
Abstract
Background
Serum squamous cell carcinoma antigen (SCCA) levels are elevated in sinonasal inverted papilloma (IP). However, the relationship between tumor volume and SCCA level, and the influence of skin or pulmonary diseases in which the SCCA level is high, have not been established.
Objective
To clarify whether the level of serum SCCA can be used as a diagnostic marker of IP.
Methods
Serum SCCA level was measured in 30 patients with IP (IP group) and 57 with inflammatory disease (inflammatory group).
Results
Overall, 83.3% in the IP group showed elevated serum SCCA levels regardless of whether they were new patients or patients with recurrent IP, and SCCA levels rapidly decreased after surgery. Only 5.3% had elevated SCCA levels in the inflammatory group. Before surgery, the IP group had a median preoperative SCCA level of 2.4 ng/mL, whereas the median preoperative SCCA level was 0.9 ng/mL in the inflammatory group. Pre- and postoperative SCCA levels were significantly different in the IP group. With regard to the IP diagnosis in the IP and inflammatory groups based on the SCCA level (ng/mL), sensitivity and specificity were 83.3% and 94.7%, respectively. There was no significant correlation between SCCA elevation and respiratory function, and skin disease in the two groups, except for smoking in the IP group. Preoperative SCCA levels were significantly higher in smokers than in never-smokers in the IP group. Tumor volume was significantly correlated with SCCA level in IP. Multivariable logistic analysis showed that tumor volume was a predictor of preoperative SCCA elevation (p = 0.036; 95% confidence interval, 1.027–2.176).
Conclusion
Serum SCCA level is a reliable diagnostic marker to distinguish new and recurrent IP from inflammatory disease. Because smokers tended to have higher SCCA levels in IP, a different cutoff level might be needed. Although respiratory dysfunction and skin disease were not related to SCCA level, they should be taken into consideration when evaluating SCCA level.
Inverted papilloma (IP) in the paranasal sinus is a benign neoplasm with unique clinical characteristics; in particular, it has a high recurrence rate, and a malignant lesion might develop. Recently, Wnt signaling proteins, including β-catenin, cyclin D1, and Dvl-1, may play crucial roles in the malignant transformation of IP. 5 Based on several meta-analyses of IP treatment, local recurrence after endoscopic resection and the incidence of malignancy in IP are estimated to be ∼12% and 10%, respectively.6,7 Because the recommended treatment for IP is complete surgical excision, the preoperative diagnosis of IP and the evaluation of IP extension are important for adequate resection of IP. However, in recurrent cases, it is sometimes difficult to diagnose and resect IP due to anatomic alterations from previous operations, e.g., as a result of bony hypertrophy and substantial scarring. In addition, because IP sometimes blocks the sinus ostium, the clinical features of IP resemble unilateral paranasal sinusitis with polyps. 8 The surgical technique for IP is totally different from that for chronic sinusitis, which preserves most of the sinus mucosa intact. Therefore, the preoperative diagnosis of IP and evaluation of IP extension are important for adequate resection of IP.
Yasumatsu et al. 9 first reported that the serum SCCA level is elevated in patients with IP of the sinonasal tract. In our previous study, we demonstrated that 81.8% of patients with IP and 90.3% with recurrent IP have significantly elevated SCCA levels compared with patients with inflammatory disease (the inflammatory group). 10 The quantitative values of both SCCA1 and SCCA2 messenger RNA expression in patients with IP were significantly higher (i.e., SCCA1, 22.6-fold higher; SCCA2, 23.0-fold higher) than those in the inflammatory group. 10 However, the SCCA level in the previous study was not significantly correlated with clinical characteristics, including the Krouse stage. The aim of the present study was to determine whether the serum SCCA level could be used as a diagnostic marker at the initial evaluation and in the postoperative follow-up of patients with IP.
Methods
A total of 30 patients with IP in the paranasal sinus surgically treated from January 2006 to January 2015, took part in the present study (IP group). To investigate the significance of SCCA in the IP group, 57 patients with nasal and paranasal inflammatory diseases, such as chronic sinusitis, eosinophilic sinusitis, and postoperative maxillary cyst (inflammatory group), also participated in the present study. Surgical specimens from all the patients with IP and those with inflammatory disease were examined to confirm the pathology. Patients with pulmonary and skin diseases showed elevated serum SCCA levels; therefore, these diseases as well as smoking habit were recorded. 4 The study protocol was approved by the institutional review board of the University of the Ryukyus. This study was conducted in accordance with the principles of the Declaration of Helsinki. Y. Yamashita and T. Uehara contributed equally to this study.
SCCA Measurement
Serum SCCA levels in the IP group were measured before and after surgery, and during the follow-up period. Patients in the inflammatory group were examined only before surgery. Because the elevated serum SCCA level in patients with oral cancer returned to normal within 4 days, 11 the postoperative SCCA level was measured within 1 week after surgery. The SCCA level was measured by using the IMx SCCA microparticle enzyme immuno-assay (Abbott Laboratories, Tokyo, Japan) until December 2008, 12 and Architect, an automatic chemiluminescence immunoassay (Abbott Laboratories), from January 2009. 13 Because the correlation coefficient of the SCCA level measured by the two different methods is 0.977, 14 data obtained by using these two methods were considered identical. A level of ≤1.5 ng/mL was considered normal according to the manufacturers’ instructions.
Relationship between Clinical Characteristics and SCCA
The Krouse classification, 1 history of previous surgery, recurrence after surgery, skin diseases, pulmonary function, smoking habit, and tumor volume were recorded retrospectively according to patients’ clinical records. Tumor volumes were measured by magnetic resonance imaging (MRI) by using the OsiriX Dicom Viewer 6.02 (Pixmeo, Geneva, Switzerland) software in the patients with IP.
SCCA Level Alteration in Recurrent Cases
The relationship between tumor volume and SCCA level alteration was determined in patients with recurrence after surgery.
SCCA Fluctuation in Patients without IP Recurrence during the Follow-up Period
To evaluate physiologic fluctuation of the SCCA level in patients without IP recurrence, the SCCA level was repeatedly examined during the follow-up period for 26 of 28 patients.
Statistical Analysis
Differences between patients with normal SCCA levels and patients with elevated SCCA levels were determined in the IP group by using the two-tailed Pearson χ 2 test or Fisher's exact test. Serum SCCA levels in the IP and inflammatory groups were statistically evaluated by the Mann-Whitney U test. The sensitivity, specificity, positive predictive value, negative predictive value, and predictive accuracy of the outlier serum SCCA levels (≤1.5 ng/mL) were measured. The Wilcoxon signed rank test was used to determine differences between pre- and postoperative SCCA levels in the IP group. Statistical analysis of the correlation between the preoperative SCCA level and the tumor volume in the IP group was performed by using the Spearman rank correlation coefficient. Multivariable logistic regression models were prepared to estimate the SCCA elevation associated with potential predictors, including clinical variables, such as smoking habit and tumor volume, and were used to calculate odds ratios and 95% confidence intervals after controlling simultaneously for other potential predictors. All analyses were performed by using the SPSS statistical package (SPSS for Windows, version 19.0; SPSS Inc., Chicago, IL). Statistical significance was established at the p < 0.05 level.
Results
Clinical Characteristics and Serum SCCA Level
The clinical characteristics of the patients with IP are shown in Table 1. The IP group consisted of 18 male and 12 female participants (age range, 10–77 years; median, 58.5 years), including 22 with new IP and 8 with recurrent IP who underwent previous surgery at another hospital. The mean and median observation periods after surgery were 36.6 months and 30.5 months, respectively.
Clinical characteristics of the inverted papilloma group
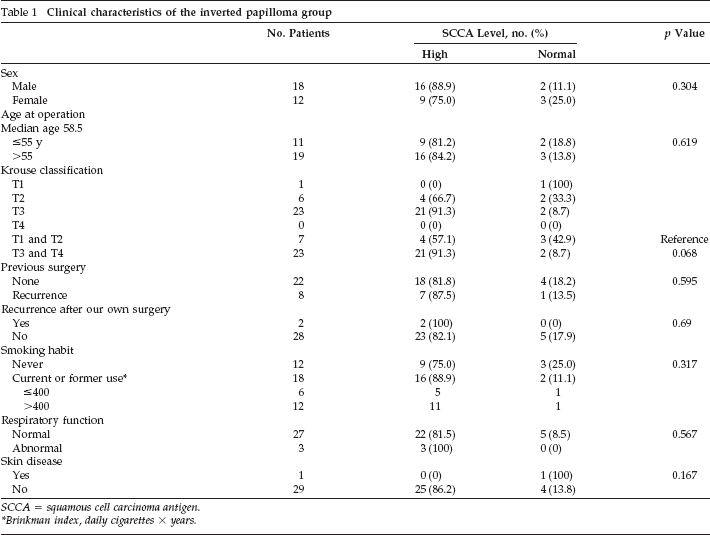
SCCA = squamous cell carcinoma antigen.
Brinkman index, daily cigarettes X years.
Of 30 IP cases, 25 patients (83.3%) showed elevated serum SCCA levels, and 7 of 8 patients (87.5%) with recurrence also had elevated SCCA levels. There were no significant correlations between SCCA elevation and any of the observed clinical characteristics listed in Table 1 (sex, age, Krouse classification, previous surgery, recurrent case, respiratory function, and skin disease). Although the proportion of smokers in the high SCCA group was similar to the normal SCCA group, preoperative median SCCA values in smokers and never-smokers were 4.2 ng/mL (interquartile range, 1.9–8.4 ng/mL) and 2.0 ng/mL (interquartile range, 1.6–2.4 ng/mL), respectively. There was a significant difference in preoperative SCCA values between smokers and never-smokers (p < 0.021, Mann-Whitney U test).
The inflammatory group consisted of 33 male and 24 female participants (age range, 10–78 years; median, 52.1 years), as shown in Table 2. There were only three patients (5.3%) with a high SCCA level in the inflammatory group. Of the three patients with an elevated SCCA level, two with a smoking history had mild pulmonary dysfunction and the one never-smoker had severe polyposis due to allergic fungal sinusitis. Among these three cases, two patients had normal SCCA levels after surgery. There was no significant correlation between SCCA elevation and clinical characteristics, including smoking status, in the inflammatory group (Table 2). Although the rate of never-smokers was smaller in the inflammatory group than in the IP group, the difference did not reach the level of significance.
Clinical characteristics of the inflammatory group
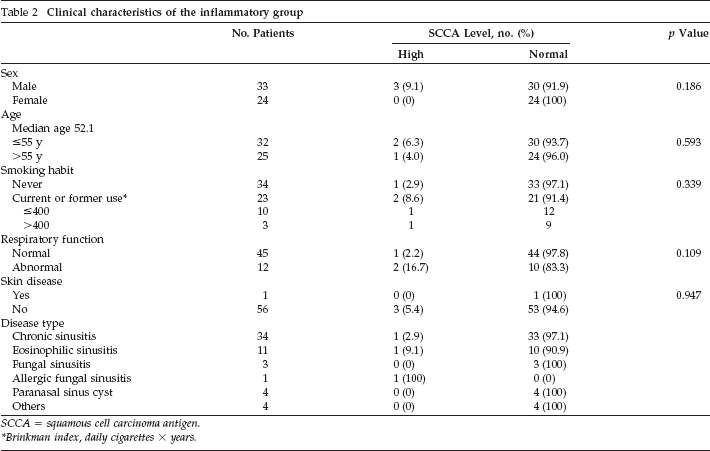
SCCA = squamous cell carcinoma antigen.
Brinkman index, daily cigarettes × years.
The receiver operating characteristic curve analysis for SCCA level yielded an area under the curve of 0.889 (Fig. 1). Regarding the IP diagnosis in the IP and inflammatory groups based on the SCCA level (≤1.5 ng/mL), sensitivity, specificity, positive predictive value, negative predictive value, and predictive accuracy were 83.3, 94.7, 89.3, 91.5, and 90.8%, respectively.
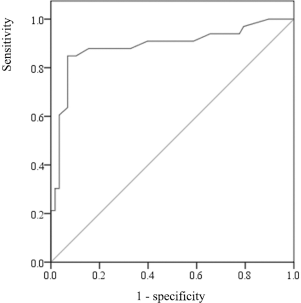
Receiver operating characteristic (ROC) curve analysis for squamous cell carcinoma antigen (SCCA) in the inverted papilloma (IP) and inflammatory groups. ROC curve analysis yielded an area under the curve of 0.889 (95% confidence interval, 0.807–0.970).
Pre- and Postoperative SCCA Levels in the IP Group
The median preoperative serum SCCA level was 2.4 ng/mL (interquartile range, 1.7–5.2 ng/mL) in the IP group and 0.9 ng/mL (interquartile range, 0.6–1.3 ng/mL) in the inflammatory group. There was a significant difference in the preoperative SCCA concentration between the IP and inflammatory groups (p < 0.001) (Fig. 2). The median postoperative serum SCCA level in the IP group was 1.0 ng/mL (interquartile range, 0.8–1.4 ng/mL). In three patients, the SCCA level was >1.5 ng/mL within 1 week after surgery. There was a significant difference in SCCA levels between the pre- and postoperative stages in the IP group (p < 0.001) (Fig. 3).
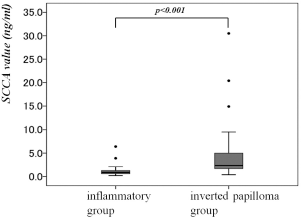
Preoperative serum squamous cell carcinoma antigen (SCCA) levels in the inverted papilloma and inflammatory groups. The serum SCCA level was significantly higher in the inverted papilloma group than in the inflammatory group.

Pre- and postoperative serum squamous cell carcinoma antigen (SCCA) levels in patients with inverted papilloma. The postoperative level was significantly lower than the preoperative level.
Tumor Volume and SCCA Level
The mean (standard deviation) tumor volume measured by MRI was 14.1 ∓ 8.9 cm3. The Spearman rank correlation analyses showed that the correlation coefficient of the preoperative SCCA level and tumor volume in the IP group was 0.522 (p = 0.003) (Fig. 4).
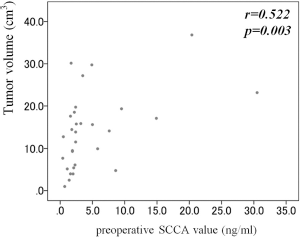
The Spearman rank correlation analysis of tumor volume and the preoperative serum squamous cell carcinoma antigen (SCCA) level. The correlation coefficient of the preoperative serum SCCA level and the tumor volume in the inverted papilloma group was 0.522 (p = 0.003).
SCCA Level in Recurrent Cases
A total of 8 of 30 patients in the IP group received previous surgical treatment and had recurrent lesions. The pre- and postoperative median SCCA levels were 2.0 ng/mL (interquartile range, 1.6–3.0 ng/mL) and 0.9 ng/mL (interquartile range, 0.7–1.2 ng/mL), respectively. The postoperative SCCA concentration was significantly lower than in the preoperative value (p = 0.017) (Fig. 5).
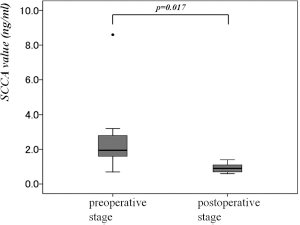
Pre- and postoperative serum squamous cell carcinoma antigen (SCCA) levels in eight patients with recurrent inverted papilloma. The postoperative level was significantly lower than the preoperative level.
Recurrent Cases after Surgery
Only 2 of 30 patients with IP (6.7%) had recurrent lesions after surgery. Both patients had elevated levels of SCCA at the time when the recurrent lesions were found. The clinical course of a representative patient with recurrent IP who received repeated measurements of SCCA levels for early detection of recurrence is shown in Fig. 6. The patient received lateral rhinotomy for removal of IP at another hospital. The preoperative SCCA level and the tumor volume were 8.6 ng/mL and 4.77 cm3, respectively; the SCCA level decreased to 1.0 ng/mL after surgery. After the first operation at our hospital, the patient had three recurrences and received endoscopic surgical resections. The serum SCCA level increased at each recurrence, and, after surgery, the value returned to normal levels. Recurrent lesions could not be detected by MRI or computed tomography but could be detected by endoscopic examination and SCCA level in November 2001 and December 2012.
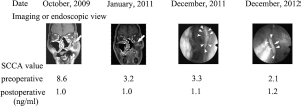
The change in serum squamous cell carcinoma antigen (SCCA) level in relation to tumor recurrence in a representative patient with multiple recurrences. Serum SCCA levels were high at every recurrence. Although magnetic resonance imaging and computed tomographic examination could not detect the small recurrent lesions at the third and fourth operations, the SCCA level was elevated. Endoscopic examination showed small lesions at the third and fourth operations.
SCCA Fluctuation in Patients without IP Recurrence during the Follow-up Period
Of the 28 patients without IP recurrence, 26 received more than two measurements of their SCCA level after surgery; in total, measurements of 115 SCCA levels were carried out in these 26 patients during the follow-up period. The median postoperative serum SCCA level was 1.0 ng/mL (interquartile range, 0.8–1.4 ng/mL). Nine patients (34%) had an SCCA level of ≥1.6 ng/mL at least once after surgery, even without recurrence, whereas only two patients had a postoperative SCCA level of >2.0 ng/mL. There was no significant correlation between the 115 SCCA level measurements and the follow-up period. The preoperative SCCA values were not significantly correlated to the highest value of SCCA during the follow-up period. A postsurgery SCCA level of ≥1.6 ng/mL in IP was observed in 8 of 15 current or ex-smokers (smokers) and 1 of 11 never-smokers. There was a significant difference in a high SCCA level between smokers and never-smokers (p < 0.024, Fisher's exact test).
Multivariable Logistic Analysis of IP
According to the above analysis, variables considered in the models were tumor volume and smoking habit. In multivariate logistic analysis to identify independent risk factors with an effect on preoperative SCCA elevation in these 30 patients with IP, the final model showed that tumor volume was a predictor of SCCA elevation (p = 0.036; odds ratio 1.495 [95% confidence interval, 1.027–2.176]).
Discussion
In our previous study, we found that serum SCCA level measurement is useful for the diagnosis of IP because expression of the SCCA gene is extremely high in this disorder. 10 Matousek et al. 15 subsequently reported similar results. However, because the sample size was relatively small, we included additional patients in the present study and reanalyzed the importance of the measurement of the SCCA level as a diagnostic marker for IP. In the present study, measurement of the SCCA level was found to be very useful for IP detection, with high sensitivity and specificity. IP in the paranasal sinus usually appears as unilateral polyps in the nasal cavity. 8 Although biopsy is the most reliable test for IP, the condition is sometimes accompanied by an inflammatory polyp due to sinus ostium obstruction and so IP cannot always be detected by biopsy of the nasal lesion. Furthermore, it is sometimes difficult to detect recurrent IP because of hyperostosis and marked fibrosis due to previous surgical procedures, as in our representative patient with a recurrence shown in Fig. 6.
The usual diagnostic procedure for IP is endoscopic, imaging, and pathologic examinations. 16 Because the detection rate of IP by using the measurement of the SCCA level is fairly high, measurement of the serum SCCA level is helpful, in addition to the endoscopic, imaging, and pathologic examinations, for diagnosing IP. In this study, respiratory dysfunction and skin disease were not related to SCCA levels in the IP and inflammatory groups. However, smoking habit was significantly associated with SCCA elevations, consistent with a previous report. 17 Smoking habit, respiratory dysfunction, and skin disease should be taken into consideration when evaluating SCCA levels because this study included a limited number of patients with these lesions.
Yasumatsu et al. 18 reported a significant relationship between SCCA levels and the Krouse classification. However, the SCCA level in our previous study 10 was not significantly correlated with clinical characteristics, including the Krouse classification. Because the Krouse staging system is based on tumor location and not tumor size, the relationship between tumor size and SCCA level was investigated in the present study. Despite a lack of correlation between the SCCA level and the Krouse stage, there was a clear correlation between the SCCA level and the tumor volume measured by MRI. Multivariable analysis revealed that tumor volume was a significant predictor for SCCA elevation, which is consistent with the finding of SCCA expression in our previous study. 10 Even small IP lesions that could not be detected by imaging could be detected by SCCA level. Analysis of these results indicated that SCCA level measurement was useful for the early detection of recurrent lesions. However, during the follow-up period, 34% of patients without IP recurrence showed elevated SCCA levels (≥1.6 ng/mL). Because current and ex-smokers tended to have higher SCCA levels than never-smokers, a different cutoff SCCA value for smokers and never-smokers might be appropriate. The current results indicated that 2.0 and 1.5 ng/mL might be suitable cutoff levels for smokers and never-smokers, respectively. To more precisely determine the optimal cutoff value, a future study that recruits a large number of patients is needed.
Conclusion
Serum SCCA is a diagnostic marker for distinguishing new and recurrent IP from inflammatory disease. Because the SCCA level was related to tumor volume, repeated SCCA level measurement after surgery combined with endoscopic, imaging, and pathologic examinations could detect small recurrent lesions. Although respiratory dysfunction and skin diseases were not related to the SCCA level in the present study, these conditions and smoking habit should be considered in the evaluation of the SCCA level.