
Abstract
Background
Initial descriptions of endoscopic approaches to the sella and pituitary involved resecting the middle turbinate (MT) to help improve access and visualization. Modifications of these procedures to preserve the MT have since been described, one rationale being to reduce the incidence of frontal sinusitis. The objective of this study was to establish the incidence of postoperative frontal sinusitis in MT sparing (MTsp) and MT sacrificing (MTsc) approaches to the sella.
Objective
A retrospective cohort study that compared radiographic evidence of frontal rhinosinusitis or frontal recess obstruction after skull base surgery in patients who underwent MTsc and MTsp endonasal approaches to the sella.
Methods
Consecutive retrospective review of pre- and postoperative magnetic resonance imaging from two institutions in geographic proximity but with different approaches to the sella. Mucosal thickening in the frontal sinus was measured and graded by a radiologist blinded to patient cohorts.
Results
Seventy-five patients, based on sample size calculations, were included at each site. Baseline demographics and indications for surgery were not significantly different between the groups. No difference was seen between the groups in the overall grade of radiographic frontal sinusitis seen on postoperative imaging. A total of 8 patients (10%) in the MTsc group had measured mucosal thickening, which was increased from their preoperative scan versus 15 in the MTsp group (20%) (p = 0.10). New mucosal thickening of >1 mm was found in three patients in the MTsc group and eight patients in the MTsp group (p = 0.21); the only patient with postoperative complete frontal sinus opacification was in the MTsp group.
Conclusions
The choice of MTsc versus MTsp in endonasal endoscopic approach to the sella does not seem to make a difference in the incidence of postoperative radiographic frontal sinusitis.
Initial descriptions of endoscopic approaches to the sella involved resecting the middle turbinate (MT) to help improve access and visualization. Several investigators have since described modifications of this procedure to preserve the MT; the rationale being preservation of a normal nasal structure, decreased synechiae, decreased risk of loss of olfaction, decreased frontal sinusitis, and decreased risk of empty nose syndrome. 1
The reality is that little research has been done to compare these two techniques. The risks described above are theoretical and based on experiences with middle turbinectomy in patients with chronic rhinosinusitis, many of which do not demonstrate a higher incidence of adverse outcomes.2–10 Given that the vast majority of candidates for endonasal endoscopic skull base surgery have no history of sinus disease or inflammation in their nasal cavity, this is, in fact, likely not a valid assumption. No studies have been performed that examined this topic in skull base surgery and the issue of iatrogenic frontal sinusitis has not yet been evaluated between the two different approaches to the MT in endoscopic transsphenoidal approaches to the sella. The primary objective of this study was to determine if the type of endonasal endoscopic approach, MT sacrificing (MTsc) versus MT sparing (MTsp), for pituitary and skull base surgery has an effect on the incidence of radiographic frontal sinusitis in patients after surgery.
Methods
A retrospective cohort study was performed at two institutions in geographic proximity but with different approaches to the sella. Research ethics board approval was obtained from both the University of Alberta and the University of Calgary before commencing the study. Potential patients were identified from the respective senior surgeon's (E.D.W., Y.S.) data bases in consecutive series. All the patients who underwent an endoscopic endonasal approach to the sella for pituitary pathology from January 2008 onward were eligible for inclusion.
Surgery at the MTsc site was performed as described by Kassam et al., 3 4 whereas surgery at the MTsp site was done with the modification of MT preservation with outfracture of the MT. 3 5 In regard to the middle turbinectomy, the MT was sacrificed unilaterally from the right side. A MicroFrance Wormald bipolar forceps (Medtronic Canada, Mississauga, Ontario, Canada) was first used to cauterize the MT 5 mm below the axilla. Curved endoscopic scissors were then used to transect the basal lamella back to the insertion on the lateral wall, which was also cauterized with bipolar forceps and allowed for removal of the MT. The patients also were only included if >18 years old at the time of surgery and if postoperative imaging >2 months from the date of surgery was available for review. The patients were excluded if there was a history of previous or concurrent sinus surgery, if postoperative imaging was unavailable, if the frontal sinus was aplastic, or if the converse technique (i.e., MT resection at the MTsp site) was performed. The online charts of candidate patients were examined for eligibility, and demographic data for eligible patients were collected.
Once the sample size was reached, the patient list was completed and the pre- and postoperative magnetic resonance imaging (MRI) for the included patients were retrieved. The images were reviewed by a board-certified radiologist (S.M., T.K.) blinded to patient cohorts, and the maximal thickness of the frontal sinus mucosa was recorded in the study data base and graded as per the grading scale described by Saidi et al. 10 (Fig. 1). The measured mucosal thickening in the frontal sinus was compared between before and after scans, and were used to determine if an increase or decrease in mucosal thickening was seen.
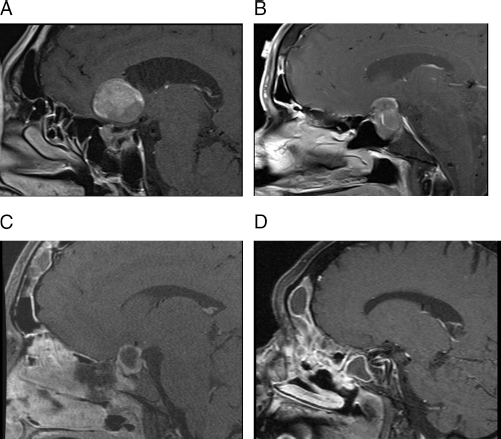
Radiographic evidence of frontal sinusitis scoring (as per Ref. 10). (A) Grade 0, no appreciable thickening. (B) Grade 1, minimal mucosal thickening. (C) Grade 2, heaped-up mucosal thickening.(D) Grade 3, air-fluid levels or complete opacification of the frontal sinus.
Sample size calculation was challenging because, to our knowledge, no studies have been reported in the literature that examined postoperative frontal sinusitis in patients without chronic rhinosinusitis. In patients with chronic rhinosinusitis, many investigators have documented no difference,3,8–10 while others have reported a difference in frontal sinusitis after MT resection. 4 In one retrospective case-control study, the incidence of frontal sinusitis was 75% in cases in which the MT was resected and 45% in those in which it was preserved. 4 Another study that examined findings on MRI found a new onset of frontal sinusitis in ∼11% of cases of partial MT resection. 10 As such, we assumed that there could potentially be, at minimum, an 11% difference in incidence of frontal sinusitis to ensure any difference present was detected. When assuming a two-sided test, an α of 0.05, and a power of 0.8, a total of 70 patients would be required in each group to show a significant difference. The Fisher exact test was used to compare the categorical variable of mucosal thickening whereas the Student's t-test was used for continuous variables with a normal distribution. All statistical analyses were performed with SPSS version 14.0 (SPSS Inc., Chicago, IL), with an α of 0.05 for significance.
Results
A total of 75 consecutive patients who met inclusion criteria were identified and enrolled from each site. The demographic data demonstrated no significant differences between groups. The mean (standard deviation) age was 52 ± 16 years in the MTsc group and 54 ± 17 years in the MTsp group (p = 0.54). There was no significant difference in sex, with 57% men in the MTsc group and 49% men in the MTsp group (p = 0.26). There was no significant difference between the groups in indication for surgery (p = 0.25) (Table 1). A significant difference was present between the two groups in the time between surgical intervention and the postoperative scan. The mean (standard deviation) time to postoperative scan in the MTsc group was 112 ± 53 days, whereas it was 368 ± 272 days in the MTsp group (p = 0.00002).
Indication for endoscopic transsphenoidal surgery

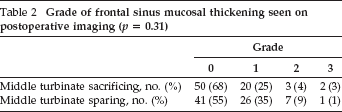
A total of 22 patients (29%) in the MTsc group and 29 patients (39%) in the MTsp group had mucosal thickening in the frontal sinus on preoperative imaging (p = 0.30). The grade of mucosal thickening seen on postoperative imaging in the two groups is outlined in Table 2. There was no significant difference between the two groups in overall postoperative grade of visualized mucosal thickening (p = 0.31). A total of 7 patients in the MTsc group and 16 patients in the MTsp group had an increase in the grade of radiographic frontal sinusitis on their postoperative imaging (p = 0.068). Conversely, 4 patients in the MTsc group and 12 patients in the MTsp group had a decrease in their post-operative grade from their pre-operative one (p = 0.061). There was one new case of grade 3 mucosal thickening in both groups on postoperative imaging (the MTsc group had one case with grade 3 mucosal thickening on both pre- and postoperative imaging, without change).
Grade of frontal sinus mucosal thickening seen on postoperative imaging (p = 0.31)
An increase in the maximal amount of measured frontal sinus mucosal thickening was seen in 15 patients (20%) in the MTsp group and in 8 patients (10%) in the MTsc group (p = 0.10). A total of 5 patients in the MTsc group and 13 patients in the MTsp group had a maximal mucosal thickening of >1 mm on their postoperative MRI (p = 0.12). When only new-onset post-operative mucosal thickening of more than 1 mm was compared, there were three patients in the MTsc group and eight in the MTsp group (p = 0.21). Only one case of new complete frontal opacification after surgery was seen, and it was in the MTsp group.
Discussion
This study demonstrated that there was no significant difference in the degree of frontal sinus mucosal thickening with a MTsc approach to the sella. This finding indicated that sacrifice of the MT for surgical access to the sella does not put patients at increased risk for frontal sinusitis.
Previous studies examined the controversial topic of MT resection thoroughly in the chronic rhinosinusitis disease state. The findings, however, are heterogenous, and recent studies indicate that the impact of MT resection is minimal. This is likely secondary to differences in technique and to refinements in sinus surgery with the addition of the endoscope. Early reports of middle turbinectomy were done with a headlight and polyp snare, often by removing the MT within 5 mm of the skull base.3,4 Studies from the 1990s demonstrated an incidence of frontal sinusitis in patients who underwent middle turbinectomy that ranged from 10 to 75%, which contributed to the dogma that the MT must, by and large, be preserved.4,8 Interestingly, other studies from the same era also demonstrated no significant difference between groups.9,10
Contemporary studies support the latter finding. In 2010, Soler et al. 12 demonstrated, in a retrospective review, that bilateral MT resection provided improved endoscopy scores and olfaction in patients with severe chronic rhinosinusitis, with no difference in quality-of-life scores. A systematic review in 2014 that examined the effect of MT resection identified nine relevant studies, with a combined total of 2123 patients. The pooled results demonstrated no difference in quality of life, nasal resistance, or frontal sinusitis but may actually have demonstrated improved olfaction in patients with a resected MT. 13 It is important to note that the above findings are all relevant to a disease state and that very little has been published on the effect of resection of the MT in the absence of disease.
Although concerns regarding olfaction have also been raised with sacrifice of the MT, previously reported studies on olfaction in transsphenoidal endoscopic approaches have shown otherwise. One prospective study with uniform sacrifice of the MT for access demonstrated no difference in pre- and postoperative olfaction with objective testing. 14 Preservation of olfaction has also been demonstrated with a MTsp approach, 15 but a second study with MT preservation found a significant decrease in olfaction after transsphenoidal skull base surgery, from 37 to 30, on the Smell Identification Test (Sensonics Inc., Haddon Heights, NJ). 16 This is likely due to other cofounders, e.g., the use of a nasoseptal flap and harvesting the flap with monopolar cautery. A general understanding of the role that the MT plays in normal nasal physiology and olfaction is evolving; preserving the middle turbinate, when possible, may help with restoring normal nasal function after surgery and can act as a landmark for future revision surgery. That being said, the above findings should support the surgeon to resect the MT when necessary for improved access.
Both the retrospective nature of this study and the fact that two different surgeons were performing the respective techniques temper the results somewhat. Ideally, a prospective, randomized trial that compares the MTsc versus an MTsp technique would help tease out some of the differences between these two techniques, not only with regard to frontal sinusitis but also for olfaction, postoperative synechiae, crusting, and nasal obstruction, and whether or not sacrifice does indeed improve surgical access. Another important potential confounder in this study was the difference in duration of follow-up imaging after surgery. This difference is largely due to variation in practice patterns between the two sites involved.
This difference in duration, however, is unlikely to be significant because any edema or scarring in the frontal recess would be expected to have occurred by the 2-month mark. Most other studies that examined frontal sinusitis after middle turbinectomy did not comment on the duration of time between pre- and postoperative imaging.3,4,8,10 Data on the use of a nasoseptal flap in reconstruction was not collected. The superior cut in harvesting the flap is routinely below the level of the middle turbinectomy and, hence, unlikely to impact the frontal recess. Also, there is a risk of a type II error based on the sample size calculation because the study was underpowered to detect a difference of <11% between the groups. Nevertheless, the trend seen in increased mucosal thickening was actually toward the MTsp group rather than toward the null hypothesis.
Conclusion
There does not seem to be a difference in incidence of radiographic frontal sinusitis between an endoscopic MTsp and a MTsc approach to the sella. The theoretical risk of frontal sinusitis with MT resection should not stop skull base surgeons from removing the MT to assist with access.