
Abstract
Background
Radiation therapy is a cornerstone in nasopharyngeal cancer treatment. However, it can induce acute and long-term adverse effects, such as acute mucositis and late submucosal fibrosis. Late toxicities could not only affect submucosa but also mucosal cells, determining long-term cytological changes.
Objective
Evaluation of delayed nasal cytological alterations in patients who underwent radiation therapy for nasopharyngeal carcinoma (NPC).
Methods
In this case-control study, we analyzed 30 healthy subjects and 30 patients treated with chemotherapy and radiotherapy for NPC between 2003 and 2011, with a median follow-up of 59 months. All subjects underwent symptoms anamnestic evaluation (rhinorrea, nasal obstruction), endoscopic fiber optic nasal examination, skin-prick tests, and nasal scraping for cytological exam.
Results
A higher percentage of rhinorrhea, nasal obstruction, mucosal hyperemia, and presence of nasopharyngeal secretions at fiber optic endoscopic exam was found in radiated subjects (p < 0.05). Nasal cytology analysis demonstrated a higher percentage of neutrophilic inflammation and squamous cell metaplasia and mucous cell metaplasia in treated patients (p < 0.05). No cytological atypia was seen. No statistically significant correlation between nasal cytological changes and objective findings, patients' age, tobacco smoking, and gastroesophageal reflux has been found in the radiotherapy group (p > 0.05).
Conclusion
Radiation therapy induces late nasal mucosal changes, which may be related to clinical consequences, such as abundant mucus production and its consequent endonasal stagnation. In the future, detailed knowledge of cytological changes in patients' nasal mucosa could represent a key prerequisite for the choice of effective interventions for late radiation-induced rhinitis.
Radiation therapy represents standard of care for NPC in early and late stages, alone or in association with chemotherapy.
Irradiation fields for NPC involve nasal and oral mucous membranes and submucosa, inducing acute and long-term adverse effects, such as acute mucositis and late submucosal fibrosis.3–6 However, late toxicities could not only affect submucosa but also mucosal cells, determining long-term cytological changes.
These effects mainly involve rapidly renewing cells, both neoplastic and healthy tissue stem cell. In the head and neck region mucosal proliferating cells are the more susceptible to radiation-induced mitotic deaths.
Decrease in oral epithelial cell density, cytological atypia, inflammatory infiltrate, and viral cytopathic effects are reported during chemotherapy and/or radiotherapy7,8, but details of radiation effects on mucosa have not been studied as intensively as for skin and subcutaneous vasculoconnective tissue.
Aim of this case-control study is the evaluation of delayed nasal cytological alterations in patients who underwent radiation therapy for NPC.
Materials and Methods
Between 2003 and 2011, 30 healthy subjects and 30 patients treated with chemo-radiation therapy for NPC at our Department were enrolled in this retrospective case-control study. Each patient underwent neoadjuvant, concomitant and/or adjuvant chemotherapy associated with radiotherapy and had a minimum follow-up of two years to evaluate stabilized late effects. All patients included in the study were disease free at the time of enrollment, and they had no clinically evident viral and/or bacterial diseases involving nasal cavities. Healthy subjects were patients with vocal fold nodules or polyps and without any clinical and endoscopic sign of sinonasal disease. Written informed consent was obtained in every case. Approvals of the Ethics Committee of the University of Turin and the Institutional Review Board were obtained.
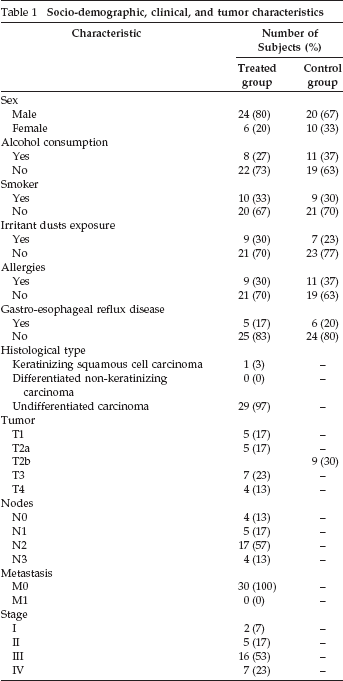
Mean age was 52.35 ∓ 11.89 years (range, 42–76 years) for the control group and 53.53 ∓ 10.96 years (range, 37–75 years) for the treated group. Socio-demographic and clinical characteristics, such as age and gender distribution tobacco, alcohol consumption, previous exposure to irritant substances, gastroesophageal reflux and allergies, and tumor related factors, such as histologic type, TNM classification and stage, are reported in Table 1. There were no clinical or demographic differences between control group and treatment group (p > 0.05).
Socio-demographic, clinical, and tumor characteristics
Chemo-radiotherapy schemes are reported in Table 2. Cisplatin-based concurrent chemotherapy (CT) was 30 mg/m2 administered weekly (one to three cycles) or 100 mg/m2 administered once every three weeks (five to eight cycles); neoadjuvant CT schemes included cisplatin/fluorouracil or taxanes/cisplatin/fluorouracil (one to three cycles); and adjuvant CT was based on one or two cycles of cisplatin and fluorouracil. Radiotherapy was performed using two-dimensional, conformal three-dimensional, or intensity-modulated techniques. Only two patients underwent selective or type III modified radical neck dissection for persistent nodal disease.
Chemo-radiotherapy schemes
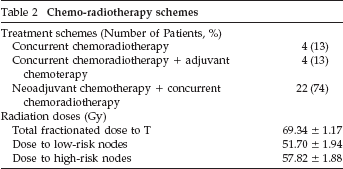
All patients were immobilized with a thermoplastic mask. Radiation techniques are described elsewhere.9,10
In two-dimensional radiotherapy (five patients) and conformal three-dimensional radiotherapy (five patients) groups, nasopharynx and metastatic lymph nodes were treated up to 70.2 Gy (1.8 Gy daily fractions, five fractions per week) with a six Megavolt linear accelerator (Elekta SL-75, Stockholm, Sweden). Uninvolved nodal levels I–IV and retropharyngeal nodes were treated bilaterally with 45–64.8 Gy using a shrinking lateral opposed field technique, with 50–54 Gy to lower part of the neck and supraclavicular fossae. High-energy electron boost (10–20 Gy) were used for posterior neck lymph nodes.
In the intensity modulated radiation therapy group (20 patients), a varied schedule was used. The most employed schedule provides the use of simultaneous integrated boost, with 70 Gy/35 fractions delivered to the nasopharynx and involved nodes, 63 Gy/35 fractions to high-risk negative lymph node echelons, and 54.25 Gy/35 fractions to node negative regions. Dose to the lower neck and supraclavicular fossae was 50 Gy in 25 fractions in the split-field technique. Intensity modulated radiation therapy plans were delivered with a six MV LINAC (Elekta Precise or Elekta Synergy, Stockholm, Sweden). Sparing of at least one parotid gland was attempted, especially the contralateral one with respect to tumor or metastatic lymph nodes.
All subjects underwent symptoms anamnestic evaluation (rhinorrea, nasal obstruction), endoscopic fiber optic nasal examination, skin-prick tests, and nasal scraping for cytological exam. Cytological samples were obtained by scraping with a Rhino-Pro Curette (ASI Arlington Scientific Inc., Springville, UT). Samples were collected from the medial portion of the inferior middle turbinate. After sampling, the material is laid on a microscope slide, fixed in 95° alcohol for four seconds, and stained by the May-Grünwald-Giemsa method. Observation is performed by a common optical microscope, provided it is able of a 1000X magnification, analyzing at least 50 microscopic fields. Nasal scraping and cytological analysis were performed by an otolaryngologist expert in these procedures and not knowing whether the subjects received radiotherapy or not. Skin-prick tests were performed to correctly evaluate nasal cytology. All cytological samples were collected in November, when the majority of pollens were absent. Specimen evaluation was performed using a checklist for cytological findings. 11
Statistical Package for Social Sciences, version 17.0, was employed for data analysis. A descriptive analysis of all data was performed, and they were reported as means or percentages and standard deviations. The Kolmogorov-Smirnov test demonstrated a non-Gaussian distribution of variables, so nonparametric tests were used. The χ 2 test was used to assess differences between groups in the mean of categorical variables. Odds ratios were reported. p < 0.05 was considered statistically significant.
Results
Median follow-up was 59 months (range, 21–124 months). Symptoms and endoscopic findings of healthy subjects and treated patients are reported in Table 3. A higher percentage of rhinorrhea, nasal obstruction, xerostomia, hyposmia, and hypogeusia at anamnestic evaluation and mucosal hyperemia and presence of nasopharyngeal secretions at fiber optic endoscopic examination was found in irradiated subjects (p < 0.05). No endoscopic signs of rhinosinusitis was observed in all patients. No specific treatments for nasal complaints were reported by the patients, with the exception of occasional nasal irrigation with saline isotonic solutions.
Symptoms and endoscopic findings
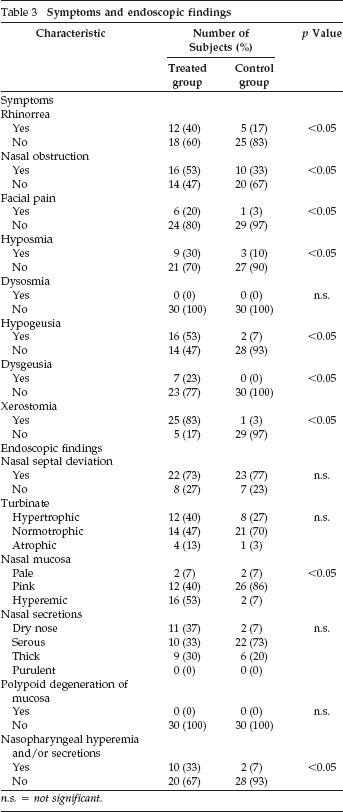
n.s. = not significant.
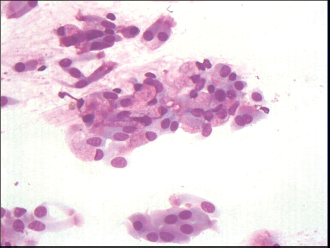
Cytological analysis demonstrated a neutrophilic inflammation in 13% of healthy subjects (control group) and in 40% of irradiated patients (odds ratio, 4.33); squamous cell metaplasia (presence of squamous cells) (Fig. 1) and mucous cell metaplasia (mucous cells more than 25% of epithelial cells) (Fig. 2) were found in 3% and 3% of control group and in 20% and 13% of treated patients, respectively (odds ratio for squamous and mucous cell metaplasia, 7.25 and 4.46, respectively). A statistically significant difference between healthy subjects and irradiated patients was observed (p < 0.05) (Table 4). Rare eosinophils were found in two healthy subjects and two irradiated patients; all these patients had an allergic perennial rhinitis. No mast cell and lymphocyte were found in both groups.

Nasal cytology (May-Grünwald-Giemsa staining, magnification: X400): squamous cell metaplasia and presence of bacteria in irradiated patients.
Nasal cytology (May-Grünwald-Giemsa staining, magnification: X400): mucous cell metaplasia in irradiated patients.
Nasal cytology findings

n.s. = not significant.
No cytological atypia (nuclear enlargement associated with increased nuclear-cytoplasmic ratio, hyperchromatism, chromatin clumping with moderately prominent nucleoli, irregular nuclear membranes and multinucleation, and variation in size and/or shape of the cells and nuclei) was seen. Concerning irradiated patients, the hyperchromatic supranuclear stria was absent in ciliated cells. 11
Analyzing nasal cytological changes of irradiated patients, no statistically significant correlation with symptoms, endoscopic findings (turbinate hypertrophy, mucosal hyperemia, nasopharyngeal secretions), patients' age, tobacco smoking, gastroesophageal reflux, and tumor stage was found (p > 0.05). Furthermore, no significant difference was found between different radiation techniques and radiation dose (p > 0.05).
Discussion
Radiation therapy for head and neck cancer is responsible for acute and long-term tissual changes. Acute alterations induced by radiotherapy characteristically are observed in several head and neck tissues: mucosa (erythema and ulceration), taste buds (decreased acuity), salivary glands (decrease in serous output), and skin (erythema and desquamation). All this tissue, however, underwent to late modifications: damage of the mucosa or skin may lead to ulceration, telangiectasia, and/or atrophy; loss of taste buds may result in transient or permanent hypogeusia; injury of the connective tissues may lead to fibrosis, trismus, edema, and soft tissue necrosis; and damage of the salivary glands may lead to xerostomia. 3
Concerning late toxicity, the classic concept that considers proliferation dynamics of the target organ to understand radiation effects has been integrated with recent investigations on molecular mechanisms. Thus, a combination of cell death, production of reactive oxygen species, alterations in gene expression, and expression of both proinflammatory and profibrotic cytokines are viewed as integral in pathogenesis of late effects.5,12–14
Acute mucositis is one of the most debilitating side effects of head and neck cancer therapy; experimental models suggests that mucosal alterations derived from an inflammatory cascade leading to cellular damage. However, Hamilton et al. found no typical microvascular inflammatory changes with video-imaging of sublingual microcirculation in radiation-induced mucositis. 15
A few studies investigated acute mucosal changes induced by radiation therapy, but no one evaluated late cytological alterations of nonmalignant mucosa in healthy patients. Lou et al., using ultrastructural studies, showed ciliary loss and disturbed mucociliary function at the infundibular epithelium at a median time of 5.9 years after radiotherapy (range, 0.8–23 years) in patients with rhinosinusitis 16 ;in contrast, we used a safe, not invasive method for evaluating mucosal changes in radiated patients with or without rhinosinusitis. Moreover, rhinosinusitis may represent a confounding factor for disturbed mucociliary function, and it should be taken into account.
Previous studies involving the middle ear mucosa reported that irradiation induces acute effects, including vacuolization of ciliated cells, appearance of compound cilia, expansion of intercellular spaces, hyperreactivity of secretion, and stromal edema.17–19 Delayed effects at 6–11 months after irradiation included reduction of cytoplasmic mass, variable degrees of ciliary loss, and widened intercellular spaces. 20
Mucosa is composed of rapidly renewing, proliferating cells, whereas soft tissues, particularly their vasculoconnective components, are more slowly renewing structures. Although actively cycling tissues tend to be more susceptible to radiation-induced mitotic deaths, both groups of tissues are relatively tolerant of irradiation. Clinically important late changes rarely occur until doses greater than 50.0 Gy (in conventional fractionation, 2 Gy per day, 10 Gy per week), and mucosal ulceration remains rare for doses less than 65.0 Gy. 3 Late effects of radiation on the mucous membranes of the upper aerodigestive tract are characterized by paleness and thinning of the epithelium, submucosal induration, and occasionally, chronic ulceration and necrosis with exposure of underlying bone and/or soft tissue. 3
Oral mucosal cell density and proliferation rate decrease during conventional radiotherapy of head and neck cancer. 4 However, mucosal tissue has been believed to be sufficiently rapidly dividing that the direct histopathological effects of irradiation are evident only during or shortly after irradiation. In our study, we demonstrated that this concept could not be considered true.
Nasal cytology is a safe, not invasive, low-cost method for evaluating mucosal changes. It is already a currently used tool for the diagnosis of allergic and nonallergic rhinitis and other pathological alterations of nasal mucosa. The nasal mucosa of healthy subjects is constituted by four cytotypes (ciliated, goblet, striated, and basal), which are arranged in a pseudostratified pattern on an underlying basement membrane, and does not show other cells except, rarely, neutrophils; therefore, the detection of a cell type different from these is a sign of possible pathology. 21
In our irradiated subjects, we investigated, particularly, the presence of inflammatory cells, squamous cell metaplasia, and/or prevalence of goblet cells. A high rate of neutrophilic infiltration (40%) was seen. Some of these cases were related to minimal persistent inflammation of allergic rhinitis or to nonallergic rhinitis. However, most of them may not be explained by causes other than radiation therapy. Only a few cases recognized the presence of bacteria as a cause of neutrophilic inflammation; nevertheless, this patients had not endoscopic findings of acute or chronic rhinosinusitis.
The presence of a minor component of squamous or mucous cell metaplasia could be considered normal in older subjects with previous exposure to irritants, but we showed a significant increase of these pathological conditions among irradiated patients compared with healthy ones; therefore, they were not only due to the aging process of nasal mucosa or previous exposure to irritant substances. Mucous cell metaplasia has important clinical consequences, in fact, the decrease of the ciliated component and the proportional increase of goblet cells elicits an abundant mucus production and its consequent endonasal stagnation.22,23 Furthermore, the decrease of ciliated cells can reduce the mucociliary clearance with the consequent presence of bacteria in nasal cavities, as reported in a few patients. Although rhinosinusitis is reported to be a common post-radiotherapy side effect in NPC patients, 24 no clinical and endoscopic findings of rhinosinusitis were found in our study.
We did not find any atypical cell in nasal mucosa of long-term survivor who underwent combined treatment for NPC; this issue is in contrast to the report of cytological atypia in oral mucosa during radiation therapy and/or chemotherapy. 8
In future, detailed knowledge of cytological changes in patients' nasal mucosa could represent a key prerequisite for the choice of effective interventions for late radiation-induced rhinitis, such as nasal irrigation, topical antibiotics, corticosteroids, and/or hyaluronic acid. 25 Further studies are necessary to investigate whether different treatments for nasal complaints in patients who underwent radiotherapy for head and neck cancer may be effective for different nasal cytological findings.