
Abstract
Background
In the field of otolaryngology, oral corticosteroids (OCS) are widely prescribed for rhinosinusitis. Although there is evidence in the literature regarding specific OCS dosing protocols, it is not known to what extent these recommendations are being followed.
Objective
To examine the current state of OCS prescribing habits for rhinosinusitis by American Rhinologic Society members.
Methods
An anonymous online survey was sent to all American Rhinologic Society members. Dosing, frequency, tapering, and overall prescribing habits for OCS were assessed in chronic rhinosinusitis with polyposis (CRSwP) and in chronic rhinosinusitis without polyposis and acute bacterial rhinosinusitis. The CRSwP group was subdivided into aspirin-exacerbated respiratory disease, allergic fungal sinusitis, and not otherwise specified. Results were compared with current guidelines. Descriptive statistics were used to analyze data.
Results
Ninety-three surveys were completed (response rate, 12.9%). Prednisone was the most common OCS prescribed. In the CRSwP-aspirin-exacerbated respiratory disease group (n = 86), the median starting dose was 60 mg (range, 4-80 mg) and the average duration was 8 days (range, 2-28 days). In the CRSwP-allergic fungal sinusitis group (n = 81), the median starting dose was 50 mg (range, 20-60 mg), and the average duration was 6 days (range, 2-35 days). In the CRSwP-not otherwise specified group (n = 84), the median starting dose was 50 mg (range, 20-80 mg) and the average duration was 5 days (range, 1-21 days). OCS were prescribed for chronic rhinosinusitis without polyposis and acute bacterial rhinosinusitis by 66.0 and 62.4% of respondents, respectively.
Conclusion
Significant heterogeneity existed in OCS prescribing habits for rhinosinusitis. Discrepancies were observed between survey results and evidence-based recommendations. Developing standardized OCS treatment protocols for rhinosinusitis may improve the quality of care by optimizing clinical outcomes and reducing the risk of complications.
Oral corticosteroids (OCS) are commonly used to treat a variety of inflammatory conditions. In the field of otolaryngology—head and neck surgery, OCS are frequently prescribed to treat a range of conditions, with rhinologic indications among the most common. 1 In the treatment of rhinosinusitis, OCS therapy is considered part of standard medical therapy. 2 Specifically, recent appropriateness criteria require a short (i.e., 1-3 week) OCS course before a patient with uncomplicated chronic rhinosinusitis (CRS) with polyposis (CRSwP) becomes a candidate for endoscopic sinus surgery. 3 Despite widespread use, it is imperative to recognize that OCS have an array of potential adverse effects, such as psychosis, decreased bone density, metabolic disturbances, insomnia, irritability, avascular necrosis of the hip, and cataracts.4–8 Because a correlation exists between the presence of adverse effects and increasing OCS dose, physicians should endeavor to prescribe the minimal effective dose of OCS, thereby maximizing clinical benefit while minimizing potential harm.4–8
Despite recommendations for the use of OCS during management of CRSwP and limited evidence for use in CRS without polyposis (CRSsP) and acute bacterial rhinosinusitis (ABRS), there are no recommendations of what would be considered a “standard” dose and duration of OCS therapy for these conditions. The purpose of this study was to examine the OCS prescribing practices of American Rhinologic Society (ARS) members during the management of acute rhinosinusitis and CRS, and compare the results to current practice guidelines and evidence-based reviews for OCS. Outcomes from this study will define the degree of heterogeneity in OCS prescribing habits and assist in the development of a standardized evidence-based approach to the prescribing of OCS during management of rhinosinusitis.
Methods
A cross-sectional survey was performed after Health Sciences Research Ethics Board approval was received from Western University (London, Ontario, Canada) (file 107184). Inclusion criteria were being an active member of the ARS and completion of the entire questionnaire. The Web-based questionnaire was developed through the online software platform QuestionPro (San Francisco, CA) and took ∼10 minutes to complete. An e-mail with a link to the survey was sent to the entire ARS mailing list. A modified Dillman approach was used with a reminder e-mail sent to the ARS membership 2 weeks after the first e-mail. The questionnaire began by collecting demographic information from the respondents, including location of training and practice, type of fellowship, experience with inflammatory sinonasal disease, and resources involved in OCS prescribing regimens (see Supplemental Appendix 1). The survey was then truncated into groups of questions that focused exclusively on the prescribing habits of OCS for various subtypes of rhinosinusitis: ABRS, CRSsP, and CRSwP divided into the subtypes of aspirin-exacerbated respiratory disease (CRSwP-AERD), allergic fungal sinusitis (CRSwP-AFS), and undifferentiated polyposis (CRSwP-NOS). Answer options were in the form of yes or no, multiple choice, ranking, and free text. Data were evaluated by using descriptive statistical analyses in Microsoft Office Excel 2011 (Microsoft Corp., Redmond, WA). Dosage of OCS, if not prednisone, was converted to the equivalent dosage of prednisone for ease of comparison.
Results
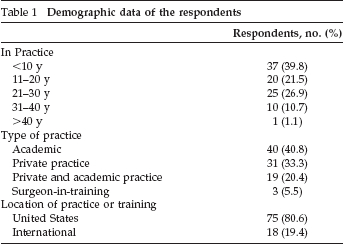
The survey was sent to 842 members of the ARS; 723 individuals met eligibility criteria. Ninety-three surveys were completed, which gave a response rate of 12.9%. The demographic breakdown of respondents is outlined in Table 1. The majority of respondents were in active practice (88.2%) and more than half (54.0%) had completed fellowship training in rhinology and anterior skull base surgery. There was a preponderance for American-trained (76.4%) and practicing (80.6%) otolaryngologists. A total of 19.4% of respondents were practicing internationally, which was comparable with the 12.1% of ARS members who are outside the United States. The most common location of international members was Canada (14.0%), followed by Australia (7.5%). The approximated frequency of sinonasal inflammatory disease managed in each respondent's practice is illustrated in Fig. 1. Nearly three-fourths of the respondents indicated that at least half of their practice consisted of treating sinonasal disease-related issues. The most influential resources used in the development of OCS prescribing habits are shown in Fig. 2. The most common resource for prescribing habits was mentorship (41.0%), followed by personal experience (33.0%). The most frequently reported indication for OCS use in all CRSwP subtypes and ABRS was “symptomatic relief.” A trial of “maximal medical therapy” was the most common indication in CRSsP (Table 2). Preoperative OCS utilization was much less common in ABRS (7.0%) and CRSsP (15.7%) when compared with CRSwP subtypes.
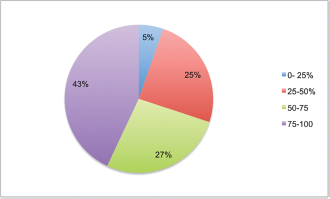
Percentage of respondent's practice dedicated to sinonasal inflammatory disease.
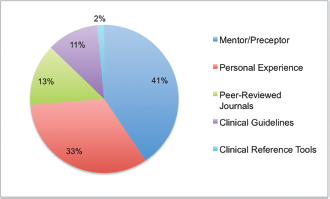
Top ranked resource for respondent's development of oral corticosteroid dosing habits.
Demographic data of the respondents
Primary reported indication for the initiation of OCS therapy in the various rhinosinusitis subtypes
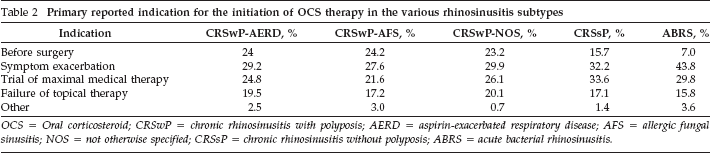
OCS = Oral corticosteroid; CRSwP = chronic rhinosinusitis with polyposis; AERD = aspirin-exacerbated respiratory disease; AFS = allergic fungal sinusitis; NOS = not otherwise specified; CRSsP = chronic rhinosinusitis without polyposis; ABRS = acute bacterial rhinosinusitis.
Across all conditions, the most commonly prescribed OCS was prednisone (84.3%) taken once daily (86.5%). As is evident in Table 3, considerable variation in the starting dose and duration of OCS existed for each condition. The median starting dose ranged from 25 mg (ABRS) to 60 mg (CRSwP-AERD), with a mean initial dose duration from 5 days (CRSwP-AERD, CRSsP, and ABRS) to 8 days (CRSwP-AERD). The number of unique starting doses as a function of quantity and duration can be seen in Figs. 3 and 4, respectively. With regard to the amount of OCS initially prescribed, CRSwP-AERD had the largest variability, with 10 unique starting doses described by respondents. With respect to the duration of initial OCS prescribed, the greatest variability was observed in CRSwP-AFS, with 14 different durations outlined. The majority of respondents (87.3% overall) used an OCS taper; however, the duration of taper varied extensively across the conditions and subtypes. A taper of <7 days was used in ABRS (65.2%), followed by CRSwP-AFS (22.0%) and CRSwP-AERD (21.9%). Taper duration of >14 days was highest in CRSwP-AFS (39.0%), followed by CRSwP-AERD (37.6%) and CRSwP-NOS (33.8%). Long-term dosing (>4 weeks) was highest for CRSwP-AERD (22.1%), followed by CRSwP-AFS (16.0%). The most frequently used antibiotic with an OCS regimen was amoxicillin-clavulanic acid. Respondents most commonly prescribed antibiotics for CRSsP (88.5%) and ABRS (87.7%). Overall, an excess of 120 unique prescribing regimens were used among respondents when OCS starting dose, duration, and taper were considered.
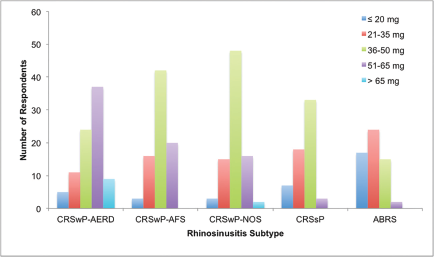
Variation in oral corticosteroid starting dose amounts among respondents across rhinosinusitis subtypes.
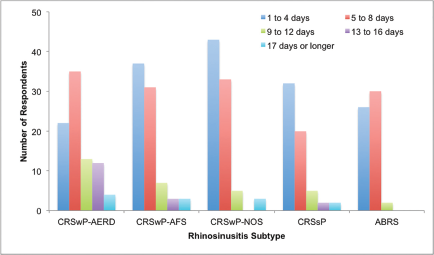
Variation in oral corticosteroid starting dose duration among respondents across rhinosinusitis subtypes.
Initial OCS dosing for rhinosinusitis subtypes
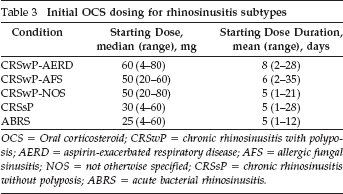
OCS = Oral corticosteroid; CRSwP = chronic rhinosinusitis with polyposis; AERD = aspirin-exacerbated respiratory disease; AFS = allergic fungal sinusitis; NOS = not otherwise specified; CRSsP = chronic rhinosinusitis without polyposis; ABRS = acute bacterial rhinosinusitis.
Discussion
This study has characterized the OCS prescribing habits of respondent ARS members for acute rhinosinusitis and CRS, and has demonstrated significant heterogeneity in prescribing habits. This study was done to broaden the scope of the findings of Ansari et al., 9 who surveyed Canadian otolaryngologists on this issue. Further research into the optimal OCS dose and duration will aid physicians in optimizing efficacy and adherence to therapy while minimizing potential harm to patients from over- or underprescribing OCS.
With respect to CRSsP, a systematic review done by Lal and Hwang 10 noted that no randomized control trials exist that investigated OCS monotherapy because antibiotics or nasal corticosteroids were often studied in combination. Expert committee recommendations for CRSsP have been published.11,12 The American Academy of Allergy, Asthma & Immunology has recommended prednisone 60 mg once daily for 10-12 days without a taper as second-line therapy, after initial treatment with antibiotics and topical steroids. 11 The British Society of Allergy and Clinical Immunology recommended prednisone 0.5 mg/kg orally for 5-10 days, again without a taper. 10 Recent systematic reviews published by Rudmik and Soler 13 and Poetker et al. 5 gave only level C recommendations for the use of OCS in CRSsP secondary to the weak body of evidence and paucity of randomized control trials. Neither review gave concrete guidance regarding specific dose or duration of treatment; however, Poetker et al. 5 noted that three of the four identified studies used prednisone, which ranged from 40 to 60 mg for 10-14 days, and all three used a rapid taper. 3 With regard to the initial OCS dose for CRSsP by the ARS membership surveyed, there were seven unique starting doses used over 12 different treatment periods.
In evaluating the use of OCS during the management of CRSwP-AFS, a review article by Lal and Hwang 10 reported some support for perioperative OCS use. Perioperative dosing regimens ranged from 0.5 mg/kg to 50 mg over 10-42 days. In the double-blind randomized control trial by Rupa et al., 14 patients with CRSwP-AFS who underwent endoscopic sinus surgery received 50 mg daily for 6 weeks after surgery, followed by a 6-week tapering period. Although symptoms and endoscopic examinations were improved in the OCS group compared with placebo, all the patients in the experimental group experienced significant adverse effects from the oral corticosteroid. 11 In this study, the indications for OCS use in CRSwP-AFS were symptom exacerbation, preoperative use, and trial of maximal therapy. Furthermore, respondents described several unique treatment regimens, including seven different doses over 14 different durations.
For CRSwP-AERD, a review by Simon et al. 15 described OCS being used to perform a “medical polypectomy”; however, efficacy of this was shown to vary with histology. Specifically, eosinophil-rich polyp tissues have been shown to respond better to OCS therapy than to neutrophil dominant or mixed types of polyps. A prospective cohort study by Wen et al. 16 demonstrated a reduction in the level of eosinophilia in nasal polyps with prednisone (30 mg daily for 7 days). Although this study did not examine CRSwP-AERD specifically, the results may translate into a reduced illness severity for these patients. We did not identify any studies that exclusively evaluated OCS use during management of CRSwP-AERD. Outcomes from our study demonstrated that, among all CRS subtypes, CRSwP-AERD had the highest median starting dose (60 mg), widest range (4-80 mg), and longest mean duration (8 days). Furthermore, some of the reported starting doses of OCS for CRSwP-AERD were higher than those used in published evidence. For CRSwP-AERD, respondents reported 10 different starting doses and 12 different durations for OCS therapy.
Expert opinion guidelines recommend brief OCS use for large polyps (CRSwP-NOS) but in combination with topical nasal corticosteroids.12,17 The OCS dose and duration suggested by the British Society of Allergy and Clinical Immunology was 0.5 mg/kg of prednisolone for 5-10 days. 12 Another group of experts discussed a 4-week course of OCS for mild-to-moderate CRSwP-NOS but only if no improvement is observed after 3 months of topical therapies. 18 For severe CRSwP-NOS, this same committee endorses immediate OCS initiation for 4 weeks in combination with topical corticosteroids. These recommendations are based on six randomized placebo-controlled trials; however, there is significant variation among methodology and sample populations in these studies, which weakens the strength of recommendations. Initial OCS doses (25-50 mg) and treatment durations (14-20 days) were variable across the studies.18–25 There also was a question about the utility of long-term (>12 weeks) OCS dosing in CRSwP-NOS when the literature is considered.5,23 For CRSwP-NOS, respondents reported nine different starting doses and 13 different durations for OCS therapy.
In a recent Cochrane review, OCS were found to have no benefit over placebo as a treatment modality for ABRS. 24 The British Society of Allergy and Clinical Immunology has a grade D recommendation for the use of OCS in ABRS. 12 In 2012, Venekamp et al. 24 conducted a randomized, double-blind, placebo-controlled trial in primary care practices that found no clinically relevant effect of OCS in the treatment of uncomplicated acute rhinosinusitis. Although the study did not specifically evaluate ABRS, the limited improvement indicated that, in acute processes, whether viral or bacterial, OCS may not be clinically useful. 24 In 2015, Rosenfeld et al., 26 published revised guidelines, which suggest a period of watchful waiting (up to 7 days) rather than OCS or antimicrobial therapy. Despite the lack of literature in support of OCS and antibiotics in combination, a majority of respondents (61.3%) in this survey prescribed OCS with antimicrobials for ABRS. A Cochrane review in 2014 concluded only minimal symptomatic benefit from this combination and an increase in adverse effects, such as nausea, vomiting, and gastric upset. 24 Specifically, with respect to initial OCS therapy for ABRS, the respondents described eight different doses and eight different durations. The use of OCS in this treatment scenario, given the limited efficacy and evidence against utility in clinical trials, exposes patients to potential harmful adverse effects with limited established benefit.
A potential weakness of the questionnaire was the inability of the respondents to specify the severity of the individual condition. Often times when otolaryngologists are debating OCS therapy for a patient, they not only consider their clinical examination but also their general gestalt and sense from the patient. One could argue that the initiation of steroid therapy in rhinosinusitis is done on a case-by-case basis, and this was certainly something that our survey could not elucidate. The survey had a low response rate, which could, in part, be a result of the length of the survey; however, attempting to tease out the subtleties of prescribing habits for different types of CRSwP required a longer survey to ask the needed questions. The response rate, however, was similar to other published ARS surveys.27,28 Despite a slightly lower response rate, most respondents were practicing otolaryngologists with subspecialty training in rhinology, which does limit the generalizability of our results. Conversely, one would expect less variability and nonadherence to guideline recommendations in an expert group such as this. The heterogeneity seen suggests more work should be done to tease out the optimal OCS dose to maximize benefit and minimize side-effects in patients with rhinosinusitis.
Conclusion
Otolaryngologists frequently prescribe OCS for various forms of rhinosinusitis. This study characterized the OCS prescribing practices of ARS members with respect to CRSwP subtypes, CRSsP, and ABRS. The variability among respondents in prescribing practices is consistent with the heterogeneity that currently exists in the literature. Many of the dosages and durations of OCS therapy that were reported were not congruent with established evidence, in particular, with the use of OCS in ABRS. Further research is needed to develop standardized evidence-based OCS treatment algorithms with the goal of maximizing clinical benefit and reducing potential adverse events.