
Abstract
Background
Chronic rhinosinusitis (CRS) is recognized as a common disease that imposes a big burden on the health system worldwide. There is ongoing evidence of the anti-inflammatory effect of long-term macrolide in the management of patients with CRS.
Objective
The aim of this randomized clinical trial was to evaluate the efficacy of long-term consumption of low-dose azithromycin after functional endoscopic sinus surgery.
Methods
Sixty-six patients who fulfilled the inclusion criteria were randomly divided into intervention and control groups. The subjects received the standard conventional treatment (fluticasone nasal spray plus normal saline solution irrigation) or the conventional treatment plus 250 mg of azithromycin on a daily basis for 3 months. Evaluation was made based on the 22-item Sino-Nasal Outcome Test (SNOT-22) immediately before surgery and 3 months after surgery.
Results
The intervention group showed a statistically significant improvement in SNOT-22 scores after the treatment and a higher percentage change after 3 months of therapy compared with the control group. A significant correlation was found between the percentage change of SNOT-22 scores and smoking in the placebo group. Lund-Mackay scores, patient age, and the duration of symptoms had no significant correlation with the percentage change.
Conclusion
Treatment with long-term low-dose azithromycin in combination with the conventional therapy could statistically reduce the recurrence rate of CRS symptoms after functional endoscopic sinus surgery, but there was not sufficient evidence to support clinical significance of azithromycin at the investigated dose. Further larger scale trials, along with a longer follow-up period, is needed to evaluate the effectiveness of the therapy.
The initial treatment for CRS is salt water irrigation and nasal corticosteroids. More severe cases are treated with oral corticosteroid and antibiotics. In patients in whom initial medical treatment failed and who have persist or worsening symptoms, surgery is indicated. Although endoscopic sinus surgery (ESS) has a success rate that ranges from 75 to 98%,4–6 mucosal inflammation necessitates continuous long-term medical treatment after surgery. In addition to their antimicrobial effect, macrolides are considered to have anti-inflammatory capacities through their immunomodulatory effect, which is achieved via hindering the proinflammatory cytokines production, which affects neutrophil migration and adhesion, and modulates the synthesis and secretion of mucus.7,8
The results of some recent studies indicate that, in addition to the probable effect of long-term macrolide therapy on CRS, postoperative long-term macrolide therapy with erythromycin or clarithromycin is effective in decreasing the number of clinical symptoms and improving the quality of life.9,10 Few randomized trials have been reported in which the efficacy of long-term, low-dose macrolides in CRS was examined. To further evaluate the use of azithromycin in the treatment of CRS, a double-blind, randomized, placebo-controlled trial was designed to examine the efficacy of postoperative long-term azithromycin in patients with CRS.
Materials and Methods
Study Population
This study was designed as a double-blind, randomized, placebo-controlled unicenter trial to investigate the efficacy of postoperative long-term azithromycin in patients with CRS. It has been registered by the Iranian Registry of Clinical Trials (201105146468N1). Full ethical approval was granted by the research ethics committee of Tehran University of Medical Sciences. Sixty-six patients, who ranged in age from 15 to 62 years old (mean, 37.7 years), with chronic sinusitis and who had attended the Otorhinolaryngology Department, Vali-Asr Hospital, between March 2009 and April 2012 were enrolled in the study. A thorough explanation of the objectives and the methods of the study with its expected effects and potential risks was provided for each patient, and voluntary written informed consents were obtained. Patient specifications, including telephone and identification card numbers, were collected.
Patients with >3 months of CRS symptoms and endoscopic signs and/or changes on computed tomography (CT) and who did not respond to the standard treatment regimes, including nasal saline solution irrigation combined with intranasal corticosteroids and antibiotics, and were candidates for ESS, were recruited. The exclusion criteria included previous sinus surgery, hypersensitivity to macrolides, use of drugs suspected of having interactions with macrolides, cystic fibrosis, congenital mucociliary problems, immune deficiency, systemic vasculitis, severe septal deviation, and craniofacial malformation. Patients who had used systemic antibiotics and/or systemic corticosteroids within 4 weeks of the study or throughout the study were excluded.
Randomization
The study medications were randomized through block randomization with 2:1 randomization design (block size of 6). According to the randomization schedule, the pharmacist produced numbered bottles, each labeled with a patient's study number, which contained either azithromycin or placebo. The patients were given study medication with consecutive numbering and a 3-month supply of medication. The patients, investigators, and individuals who analyzed the outcomes were unaware of the randomization schedule.
Intervention
The subjects were randomized to receive 250 mg of oral azithromycin for 12 weeks on a daily basis or placebo after the surgery. All the patients received a 12-week course of nasal saline solution irrigation, three times a day, and intranasal corticosteroid preparation (fluticasone, 2 puffs twice a day).
Outcomes
The nasal cavity was examined with a rigid nasal endoscope. All evaluations were carried out by the first author (A.A.). A CT of the paranasal sinuses was conducted before ESS and was scored by using the Lund-Mackay scoring system. 11
The patients’ main concerns, including postnasal discharge, nasal congestion, facial fullness, and facial pain or headache as well as the duration of the symptoms were assessed. Moreover, the 22-item Sino-Nasal Outcome Test (SNOT-22) questionnaire was completed by all the subjects. 12 After the 12-week course of treatment, the SNOT-22 questionnaire was completed by the patients once again. The primary outcome measure considered in this study was the percentage change of SNOT-22 scores, which was calculated as follows: ([before treatment SNOT-22 score — after treatment score]/before treatment score) X 100. The Morisky Medication Adherence Scale 4 was used to subjectively measure medication-taking behavior. The patients were questioned about their forgetfulness or carelessness with taking their medication and whether they had stopped taking the medicine when they had been feeling better or worse.
Analysis
With N = 22 per group, the current trial would have an 80% chance of detecting 20% difference in the groups’ means in the outcome measure. This calculation was based on a two-sample t-test with a two-sided alternative hypothesis that assumed equal group variances and a type 1 error level of 5%. All statistical analyses were performed with the use of computer software (SPSS, version 15; IBM Corp, Armonk, NY). The distribution of continuous variables was analyzed by using the Kolmogorov-Smirnov test for normality. Baseline variables were compared between the two groups by using the independent Student's t-test and x 2 test. Correlations were analyzed by using the Pearson correlation coefficient. A p value of <0.05 was considered statistically significant.
Results
Sixty-six patients with CRS were enrolled in the study. All the patients were unresponsive to the conventional medical treatment and were candidates for ESS. The patients who were randomized to receive azithromycin (n = 22) or placebo (n = 44) were later followed up for 12 weeks. During the monthly follow-up visits, the patients were encouraged in adherence to their medication. Four patients in the placebo group and two patients in the azithromycin group were lost to follow-up (Fig. 1). Both the azithromycin group and the placebo group had a high adherence to medication; the mean score of the Morisky Medication Adherence Scale 4 in the azithromycin group and in the placebo group was 0.95 and 0.91, respectively. No significant difference was identified between the placebo and azithromycin groups in terms of age, sex, smoking, history of allergy, asthma, nasal polyposis, CT score, or baseline values of the SNOT-22 score. Smoking was reported over the whole group, including smokers and nonsmokers in terms of pack-year. The patients’ main concerns, including postnasal discharge, nasal congestion, facial fullness, and headache, showed no significant difference between the two groups. There was also no significant difference between the two groups in the duration of any of the above-mentioned symptoms before the surgery. No one had aspirin triad. The patients’ characteristics at the time of enrollment are summarized in Table 1.
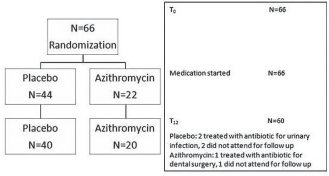
Chart of patients.
Patient characteristics at enrollment
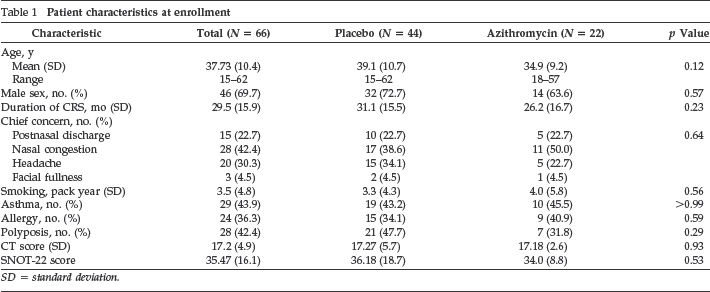
SD = standard deviation.
Although the duration of symptoms was longer in men compared with women (33 versus 21 months; p = 0.01), no difference was observed in SNOT-22 and Lund-Mackay scores. No significant correlation was observed between pretreatment SNOT-22 scores and patients age or duration of symptoms. The SNOT-22 questionnaire was completed by the patients after the treatment. The azithromycin group showed a mean score of 5.85 after the treatment and an 80% change, whereas the placebo group showed a mean score of 10.07 after treatment and a 68% change. The improvement in SNOT-22 scores after treatment and the percentage change were statistically significant in the intervention group compared with the control group after 3 months of therapy (p < 0.05), but the improvement in outcomes was <8.9, which was reported as the minimal clinically important difference (MCID) score of SNOT-22 (Table 2). SNOT-22 scores before and after the treatment are shown in Fig. 2.
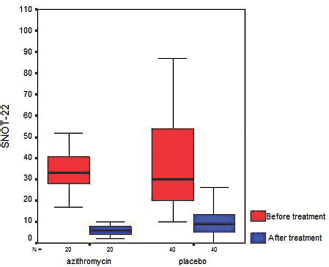
SNOT-22 scores before and after the treatment.
SNOT-22 scores and the percentage change

Percentage change = ([before treatment score — after treatment score]/before treatment score) X 100. SD = standard deviation.
The whole SNOT-22 scores at baseline and after treatment in placebo and azithromycin groups are summarized in Table 3. Within-group analysis showed that improvements in symptom scores, 3 months after the therapy were significant across all items of SNOT-22 in each group of patients. Between-group analysis showed that posttreatment scores for nasal obstruction and postnasal discharge were significantly lower in the azithromycin group. The scores for nasal obstruction in the azithromycin and placebo groups were 0.85 and 1.45, respectively (p = 0.007). The score for postnasal discharge was 0.35 in the azithromycin group and 0.7 in the placebo group (p = 0.019).
SNOT-22 symptoms before and after treatment
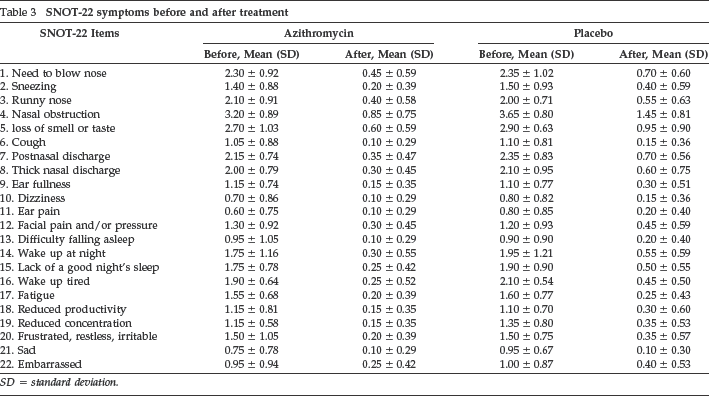
SD = standard deviation.
A significant correlation was found between the percentage change of SNOT-22 scores and smoking in the placebo group (correlation coefficient = 0.31; p = 0.05). No significant correlation was found between the percentage change and smoking in the azithromycin group (p = 0.45). Similarly, Lund-Mackay scores, patient age, and duration of symptoms had no significant correlation with the percentage change.
Adverse Events
The subjects in the placebo and azithromycin groups underwent follow-up visits for 3 months after surgery. Headache, trouble sleeping, nasal congestion, fatigue, postnasal discharge, cough, and nasal inflammation are CRS symptoms, and were not judged as adverse events. No serious adverse event, including angioedema, anaphylaxis, and cholestatic jaundice, was reported.
Discussion
CRS can be a debilitating condition and has a great impact on health-related quality of life. Despite myriad advances in the management of CRS during the past decade, a proportion of patients still do not respond to the conventional treatment. Recently, the anti-inflammatory efffect of macrolides, besides its bacteriostatic and bactericidal effect, have been observed. This effect results in the usage of this group of antibiotics for chronic inflammatory diseases, such as atopic dermatitis, nonspecific inflammatory bowel disease, psoriasis, and arthritis. 13 It is also shown that macrolide (azithromycin) is effective in the prevention of bronchiectasia exacerbations in patients without cystic fibrosis. 14
The anti-inflammatory properties of macrolides by downregulation of proinflammatory cytokines may result in the inhibition ofinflammatory pathways that contribute to CRS. Studies proved the benefits of macrolide therapy in the treatment of nasal manifestations of “sinobronchial syndrome.”15,16 The efficacy of macrolides has been proposed to be improved by long-term use. 17 In several studies, macrolide therapy for patients with CRS was evaluated, among which a recent review of three prospective clinical studies found limited scientific evidence that supports long-term use of macrolide therapy for CRS.18–20 The former prospective clinical studies that evaluated the effect of long-term macrolide therapy during the postoperative period are so scarce that the results are negligible and inconclusive.
Wallwork et al. 21 compared roxithromycin with placebo daily for 12 weeks. They found significant improvements in SNOT-20 scores, nasal endoscopy, saccharine transit time, and interleukin 8 levels in lavage fluid in the macrolide group. Moreover, a correlation was found between improved outcome measures and low immunoglobulin E levels. 21 Amini et al. 22 treated the patients with clarithromycin for 3 weeks on a daily basis and the comparative group with amoxicillin-clavulanic acid 625 mg three times a day for 3 weeks. No difference was witnessed between the groups. 22 Videler et al. 23 treated patients with azithromycin 500 mg daily for 3 days and then 500 mg weekly for 11 weeks; similarly, no significant difference between the azithromycin and the placebo groups was found in terms of the SNOT-22, Patient Response Rating Scale, Visual Analog Scale scores, Short-Form 36, nasal endoscopic findings, peak nasal inspiratory flow results, smell tests, and microbiology. 23
According to our review of the literature, this study was the first double-blind, randomized, placebo-controlled trial of long-term, low-dose azithromycin therapy in the postoperative management of CRS. This study showed that azithromycin may have the potential for resulting in an improvement in the patients’ quality of life compared with the control group, although, this improvement was clinically insignificant according to the previously reported MCID score of SNOT-22. The SNOT-22 baseline scores were relatively low in both groups; this could be explained by other factors, such as psychological status and the individual's interpretation of circumstances. As Browne et al. 24 reported in their study, the SNOT-22 does not only evaluate rhinologic symptoms but also the psychological status, as another important factor.
The limitation of this study that is worth mentioning is the number of patients in placebo group was twice as large as the azithromycin group. In addition, the emergence of resistant organism due to the long-term administration of antibiotics could possibly occur and, consequently, considering the nasopharyngeal swab to monitor the bacterial resistance could be helpful in further studies. To assess the long-term benefits, patients should be followed up after the cessation of the study medication, and applying objective outcomes, for example, the endoscopic score, helped us achieve a more comprehensive scope of treatment. When considering the fact that the MCID is not a universal fixed attribute and depends on patients’ baseline status, we believe that the MCID should be applied cautiously. Therefore, further studies are required to evaluate the consistency of our obtained result and to assess the long-term beneficial effect of azithromycin.
Footnotes
Acknowledgments
We thank the research committee of Tehran University of Medical Sciences and the personnel of Vali-Asr Hospital for their contribution in this study.