
Abstract
Background
Local allergic rhinitis (LAR) has been observed in patients without atopy. However, LAR is still underdiagnosed in patients with perennial or seasonal nasal symptoms.
Objective
The aim of this study was to determine the prevalence of LAR in young patients with a previous diagnosis of nonallergic rhinitis or suspicion of allergy.
Methods
A total of 121 patients, ages 12–18 years old, with confirmed nonallergic rhinitis and typical seasonal nasal symptoms were examined. Skin-prick tests; serum and nasal specific immunoglobulin E (IgE) measurements; and nasal provocation tests by using grass (Phleum partense), Artemisia, and birch pollens were performed. A control group of age-matched patients with a diagnosis of seasonal allergic rhinitis underwent the same procedures as the test group.
Results
LAR to grass pollen (P. partense), Artemisia, and birch was confirmed in 17 (16.6%), 6 (5.9%), and 9 (8.9%) of patients, respectively. Polyvalent allergy was established in 21 subjects (20.8%): grass and Artemisia, 11 patients (10.9%); and grass and birch, 10 patients (9.9%). The remaining 48 patients (47.5%) were diagnosed with nonallergic rhinitis. The results of the nasal provocation tests and the concentrations of nasal IgE were similar among the analyzed groups. Furthermore, the concentration of nasal IgE increased faster in patients with LAR than in patients with allergic rhinitis; however, this difference was not statistically significant.
Conclusion
LAR is a serious problem in young patients; however, its significance is still unappreciated.
Some patients who experience nasal symptoms typical for allergy cases had negative results for the SPT and the test of serum concentrations of IgE for common inhalant allergens. Regardless of age, results of studies showed that 47 to 62.5% of patients previously diagnosed with either non-AR or idiopathic rhinitis actually have LAR.1,4,5 This could explain the weak effect of rhinitis treatments in these patients. LAR is characterized by the local production of sIgE during natural exposure to aeroallergens.5–7 Typically, these patients have negative results for SPTs and serum sIgE but have positive results for the nasal provocation test (NPT) to aeroallergens.5,6 The aim of this study was to determine the prevalence of LAR in young patients with a previous diagnosis of non-AR or a suspicion of allergy (but with previous negative results for allergy diagnostic procedures) who have typical nasal symptoms during pollen season. The local ethics committee approved the study (Medical University of Silesia, Katowice, Poland, in 2014), and all the participants gave informed consent.
Methods
A total of 166 young patients who experience rhinitis during the summer months and during more than one season were prescreened for this study. However, only 121 patients met the criteria and were selected for further procedures. The inclusion criteria were the following: (1) ages 12–18 years, (2) presentation of clinical nasal symptoms during the pollen season (May–August) that required symptomatic treatment for a minimum of 7 days per season, (3) previous documentation of a negative SPT and/or negative test for serum sIgE for common inhalant allergens (see SPT), and (4) a lack of bronchial asthma. The exclusion criteria were the following: (1) chronic rhino-sinusitis and/or nasal polyposis, and (2) respiratory infections within 4 weeks before the initiation of the study.
Diagnostic Procedures
A clinical questionnaire that examined allergy symptoms, SPT results, serum total IgE and sIgE levels, and nasal sIgE (nsIgE) levels during NPTs were performed. The patients avoided systemic steroids (for 6 months), antihistamines (for 2 weeks), intranasal corticosteroids (for 6 weeks), and vasoconstrictors (for 1 week) before undergoing any study procedures. The control group included young patients with seasonal AR due to grass, birch, or Artemisia allergy, and was compared with the study group. In total, 35 patients had a monoallergy to grass, 11 patients had a monoallergy to birch, and 9 patients had a monoallergy to Artemisia. In addition, 32 patients had allergies to both grass and birch, and 29 patients had allergies to both grass and Artemisia.
Rhinitis Characteristics
According to the Allergic Rhinitis and its Impact on Asthma guide-lines, 2 rhinitis is classified as intermittent (with symptoms present for <4 days per week or for <4 consecutive weeks) or persistent (with symptoms present for >4 days per week or for >4 consecutive weeks). Rhinitis severity is based on estimations of impaired items (including sleep, daily activities, work and/or school performance, and troublesome behavior) and is classified as severe, mild, or moderate. 2
SPT
The SPT was performed with a panel of the following aeroallergens: Dermatophagoides pteronyssinus, Dermatophagoides farinae, Phleum partense, Artemisia, birch, alder, hazel, Alternaria, Cladosporium, Aspergillus, and dog and cat epithelia (Allergopharma, Reinbek, Poland). A positive control (10 mg/mL of histamine) and negative control (saline solution) were included. An allergy was defined as a positive SPT result for at least one allergen with a wheal maximum diameter at least 3 mm larger than that of the negative control. Patients who had negative results for histamine were excluded from further analyses.
Serum and sIgE
Serum total and sIgE levels to the same aeroallergens as those used in the SPT panel were determined by using an fluoroenzyme immunosorbent assay (UniCAP, Uppsala, Sweden). The positive cutoff value for sIgE was >0.35 kU/L.
nsIgE
A bilateral nasal lavage by following the Naclerio method was performed with 6 mL of physiologic saline solution at room temperature. 8 The sample of mucus and saline solution was expelled after 10 minutes. This test was performed in both nostrils. The nslgE against the aeroallergens mentioned above were examined in the supernatant by using immunoassay (UniCAP, Uppsala, Sweden). The detection limit was 0.35 kU/L. These measurements were performed at baseline and at 15 minutes and 1 hour after the NPTs.
NPT
Nasal potency was assessed by acoustic rhinomanometry by using a SRE 2000 rhinometer (Rhinometrics, Lynge, Denmark). These tests were performed according to the guidelines of the Standardization Committee on Acoustic Rhinometry. 9 The NPTs were performed in December and January. By using a meter pump spray, the patients were challenged intranasally with saline solution to exclude nasal hyperreactivity. If the NPT result was negative, then the NPT was performed again 2 weeks later with extracts of the aeroallergens mentioned above (the concentration of each allergen was 5000 SBE/mL; Allergopharma). One hundred microliters of the solution was applied to each nostril in a total volume of both nasal cavities from 2 to 5 cm for acoustic rhinometry, and the results were compared with the baseline test. The immediate reaction was analyzed at 15 minutes, 1 hour, and 6 hours after the application of the solution.
Monitoring of NPT
Nasal symptoms (nasal obstruction, rhinorrhea, itching, and sneezing) were monitored by using the 100-mm horizontal visual analog scale (VAS). Symptom severity was classified as severe (71–100), moderate (31–70), or mild (0–30). The response to an allergen was evaluated at baseline, 15 minutes after saline solution application, and 15 minutes after aeroallergen application by VAS, and in a total volume of 2–6 cm. An increase of ≥30% in the total VAS score and a decrease of ≥30% in the 2- to 6-cm volume was considered a positive response. Both nostrils underwent lavage.
Statistical Analysis
The Statistica computer program version 8.1 (SoftPOl, Cracow, Poland) was used for the statistical analyses. Continuous data are presented as means and standard deviations (SD), and categorical data are presented as percentages. The clinical and demographic data were compared between the groups by using the χ 2 analysis and analysis of variance. The Spearman rank correlation test was used for comparison of nonparametric values; p values of <0.05 were considered statistically significant.
Results
Of the 121 patients, ages 12–18 years, who requested to participate in the study, 115 were accepted and 101 completed the study. The appearance of an exclusion criterion (mainly infection) was the most common reason for discontinuation of study participation. The general characteristics of the patients are shown in Table 1. LAR was diagnosed in 53 patients (52.5%). LAR to grass pollen (P. partense), Artemisia, and birch was confirmed in 17 (16.8%), 6 (5.9%), and 9 (8.9%) patients, respectively. Polyvalent, local allergy was confirmed in 21 subjects (20.8%): grass and Artemisia, 11 subjects (10.9%); and grass and birch, 10 subjects (9.9%). The remaining 48 patients (47.5%) were diagnosed with non-AR. The results of the NPTs and nasal IgE (nsIgE) concentrations were similar between the analyzed groups.
Patient characteristics
SD = Standard deviation; NS = not statistically significant; IgE = immunoglobulin E.
The nsIgE concentration for P. partense increased from a mean (SD) value of 0.23 ± 0.12 kU/L at the baseline to 1.02 ± 0.44 kU/L at 6 hours after NPT in the study group (p ≤ 0.05). This trend was similar in the control group, with a mean (SD) AR from 0.39 ± 0.23 to 0.99 ± 0.67 kU/L (p ≤ 0.05) (Fig. 1). The nslgE concentration to birch increased from a mean (SD) value of 0.3 ± 0.07 to 1.33 ± 0.25 kU/L (p ≤ 0.05) 1 hour after NPT and then decreased at 6 hours in the study group. The nsIgE concentration trend in the control group with AR was similar to that for P. partense, with a mean (SD) increase from 0.16 ± 0.1 to 1.1 ± 0.72 kU/L at 6 hours (p ≤ 0.05) (Fig. 2). Slightly different trends were observed for Artemisia. In the study patients, there was a constant increase of nslgE concentration from a mean (SD) baseline level of 0.31 ± 0.22 to 1.62 ± 0.83 kU/L at 6 hours after provocation (p ≤ 0.05); however, in the control group with ARthe mean (SD) increase of nsIgE was observed until 6 hours after provocation, from 0.41 ± 2.1 to 1.42 ± 0.58 kU/L (p ≤ 0.05). In the first hour after provocation, the differences of nsIgE concentrations between the analyzed groups were statistically significant (Fig. 3).
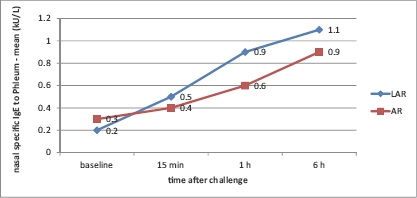
Changes in nasal level of specific immunoglobulin E (IgE) to Phleum during a nasal provocation test.
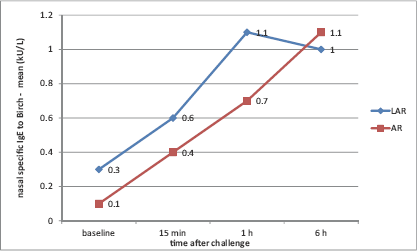
Changes in nasal level of specific immunoglobulin E (IgE) to birch during a nasal provocation test.
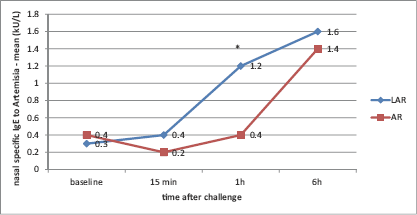
Changes in nasal level of specific immunoglobulin E (IgE) to Artemisia during a nasal provocation test.
Generally, nslgE concentrations increased faster in patients with LAR than in patients with AR, but this difference was not statistically significant except for patients allergic to Artemisia. The detailed results of the allergy diagnostic procedures are presented in Table 2. The VAS score was not significantly different between the two types of AR (local or not local) or between the different types of allergens. Clinical responses during the NPT were associated with a significant increase in nslgE (R = 0.74, p ≤ 0.05, Spearmen correlation test).
Comparison of the frequency of positive results for the SPT, sIgE, nsIgE, and clinical NPT in patients with LAR and AR (common allergens)
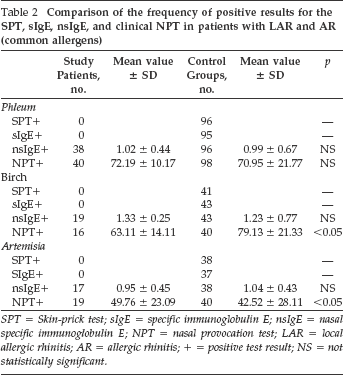
SPT = Skin-prick test; sIgE = specific immunoglobulin E; nsIgE = nasal specific immunoglobulin E; NPT = nasal provocation test; LAR = local allergic rhinitis; AR = allergic rhinitis; + = positive test result; NS = not statistically significant.
Discussion
Rhinitis is a common health problem.2,10 However, it is frequently incorrectly diagnosed and is commonly treated with symptomatic drugs, e.g., decongestants.2,11 The results obtained in this study confirmed the presence of LAR in ∼53% of the patients who were analyzed, all of whom were previously diagnosed incorrectly. This result was consistent with other observations of a group of patients with typical symptoms but with negative SPT results and serum concentrations of IgE.1,4 Our results demonstrated the clear correlation between seasonal nasal symptoms and nasal local reactions to common inhalant allergens in more than half of the studied patients. Unfortunately, there are no clear epidemiologic data for how many patients with LAR exist.
We confirmed that the typical phenotype of seasonal AR does not correspond with the typical positive systemic IgE reaction. The detection of local sIgE, which was observed during NPTs with dynamic changes after exposition of allergens, confirmed an allergic local response. Similarly, the problem of underdiagnosis of LAR in patients with seasonal allergic nasal symptoms and a negative allergy diagnosis was previously revealed by Rondon. 1 However, more observations have been made among patients with perennial nasal symptoms.7,12,13
The mechanism of LAR is known. The local IgE-secreting B-cell and plasma cell populations increase up to several-fold compared with the blood cell population, whereas the total number of these cells remains relatively constant. This pattern reflects the ongoing processes of class switch recombination and differentiation of the B cells into plasma in situ. Antigens stimulate allergen-specific B cells that express antibodies for other isotypes to undergo local heavy-chain switching to IgE in the tissue.7,14,15
The results of this study showed that the underestimation of LAR was also a significant problem in young patients (100% of patients in the study group had a previous false diagnosis). Some studies explored this topic4,16,17; however, information regarding LAR in children, especially local seasonal rhinitis, is lacking. LAR diagnosis is difficult to confirm in some patients. Positive results of nasal challenge and negative results of SPT and sIgE levels can confirm LAR.4,18,19 Unfortunately, false-positive provocation tests and symptoms of nasal hyperreactivity are sometimes observed, especially in young patients, which can reduce the probability of assigning a correct diagnosis.
For this reason, in this study, an additional nasal lavage was performed, and nsIgE concentrations were examined after allergen provocation. In the majority of patients, nsIgE concentrations increased after NPT, which confirmed the diagnosis of LAR. A significant increase in nsIgE at 6 hours after challenge was observed. A previous study of the D. pteronyssinus allergen made a similar observation. 20 In the present study, a slight difference in the dynamic increase in nsIgE concentrations was observed in the control group compared with the study group; however, the total reactivity of the nasal mucosa was very similar between the two groups.
A limitation of this work was the short observation period after the provocation tests. It would be interesting to observe clinical late reactions at 12 and 24 hours after provocation, as described by Rondon et al. 18 Other investigators also detected only the first-phase reaction,21,22 which was sufficient to make a diagnosis of LAR. It seemed to be easier to perform such short diagnostics in clinical practice. Moreover, analysis of the data indicated that the most patients exhibited reactions between 15 minutes and 6 hours, and only a subset of them exhibited a late reaction.1,20,22 The examination of nsIgE excluded many ambiguous results; however, in daily practice, this examination could have significant technical problems and was time consuming, especially in patients suspected of being allergic to multiple allergens. However, in some subjects with severe rhinitis that is not effectively controlled by treatment, nsIgE diagnostic examinations could help resolve treatment issues. Interestingly, the rates of nsIgE increase in patients with AR and LAR were different. This may emphasize the difference between these two forms of the disease in terms of the immune response.
Another limitation of this study was the lack of other monitoring parameters, such as tryptase, eosinophil cationic protein, or cells in nasal lavage. However, these parameters exhibited good correlation with nsIgE and clinical symptoms, and are not decisive for the final diagnosis of LAR.18,21,22 The results obtained here indicated the importance of NPTs as an initial diagnosis of LAR in patients with typical allergic symptoms and negative SPTs and serum IgE values. In the present study, eosinophil counts in nasal mucosa during provocation tests brought inconclusive results and, therefore, were not included here; however, most investigators did not use this method in LAR diagnoses. This method is useful for eosinophilic rhinitis recognition. However, there were no such patients in this study.
Conclusion
AR and LAR are significant problems, even in young patients and in those with seasonal symptoms; however, their significance in young patients is still unappreciated. Nasal lavage with nsIgE concentration significantly increases the reliability of LAR diagnosis.
Footnotes
The authors have no conflicts of interest to declare pertaining to this article