
Abstract
Background
Autoimmune thyroid diseases are the most common of all autoimmune diseases. In the literature, Hashimoto thyroiditis (HT) is considered to be a T-helper (Th) type 1 dominant condition, and Graves disease is considered a Th2-dominant condition.
Objective
The aim of this study was to highlight a new aspect of the relationships among Th cell subgroups by determining the incidence of autoimmune thyroid disease in patients with allergic rhinitis (AR).
Methods
Patients were diagnosed with AR based on their medical histories, physical examinations, and skin-prick test results in an outpatient clinic. The levels of free triiodothyronine, free thyroxine, thyroid-stimulating hormone, thyroid peroxidase antibodies, and thyroglobulin antibodies were measured in peripheral blood samples from all study subjects.
Results
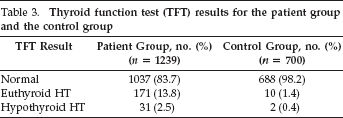
A total of 1239 patients with AR and 700 consecutive, age- and sex-matched healthy subjects were included in the study. Thyroid function tests showed that 1037 patients with AR (83.7%) had normal thyroid function, 171 (13.8%) had euthyroid HT, and 31 (2.5%) had hypothyroid HT. Among the control subjects, thyroid function test results showed that 688 subjects (98.2%) had normal thyroid function, 10 subjects (1.4%) had euthyroid HT, and 2 subjects(0.4%) had hypothyroid HT.
Conclusion
The incidence of HT in the general population is 1.5%; in contrast, it was observed in 16.3% of our patients with AR, which represented a much higher rate than that in the overall population. Graves disease was not detected in our study subjects. A high incidence of HT in patients with AR, in which Th2 responses are dominant, indicates that further studies of the relationships among atopy, autoimmune diseases, and Th cell subgroups are needed.
Allergic rhinitis (AR) is a global health problem that significantly affects quality of life. 1 AR is characterized by inflammation of the nasal mucosa that results from an immunoglobulin E mediated reaction. Cells, mediators, cytokines, neuropeptides, and a variety of adhesion molecules interact with each other and are involved in this inflammatory process. 2
CD4+ T-helper (Th) cells play an important role in the pathogenesis of allergic and autoimmune diseases. Th cells are traditionally classified as Th1, Th2, Th17, and regulatory T (Treg) cells and Th cells are further classified into subsets based on the different cytokines that they secrete. 3 Th2 cells play the most important role in AR. Although Th1 cells are dominant in healthy individuals, Th2 cells are dominant in the nasal mucosa and epithelia in patients with AR. 4 Treg cells regulate both Th1 and Th2 cell mediated inflammation. A lack of Treg cells increases the number of Th2 cells, thus increasing allergic inflammation. Treg cells limit allergic inflammation by synthesizing interleukin (IL) 10 and transforming growth factor β.5,6 Th17 cells respond to extracellular bacteria and fungi. Th17 cells are proinflammatory T cells, and they have been implicated in the cell-mediated cytotoxicity observed in some autoimmune diseases. 7
Other immunologic responses in both health and disease are under the control of similar cellular interactions. Immunologic disease results when these cellular interactions are not optimally regulated. The hypersensitivity disorder that results from an immunologic response to self-antigens is termed autoimmune disease. 8 The development of autoimmune disease depends on an imbalance among pathogenic factors generated by autoreactive T cells, B cells, macrophages, and natural killer cells, including mediators, cytokines, neuropeptides, and genetic factors, which together are the regulatory factors that normally control the immune response. 9 The balance among the responses mediated by Th1, Th2, Th17, and Treg cells is important in the development of autoimmune disease. In animal models of autoimmune diseases, Th1 cells cause tissue damage and disease progression, whereas Th2 cells suppress the autoimmune response. 10 Th17 cells may also play a role in various inflammatory diseases, although their contribution to human disease remains to be determined. Treg cells may be involved in regulating and attenuating the activity of the three Th subsets. 11
Autoimmune thyroid diseases (ATD) are the most common autoimmune disorders. They affect 1.5% of the U.S. population and disproportionately affect females. The pathogenesis is multifactorial and involves genetic and environmental factors. 12 There are primarily two autoimmune diseases that involve the thyroid gland: Graves disease (GD) and Hashimoto thyroiditis (HT). The dominant immunologic mechanisms in HT are T cell-mediated and cytokine-mediated cell damage, together with apoptotic cell death. 13 It has been shown that, although B lymphocytes and Th1, Th2, and Th17 cells are present in thyroid tissue in patients with HT, primarily Th1 cells are responsible for the development of the disease. In addition, the number of Treg cells in patients with HT are also decreased or insufficient. 14 In GD, the production of antibodies that stimulate thyroid-stimulating hormone (TSH) receptors also results in the stimulation of the activity and growth of thyroid follicular cells. The majority of intrathyroidal lymphocytes are T cells; however, B cells are also present. 15 Results of several studies have indicated that Th2 cell–mediated abnormal humoral immunity is important in GD, although which cell type is predominantly involved in the pathogenesis of GD remains controversial.16,17 In both HT and GD, individuals who are genetically predisposed show a complex relationship between humoral and cellular immune responses that are triggered by environmental agents. 18
In individuals with ATD, antibodies against three major thyroid antigens are found: thyroid peroxidase antibodies (anti-TPO Ab), thyroglobulin antibodies (anti-TG Ab), and thyrotropin receptor antibodies. Thyrotropin receptor antibody levels are found to be elevated predominantly in GD, whereas anti-TPO and anti-TG Ab levels are typically elevated in HT. 19 Very little is known about AR or the clinical course of autoimmune diseases and their effect on autoantibody production. 2 In light of this situation, this study aimed to provide a new perspective on the relationship between autoimmunity and allergy by assessing the prevalence of ATD in patients with AR.
Materials and Methods
This was a prospective study. The ethics board for clinical research of the Faculty of Medicine of Celal Bayar University, Turkey, approved this study on July 5, 2012 (Decision Reference 2012/159). Informed consent was obtained in writing from all the subjects. Patients who were included in the study had been diagnosed with AR and had been seen at the Adult Allergy Immunology Outpatient Center at Celal Bayar University for concerns of nasal drainage, nasal obstruction, and sneezing. Before participating in the study, patients’ medical histories were reviewed, and the patients were given a physical examination and a skin-prick test (SPT), as described below. The inclusion criteria for the study were that, it should be indicated in a SPT, the patients have a sensitivity to an allergen, and they did not have a history of receiving immunomodulator therapy, such as immunotherapy or corticosteroid therapy. AR symptom scores were recorded for all the patients during a symptomatic period of the disease. Incidents of sneezing, nasal obstruction, nasal itching, and watery nasal discharge were graded as 0, none; 1, mild; 2, moderate; or 3, severe, for a maximum of 12 points. Patients who did not have a positive SPT result, as defined below, who had received or were still receiving immunotherapy, or who did not have rhinitis-associated symptoms were excluded from the study. The free triiodothyronine (FT3), free thyroxine (FT4), TSH, anti-TPO Ab, and anti-TG Ab levels in peripheral blood were measured for all the participants by using a chemiluminescence method and FT3, FT4, TSH, anti-TPO, and anti-TG kits (Beckman Coulter DXI-800, Brea, CA). Some patients were reevaluated by using thyroid ultrasonography (Siemens Acuson Antares 2009, Siemens Acuson Antares, San Jose, CA) and scintigraphy as recommended by an endocrinologist (B Ozmen). The control group consisted of employees of the school of medicine or volunteers who were seen at the general internal medicine outpatient clinic and had no allergic symptoms or any known disease. Peripheral blood was also drawn from this control group, and FT3, FT4, TSH, anti-TPO Ab, and anti-TG Ab levels were measured for all the subjects in this group as well. The clinical findings and the laboratory and ultrasound results for both the patient group and the control group were evaluated by the same endocrinologist (B Ozmen). As a result of this evaluation, patients were diagnosed with HT and GD as appropriate. The endocrinologist (B Ozmen) and the radiologist (GO) were blinded to the study.
Spt
Allergic sensitization was demonstrated by using the SPT. SPTs were performed according to the European Academy of Allergy and Clinical Immunology guidelines 20 for the most common inhalant allergens in Turkey, including house-dust mites (Dermatophagoides pteronyssinus and Dermatophagoides farinae), fungi (Aspergillus fumigatus, Alternaria alternata, Cladosporium herbarum, Penicillium notatum), grasses (Lolium perenne, Festuca pratensis, Phleum pratense, Poa pratensis, Dactylis glomerata), weeds (Plantagolanceolata, Artemisia vulgaris, Rumex acetosa, Taraxacum vulgare, Parietaria officinalis), and trees (Sambucus nigra, Populus alba, Ulmus scabra, Salixcaprea, Fagus sylvatica, Carpinus betulus, Quercusrobur, Fraxinus excelsior, Olea europaea). Standardized histamine (1.7 mg/mL) and a standard negative prick solution (sodium chloride, 9 mg/mL; phenol, 4 mg/mL; and glycerol, 563 mg/mL) (Allergopharma Ltd, Reinbek, Germany) were used as positive and negative controls, respectively. Wheals that measured 3 mm or more in diameter in the areas in which histamine and allergen extracts were applied were accepted as a positive SPT result.
Statistical Analysis
The Statistical Package for Social Sciences Version 11.0 (SPSS Inc., Chicago, IL) was used for all statistical analyses. The independent samples t-test was used to compare the AR patient group and the control group. Values of p [lteq] 0.05 were considered statistically significant. The minimum number of study participants required for the study was calculated to be 1198 (the expected odds ratio 3.00, with a confidence interval of 95%) by using Epi Info 7.0 software (Centers for Disease Control and Prevention, Atlanta, GA) (for sample size and a power-unmatched case-control study). To achieve the required sample size, all patients who were seen at our clinic between July 5, 2010, and November 13, 2011, were included in the study, without using a sampling method.
Results
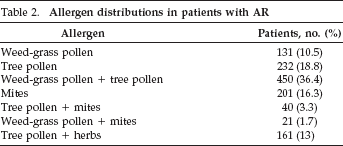
A total of 1239 patients with AR participated in the study. Of these, 631 were female (51%), and 607 were male (49%). The mean (standard deviation [SD]) age of the patients was 35.71 ± 11.14 years (range, 17-63 years), and the mean (SD) duration of disease was 7.32 ± 2.11 years (range, 2-22 years). The mean AR symptom score of the patients with AR was 11.37 ± 3.17 (range, 0-12). The demographic characteristics of the patient and control groups are shown in Table 1, and the distribution of reactions to allergens for each group are shown in Table 2.
Demographic characteristics of the patients with AR and the control group

Allergen distributions in patients with AR
When using thyroid function tests (TFT), 1037 normal thyroid (83.7%), 171 euthyroid HT (13.8%), and 31 hypothyroid HT (2.5%) cases were identified. GD was not detected. The 202 patients with HT were evaluated by using thyroid ultrasonography, and the results were consistent with thyroiditis. Scintigraphy was not considered to be necessary for any of the patients. In total, 202 patients with AR were diagnosed with HT: 149 females (74%) and 53 males (26%), with a mean (SD) age of 37.12 ± 11.3 years (range, 18-59 years). The mean (SD) duration of AR symptoms was 6.68 ± 2.13 years (range, 2-20 years).
There were 700 patients in the control group. A total of 350 control patients were female (50%), and 350 were male (50%). The mean (SD) age of the control group was 37.13 ± 13.28 years (range, 16-60 years). Based on the TFT results, 688 of these patients (98.2%) were found to have normal thyroid function, 10 patients (1.4%) were diagnosed with euthyroid HT, and 2 patients (0.4%) were diagnosed with hypothyroid HT. In total, eight female patients (67%) and four male patients (33%) had HT in the control group. GD was not detected in the control subjects. The TFT result summaries for the AR patient group and the control group are shown in Table 3, and the detailed TFT results and associated p values for both groups are shown in Table 4.
Thyroid function test (TFT) results for the patient group and the control group
Thyroid function test (TFT) results for the AR patient group and the control group
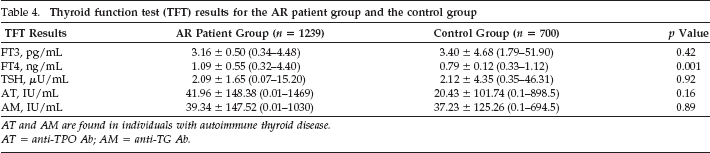
AT and AM are found in individuals with autoimmune thyroid disease.
AT = anti-TPO Ab; AM = anti-TG Ab.
A statistically significant difference was not found in the patients with AR with respect to allergen distribution, sex, age, age at disease onset, symptom scores, and ATDs. The FT4 value was found to be lower in the control group than in the AR patient group when using a t-test (p = 0.001). The prevalence of ATD was higher in the patients with AR compared with the control group (p = 0.0009). The prevalence of ATD was found to be 16.3% in the AR patient group and 1.8% in the control group.
Discussion
Published studies that examined the relationship between allergic and autoimmune diseases have been conducted in accordance with the hypothesis that the same excessive response that develops against exogenous antigens in patients with allergy could develop against endogenous antigens as well. Our aim was to provide a different clinical perspective on immune reactions associated with Th-cell subgroups by determining the prevalence of ATD in patients with AR. We found that the prevalence of HT was 16.3% in the AR patient group in our study and 1.8% in the control group. GD was not found in either group. In contrast with previous literature, HT, which is known to be Th1 mediated, was found to be more common in the patents with AR than in the control group. However, GD, which is Th2 mediated, was not detected in our patients with AR, although it is known that a Th2-mediated immune response is dominant in these patients.
Few previous studies have investigated the frequency of ATD in patients with AR. A study conducted by Reisacher 21 evaluated the prevalence of ATD in patients with AR and those without AR. Consistent with our results, the prevalence of ATD was found to be higher in the AR patient group than in the control group. In another study, Serafani et al. 22 showed that the prevalence of thyroid autoantibody positivity increased in patients with allergic asthma and/or AR; this result is compatible with our findings. In another study, Amino et al. 23 investigated the prevalence of AR in patients with GD and in those with HT. The prevalence of AR was 32.6% in the healthy control group, 42.9% in the patients with GD, and 21.6% in the patients with HT; it was also found that the prevalence of thyroid autoantibody positivity increased in patients with atopic eczema, and with allergic asthma and/or AR. 23
Numerous studies examined the prevalence of ATD in patients with atopic and autoimmune diseases. Readett 24 observed that the prevalence of thyroid disease was elevated in patients with atopic eczema. However, this relationship was not confirmed in studies conducted by Raffle and Hall. 25 In a study by Çakır et al., 26 the role of Th1-mediated immunity in allergic inflammation was investigated by examining the prevalence of atopic disease in type 1 patients with diabetes mellitus (DM) and in carriers of hepatitis B virus. It was found that the prevalence of allergic disease was elevated in carriers of hepatitis B virus, who typically lack Th1 immunity, and decreased in patients with type 1 DM, which is a Th1-mediated autoimmune disease. This previous study supports the Th1-Th2 model of allergic and autoimmune diseases. 26 Similarly, Meerwalt et al. 27 found a lower prevalence of atopic disease in children with type 1 DM disease compared with a control group. Sequeira et al. 28 found that the prevalence of drug allergies, insect allergies, and allergic asthma were elevated in patients with systemic lupus erythematosus, which is known to be a Th2-mediated non-organ-specific autoimmune disease.
Rheumatoid arthritis (RA) is a non–organ-specific autoimmune disease in which Th1- and Th17-mediated immune responses are known to be dominant. The results of studies that examined the prevalence of ATD in patients with RA have been mixed. Although previous studies showed that the prevalence of ATD was elevated in patients with RA, they also failed to show conclusively whether the prevalence of HT and GD, specifically, were elevated or re-duced.29,30
Hidaka et al. 31 showed that thyrotoxicosis was frequently aggravated after a Th2-mediated AR attack, which was accompanied by increases in serum immunoglobulin E and IL-13 levels in patients with concurrent GD and AR diagnoses. Similarly, the relapse rate was found to be higher in patients with concurrent GD and AR diagnoses compared with a control group. 32 Most previous studies showed that the prevalence of Th1-mediated diseases are reduced in patients with allergic diseases and that the prevalence of Th2-mediated diseases are elevated in patients with allergic diseases. Similarly, the prevalence of allergic disease is also elevated in patients with Th2-mediated diseases.33,34
Although organ-specific autoimmune diseases damage only the target organ, they also affect the entire immune system. For example, AR is characterized by inflammation around the nose and eyes, but it results in the activation of Th2-mediated immune responses that affect the entire immune system. It is also known that the Th1-mediated immune response is insufficient in these patients. 2 Dividing Th cells into two groups (Th1 and Th2) is a functional distinction that has improved our understanding of immunologic pathways as well as of disease itself. 35 However, with the discovery of Treg cells and Th17 cells, the focus of studies of immune response modulation has shifted toward these cell types. 36 The predominance of specific Th subsets varies across diseases, and such variation may promote different immunopathologic responses. However, this Th1-Th2 polarization is not apparent in some autoimmune diseases 37 ; moreover, the polarization of Th subsets is not absolute, and other subsets may also be present in a given disease.
In recent studies, Treg cells, which are thought to be involved in various autoimmune diseases, have been shown to play a significant role. Treg cell defects have been shown to reduce Th1 inhibition and to stimulate the production of Th1 cytokines in HT. 38 In a study in which thyroid infiltrates and peripheral blood lymphocytes were examined in patients with GD and in patients with HT, Marazuela et al. 39 found that Treg cell counts were higher in both peripheral blood and thyroid tissue from these patients. However, they also found that the suppressive functions of Treg cells were reduced in these patients; this caused their activity to be insufficient for the suppression of autoimmune responses. Gangi et al. 40 created an experimental animal model of HT and showed that the disease could be suppressed by treating animals by using granulocyte-macrophage colony-stimulating factor, which mediates IL-10 secretion from Treg cells.
Qin et al. 41 showed that IL-17A and interferon (IFN)-γ levels in peripheral blood lymphocytes and diseased thyroid tissue from patients with HT are higher than those in a control group. However, because they were unable to detect a statistically significant difference between the levels of IL-17A and IFN-γ in patients with HT, they suggested that Th1 and Th17 cells are jointly involved in the pathogenesis of HT. They also found no statistically significant difference in IL-17A and IFN-γ levels between patients with GD and individuals in the control group. These investigators thus suggested that Th1 and Th17 cells play a less significant role in GD pathogenesis than in HT pathogenesis. 41 These studies found increased differentiation of Th17 cells and enhanced synthesis of Th17 cytokines in ATD but mainly in HT. The discovery of Th17 cells and these recent findings have challenged the notion that HT is a solely Th1-mediated disease.
Thus, it has been suggested that the dominance of a specific Th subgroup within a given organ does not necessarily imply that the same Th subgroup is also dominant systemically. Our study showed that the prevalence of HT in patients with AR and with systemic Th2-cell dominance is higher than that in patients with organ-specific Th1 cell dominance. No study similar to ours, which investigated the prevalence of ATD within a large AR patient group, has previously been conducted. The effects of thyroid autoimmunity on the development of AR remain to be determined. In the present study, we found that the prevalence of HT, which is known to be Th1 mediated, was higher in the patients with AR, which is Th2 dominant, than in the controls, and we did not detect any Th2-mediated GD. This result indicates that further studies are needed to evaluate the relationships among atopic diseases, autoimmune diseases, and Th subgroups.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article