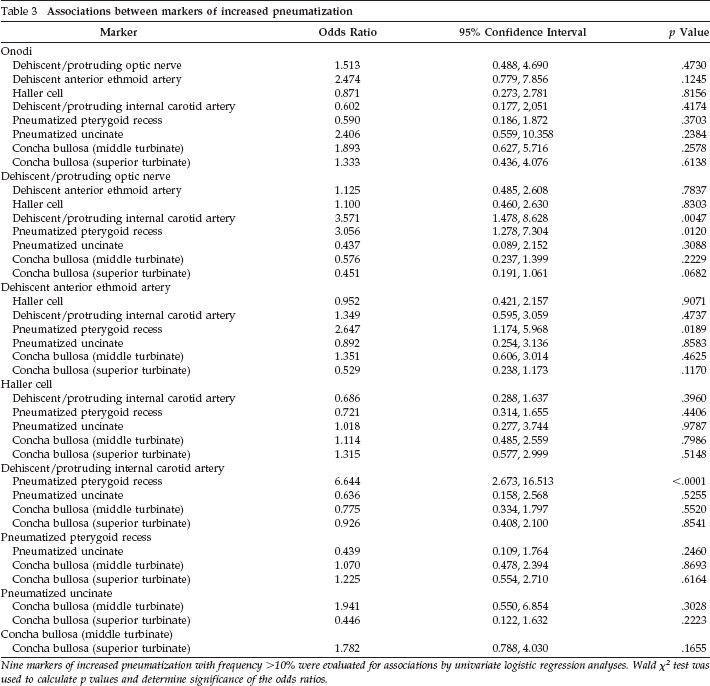
Nine markers of increased pneumatization with frequency >10% were evaluated for associations by univariate logistic regression analyses. Wald χ 2 test was used to calculate p values and determine significance of the odds ratios.
Discussion
The frequency of anatomic variants in this study is largely consistent with values reported in the literature (Table 1). Our results differ from previous reports with respect to two variants: middle ethmoidal artery and pneumatized uncinate process. In a cadaveric study of 22 adult specimens, Wang et al identified a middle ethmoidal artery in 31.8% of subjects. 33 We only noted this variant in 16% of subjects. However, this discrepancy may be due to differing identification methods, anatomic in the Wang study and radiographic in our study. Frequency of pneumatized uncinate process has been reported as 1.5–3%.8,11,12 However, we identified this variant in 11% of subjects. It is difficult to comment on whether our results deviate from the norm, because there is little published data on the prevalence of middle ethmoidal artery or pneumatized uncinate process.
We identified several anatomic variants that were significantly associated with increased overall pneumatization; many of these variants are also surgically significant. An anterior ethmoid artery suspended within a bony mesentery may be at risk during ethmoidectomy or endoscopic anterior skull base approaches. Injury to the lateral portion of this artery results in local hemorrhage, whereas injury to the medial portion may cause a subdural hematoma. 2
Dehiscence or protrusion of the ICA into the sphenoid cavity exposes the structure to surgical trauma during sphenoidotomy or endoscopic sella/clivus approaches, which can result in catastrophic hemorrhage and cerebral injury. Immediate control of bleeding is difficult due to limited exposure with the standard endoscopic endonasal approach. ON damage is another risk of operations involving the sphenoid sinus. This risk is greatly increased when the ON is dehiscent or protruding into sphenoid air space. 25 Traumatic injury to the ON can result in immediate or delayed blindness.
Of note, 97% of subjects in this study had at least one marker of increased pneumatization, and 90% had multiple markers. Figs. 1–4 and 6 illustrate examples of multiple markers of aeration in the same subject. Perez-Pinas et al have also observed this phenomenon of multiple anatomic variants in one subject in a study of 110 adults. 18 This observation is supported by our finding of significant associations between multiple markers of increased pneumatization.
The associations between pneumatized pterygoid recess, dehiscent or protruding ON, and dehiscent or protruding ICA are plausible and logical, because they are all markers of a highly pneumatized sphenoid. The association between pneumatized pterygoid recess and anterior ethmoid artery in a mesentery below the skull base is less easily explained, because these variants arise from spatially and anatomically segregated regions.
We anticipate that the associations identified in this study will inform preoperative assessment of sinus CTs, particularly for trainees and new practitioners. Anatomic landmarks can frequently be difficult to identify on CT due to mucosal disease or previous surgery. Even under these circumstances, a pneumatized pterygoid recess is fairly easily identifiable, and it can be used as an indicator for associated variants. The presence of a pneumatized pterygoid recess should prompt the sinus surgeon to closely evaluate the ON, ICA, and anterior ethmoidal artery for the risky variants described in this study.
Conclusion
When operating near so many vital structures, the best management of any potential complication is prevention. It is essential for the sinus surgeon to understand not only “standard” anatomy but also the possible variants described in this study. With modern imaging modalities, anatomic variations can be detected, and potential pitfalls can be anticipated. It is our hope that the associations identified in this study will aid in preoperative planning for trainees as well as more experienced sinus surgeons.
Footnotes
Acknowledgments
We thank Azhar Nizham, MS for biostatistical consultation.