
Abstract
Objective
To determine if sex independently affects presentation and disease-specific survival (DSS) in patients with esthesioneuroblastoma (ENB).
Study Design
A case-control study from the Surveillance Epidemiology and End Results (SEER) data base.
Methods
The assessment identified 611 patients in the SEER data base who were diagnosed with ENB from 1988 to 2010. Data on race, ethnicity, age at diagnosis, sex, histologic grade, radiation treatment status, and surgical treatment status of patients with ENB from 1988 to 2010 were extracted. By using tumor extension data, the modified Kadish stage of each case was determined. The modified Kadish system was able to successfully classify 547 of 611 tumors from 1988 to 2010. Histologic grade, modified Kadish stage and DSS of male patients was compared with the DSS of female patients.
Results
Demographic data showed that male patients presented with a significantly higher grade (p < 0.05) and a trend toward a higher stage (p = 0.08). With unmatched data, male patients had significantly worse DSS than female patients (p < 0.05). After case-matching, the difference between the DSS for male versus female patients was no longer significant.
Conclusions
Male patients with ENB seemed to have significantly worse DSS at 10 years than female patients. This disparity seems to be due to higher grade and stage in male patients at presentation. After accounting for these two factors, the prognosis of male patients was not found to be significantly different from that of female patients.
Materials and Methods
A case-control study was undertaken that assessed the presentation and DSS of male versus female patients with ENB. Data were obtained from the Surveillance, Epidemiology, and End Results (SEER) program of the National Cancer Institute. SEER is a collection of population-based cancer registries across the United States that publishes cancer incidence and survival data that covers ∼28% of the population. 8 Data are subject to rigorous quality control studies and various assessments. This study was exempt from review by the institutional review board due to the de-identification of patient data.
Incidence
The SEER data base maintains standard population statistics from the 2000 and 2010 U.S. Census in the regions where cancer registry data are gathered. With the population data, we were able to obtain the relative incidence of ENB among different population groups in the United States. Rates were expressed per 100,000 persons, and the time period studied spanned from 2000 to 2010. The incidence of ENB was stratified by ethnicity, race, sex, and age.
Patient Selection
Patients with ENB were identified by the International Classification of Diseases for Oncology, Third Edition (ICD-O-3) histologic code 9522/3: olfactory neuroblastoma. The primary tumor location was determined by ICD-0–3 codes, with the vast majority originating within the nasal cavity or sinuses (IDC-O-3 codes 30.0, 31.0–31.3, 31.8–30.9). Any cases of ENB outside the head and neck region were excluded from analysis.
Demographics
Race, ethnicity, age at diagnosis, sex, histologic grade, radiation treatment status, and surgical treatment status were obtained from the SEER data base. ENB-specific staging information, e.g., Kadish stage, is currently not maintained by the SEER data base. However, related information, such as primary tumor location, extent of disease, and nodal status, has been coded from 1988 to 2010. During the time period studied, the SEER data base had two coding systems to describe tumor extension. From 1988 to 2003, the tumor extent of invasions is coded under Extent of Disease 10-extent, with codes for tumor localized to the site of origin, tumor involving adjacent connective tissue, tumor involving adjacent organs and/or structures, and further extension. In 2004, with the development of the American Joint Committee on Cancer staging systems, the tumor extension is now coded under Collaborative Staging extension, with the individual codes, depending on the structures involved. Due to this limitation in reporting stage, we used the modified Kadish staging as previously described. 4 Any tumors originating from the nasal cavity and with localized extension were considered Kadish stage A. Tumors originating from the nasal cavity with extension into the sinuses and tumors originating from the paranasal sinuses with localized extension were considered Kadish stage B. Tumors originating from both sites with orbital or intracranial extension were Kadish stage C, and tumors with distant or regional nodes were considered Kadish stage D. Tumors that were unable to be properly staged were excluded from survival analysis. All variables were treated as categorical inputs. Comparisons of demographic variables were performed with a Pearson's χ 2 test.
Survival Analysis and Matching
Survival time and DSS were obtained through the appropriate functions of the SEER data base. After matching for Hyams grade and Kadish stage, we obtained 210 matched male-female pairs. Kaplan-Meier survival models were created that evaluated male versus female survival for both the matched and unmatched patients. A 10-year survival curve and 2-, 5-, and 10-year survival intervals were generated by using SPSS 21.0 (SPSS, Inc., Chicago, IL). Comparison among survival curves was performed by a logarithmic pairwise χ 2 test. In addition, we created a univariate Cox proportional hazard regression model that evaluated the effects of sex on DSS. Our univariate model was compared with a multivariate Cox proportional hazard regression model that evaluated sex by using Hyams grade and Kadish stage included as confounding variables.
Results
The assessment identified 611 patients in the SEER data base who were diagnosed with ENB from 1988 to 2010. The modified Kadish system was able to successfully classify 547 of 611 tumors from 1988 to 2010.
Incidence
The overall incidence of ENB was 0.0477 cases per 100,000 from 2000 to 2010. Stratification of patients by age showed that ENB has a peak incidence of 0.1061 cases per 100,000 for patients ages 60–69 years old (Fig. 1). Male and non-Hispanic patients had a statically higher incidence of ENB (p < 0.05) (Table 1). There was no statistical difference in the incidence of ENB by race during the time period studied (Table 1).
ENB incidence in the United States, 2000–2010
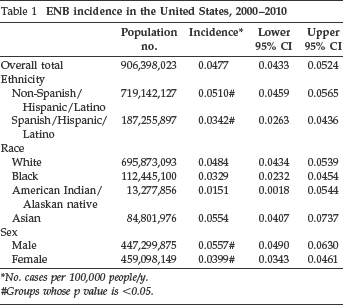
No. cases per 100,000 people/y.
Groups whose p value is <0.05.
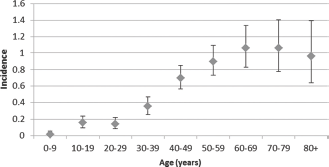
Incidence of ENB in the United States, 2000–2010, by age. The x-axis denotes the patient's age divided into 10-year groups, and the y-axis represents the number of cases of ENB per 100,000 people in 1 year.
Demographics
Male patients presented with a significantly higher Hyams grade (p = 0.037) and trended toward a higher Kadish stage (p = 0.081). Specifically, male patients had a larger proportion of grade IV and stage C tumors, and a lower percentage of grade I and Kadish Stage B tumors when compared with female patients (Table 2).
ENB presentation by sex, 1988–2010
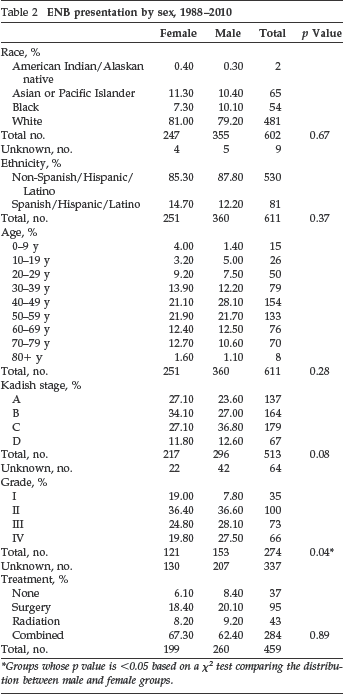
Groups whose p value is <0.05 based on a χ 2 test comparing the distribution between male and female groups.
Sex Survival Analysis
Before matching, we found that male patients had significantly worse DSS than female patients (p = 0.04), particularly at the 10-year mark (Table 3, Fig. 2). The male 10-year DSS was 60.00% (95% confidence interval, 52.75–67.25%) compared with the female 10-year DSS of 75.30% (95% confidence interval, 60.49–78.91%). However, after matching the cases by grade and stage, there was no significant difference in the DSS between the two groups (Table 3, Fig. 3). Male patients seem to have a worse prognosis than female patients, but this disparity in survival seems to be primarily driven by differences in Hyams grade and Kadish stage at presentation.
Unmatched and matched ENB DSS
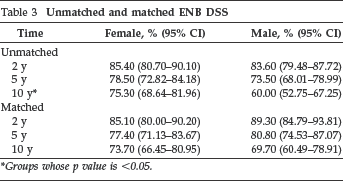
Groups whose p value is <0.05.
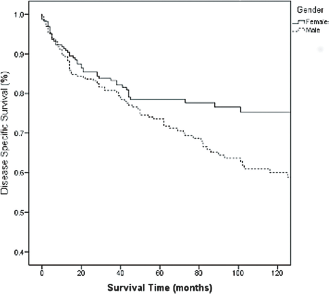
Kaplan-Meier 10-year unmatched ENB DSS curve. The x-axis represents the patient's survival time in months, and the y-axis represents the percentage of patients alive as calculated by disease-specific cause of death. Female (solid line) and male (dashed line) survival was compared by a logarithmic χ 2 test. (p = 0.04).
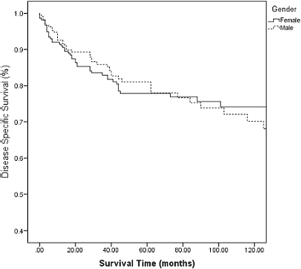
Kaplan-Meier 10-year matched ENB disease specific survival curve. The x-axis represents the patient's survival time in months, and the y-axis represents the percentage of patients alive as calculated by disease-specific cause of death. Patients were matched for Kadish stage and Hyams grade before analysis. Female (solid line) and male (dashed line) survival was compared by a logarithmic χ 2 test. (p = 0.78)
The Cox proportional hazard regression models support these findings. The univariate model showed a significantly higher hazard ratio for male patients (hazard ratio 1.420 [95% confidence interval, 1.0082.002]; p = 0.04). However, with the addition of Hyams grade and Kadish stage as confounding variables in the multivariate model, the male hazard ratio was reduced to 1.041 and was no longer significant (p = 0.88) (Table 4).
Cox proportion hazard regression models by sex
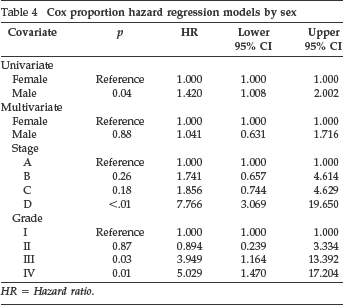
HR = Hazard ratio.
Discussion
The rarity of ENB makes the identification of patient risk and prognostic factors difficult, and typically limits studies to either systematic reviews or retrospective large multi-institutional data base studies. To date, the primary prognostic factors that have been identified for ENB are Hyams grade, Kadish stage, lymph node status, and age at diagnosis older than 65 years.1,4,5,7,9 Other demographic factors, such as race, ethnicity, and sex, are often included in the final regression models4,5,10 but have not been individually addressed as primary risk factors. The results presented demonstrate a higher incidence of ENB among male patients. In addition, male patients with ENB presented with a significantly higher Hyams grade and a trend toward more advanced Kadish stage. These two factors seem to directly affect male survival, as demonstrated by the pre- and post-matched Kaplan-Meier survival curves and univariate versus multi-variate Cox regression analysis models. Therefore, it seems that male patients with ENB carry a significantly lower 10-year survival than their female counterparts due to their presentation with higher grade and more advanced stage tumors.
The rarity of ENB makes it difficult to ascertain why male patients may present with higher-grade tumors. Hyams grade was first documented by Dulguerov et al. 2 as the most significant prognostic factor in ENB survival. This observation has since been confirmed by several follow-up studies that evaluated Hyams grade independently of Kadish stage.7,11,12 Given these findings, many researchers have alluded to low and high grade as separate entities with a significantly different prognosis for survival.11,12 In a review of the ENB literature, we were unable to identify any studies that directly compared male versus female tumor presentation.
There has been a great deal of evidence that showed sex-specific discrepancy in numerous cancers. A review of an international data base (Cancer Incidence in Five Continents) has shown that male patients have a significant increased incidence of 32 different cancers than female patients. 13 The most common cancers with male predominance were laryngeal, hypopharyngeal, lip, and urinary bladder cancer, and Kaposi sarcoma.13,14 In addition, male patients tend to present with more advanced stage lung cancer and melanoma.15,16 The sex difference in presentation of some cancers can be partially explained by an increased incidence of smoking or certain occupational exposure among the male population. 15 However, in many instances, although controlling for environmental and genetic factors, there is still no clear explanation for the sex discrepancy in presentations that are found in many cancers.13,17 Furthermore, a systematic review showed that female patients also tend to have survival advantage over male counterparts in six cancers: melanoma, lung, colorectal, gastric, esophageal, and soft tissue sarcoma. 18 Some of this survival advantage is likely due to early stage disease presentation in female patients, but, again, this alone has been insufficient to account for the differences in survival. 18
The primary limitation of our study was the reliance on the SEER data base coding system for sinonasal tumor characteristics. An accurate Hyams grade could only be obtained on roughly 45% of our patient population, and a modified Kadish stage had to be inferred based on historic SEER coding principles. The reliance on historic data increased the probability of coding errors in the data base. Furthermore, the SEER data does not account for changes in radiologic and surgical treatment strategies over time. Despite these limitations, over the past 20 years, there have been no documented changes in ENB treatment based solely on sex, and, given the quality control measures used by the National Cancer Institute, it is unlikely that there are enough documentation errors in the data to significantly affect the prognostic trends of these 611 patients.
Conclusion
Male patients carry a significantly worse ENB prognosis after 10 years compared with female patients; however, this disparity in survival seems to be driven by a higher Hyams grade and Kadish stage at presentation among male patients. After accounting for these two factors, male survival was not found to be significantly different from female survival for ENB. Therefore, even though males carry a significantly worse prognosis for ENB, treatment and outcomes should be based primarily on tumor grade and stage because sex itself does not seem to have an independent effect on ENB prognosis.
Footnotes
ACKNOWLEDGMENTS
We thank Jacqueline Ho for assistance provided in preparation of the ENB incidence figure.