
Abstract
Background
The endoscopic modified Lothrop (Draf-III) surgery has improved treatment of recalcitrant frontal sinus disease, with favorable safety and long-term results. However, the short-term clinical and quality-of-life morbidity after Draf-III relative to less-extensive procedures has yet to be investigated.
Objective
To evaluate the surgical and quality-of-life outcomes, including the burden of follow-up care, in patients who underwent endoscopic modified Lothrop (Draf-III), and compared these results with a less-extensive intervention, the endoscopic frontal sinusotomy (Draf-IIa).
Methods
A retrospective review of early (<8 weeks) postoperative recovery of patients who underwent Draf-III (2014 to 2016) for chronic rhinosinusitis was conducted and compared with age and radiographically matched Draf-IIa controls. Primary outcomes included perioperative complications, the number of postoperative clinic visits, debridements, and steroid and antibiotic therapy days. Secondary outcomes included the change in the 22-item Sino-Nasal Outcome Test (SNOT-22) scores and/or subscores (domains).
Results
Thirty-eight patients (19 Draf-III, 19 Draf-IIa) were included. Patients who underwent Draf-III versus Draf-IIa required more postoperative clinic visits (4.9 ±1.7 versus 3.3 ± 0.8; p < 0.05), debridements (4.2 ± 2.0 versus 2.3 ± 0.8; p < 0.05), and antibiotic therapy days (24.4 ± 11.8 versus 15.6 ± 6.3; p < 0.05). The mean (SD) SNOT-22 scores improved for both groups (−12.7 ± 34.5 versus -9.5 ± 20.4; p = 0.74) over the follow-up period, and subscore (domain) analysis demonstrated worsening extranasal symptoms (2.5 ± 3.0 versus -1.5 ± 4.7; p < 0.05) at the first postoperative visit, and less improvement in ear/facial symptoms at the second (−0.5 ± 2.6 versus -3.9 ± 4.7; p = 0.03) and third postoperative visits (−1.1 ± 1.6 versus 3.5 ± 3.3; p = 0.01).
Conclusion
Draf-III is associated with more postoperative clinic visits, debridements, and antibiotic therapy days. The patients who underwent Draf-III demonstrated worsening of extranasal symptoms at the first postoperative visit and less improvement in the ear/facial score at the second and third visits. Informed consent and counseling patients who may require Draf-III should include a detailed discussion of the burden of postoperative care and recovery.
The development of endoscopic sinus surgery has been an invaluable tool in the management of frontal sinus disease by facilitating access with less morbidity than conventional obliteration techniques.1,2 Improved instrumentation and understanding of the frontal sinus anatomy has resulted in a spectrum of endoscopic procedures aimed at restoration of drainage pathways and delivery of topical therapies. Although a substantial cohort of patients with chronic rhinosinusitis (CRS) and with frontal disease will respond durably to endoscopic frontal sinusotomy (Draf-IIa), treatment failures or patients at risk for re-stenosis are sometimes addressed with more-extensive procedures. One such procedure is the endoscopic modified Lothrop, or Draf-III, which involves drilling away bilateral frontal sinus floors and the intersinus septum.2–4
Recent literature demonstrated remarkable long-term efficacy of Draf-III for surgical salvage after Draf-IIa failure in patients with even the most severe CRS phenotypes. 5 Innovations in surgical technique, e.g., the outside-in approach, also decreased the time and effort associated with this procedure.6,7 The favorable outcomes data, coupled with increased accessibility, lowered the threshold for performing this procedure and raised the possibility of primary Draf-III for patients who were medically recalcitrant and with clinical subtypes that may predispose to Draf-IIa failure (e.g., aspirin-exacerbated respiratory disease [AERD]).7,8 Although the risk of surgical failure must be weighed against the anecdotally more-burdensome postoperative course associated with a Draf-III procedure, the short-term postoperative morbidity after Draf-III relative to Draf-IIa has yet to be investigated, which limits the information available for preoperative counseling regarding treatment expectations. The present study was a retrospective review of the early postoperative course of patients who underwent Draf-III compared with age and radiographically matched patients who underwent the less-extensive Draf-IIa.
Methods
Study Population
A retrospective review of adult patients (≥18 years old) who underwent elective Draf-III between 2014 and 2016 was conducted and compared with patients who underwent Draf-IIa at our institution. Draf-III was selected for patients who had medically recalcitrant disease and for whom previous Draf-IIa failed or those with anatomic or clinical subtypes that may predispose to Draf-IIa failure. The clinical data were reviewed for 8 weeks after surgery for each patient, and the duration of the follow-up was determined by the last clinical visit within this period. Quality of life was assessed before surgery and at four time intervals within the follow-up period. All the surgeries were performed by the senior investigator (A.S.D.). The patients who did not complete preoperative baseline computerized tomography (CT) or who underwent both Draf-IIa and Draf-III procedures within the study period were excluded. The study was approved by the University of California, San Diego Institutional Review Board (161005X).
Case-Control Selection
Patients who underwent Draf-III were identified and matched by age (±3 years) and Lund-Mackay score (±4 points) to those who underwent Draf-IIa, as previously described. 9
Baseline Lund-Mackay CT Scoring
The preoperative CTs were reviewed, and scores were assigned based on previously described methods. 10 Specifically, the maxillary, anterior ethmoid, posterior ethmoid, sphenoid, frontal sinuses, and the ostiomeatal complex were evaluated on the right and left, and the severity of sinus mucosal inflammation or fluid accumulation was scored as 0 (no opacification), 1 (partial opacification), or 2 (complete opacity). The range of scores was 0 (least severe) to 24 (most severe).
Clinical and Quality-of-Life Measures
The medical records, including pre-, post-, and intraoperative notes over the study period (<8 weeks after surgery) were reviewed. These data included the number of clinic visits, antibiotic and steroid treatment, debridements, and any perioperative complications. The decision for antibiotic and steroid treatment was determined by the findings of purulence and edema, respectively, on nasal endoscopy. The 22-item Sino-Nasal Outcome Test (SNOT-22) scores and domains were reviewed before surgery and at four postoperative time points within the follow-up period (frequency of intervals described below). 11 In cases of missing data, the mean score within the specific domain was used to replace the value.
Follow-up Time Interval
Routinely, all the patients who undergo frontal sinus surgery are scheduled for three visits within the first 4-6 weeks after surgery and return for a fourth and final visit 3 months later, provided the clinical and endoscopic outcomes demonstrate consistent improvement. Patients who require additional debridement or who demonstrate a postoperative infection are brought back sooner, within 1-3 weeks of the third visit, for an additional visit. Indications for debridement included the presence of crust or clot, retained secretions, or synechia and/or scar formation within the previously operated sinus cavity. For purposes of this analysis, the postoperative visits were based on the following categorization: 0-12 days (postoperative visit 1), 13-24 days (postoperative visit 2), 25-36 days (postoperative visit 3), and 37-48 days (postoperative visit 4) based on the follow-up schedule as described, and accounted for variation in surgeon and patient availability and/or scheduling. A comprehensive clinical review, including nasal endoscopy and quality-of-life assessment, was performed at each encounter.
Surgical Technique
All the procedures were performed with the patient under general anesthesia and with the use of image guidance (Medtronic Fusion ENT Navigation System, Medtronic, Fridley, MN) and involved the placement of Merocel standard nasal dressings (Medtronic, Fridley, MN) and Propel Mini (Intersect ENT, Menlo Park, CA) steroid-releasing implants in the middle meatus and frontal recess, respectively (each side).
Draf-III
The Draf-III was performed via an outside-in approach. 6 This began by creating a septal window that started at the midpoint of the middle turbinate inferiorly ∼1 cm anterior to the free edge. The mucosa was elevated in a submucoperiosteal plane posteriorly until the first olfactory fiber was visualized on both sides of the skull base. The mucosa over the bilateral frontal processes of the maxilla were then exposed. A high-speed, 5 mm, 15° diamond bur (1885076HSE; Medtronic) was then used to drill to the lateral extents of the Draf-III (periosteum of the radix). Once a small patch of periosteum was exposed laterally, the floor of the frontal sinus was removed with a drill, along with the intersinus septum. Hand instruments and the microdebrider were then used to connect the frontal recess to the neo-ostium. The superior-anterior attachments of the middle turbinates were resected as well, and stopped just short of the skull base.
Draf-IIa
The Draf-IIa was completed exclusively with hand instruments and an angled microdebrider, with the goal of complete removal of frontoethmoidal cells with mucosal preservation The frontal sinusotomy always began by taking the axilla superiorly with a frontal sinus punch (Cobra punch). All frontoethmoidal cells were then removed systematically with a variety of angled instruments to crush bone and an angled microdebrider to sharply remove the soft tissue and morselized bone under direct visualization with a 70° endoscope. The Draf-IIa dissection, regardless of the frontoethmoidal anatomic variation, always involved complete removal of frontoethmoidal cells from posterior table of the frontal sinus to the frontal beak in an anterior-posterior axis and from lamina to skull base, laterally to medially, respectively. All the controls underwent bilateral frontal Draf-IIa.
Statistical Analyses
Group differences in demographic variables were assessed by using χ 2 tests of association. Independent sample t-tests were used to analyze differences in the mean score change between the Draf-IIa and Draf-III groups (significance α = 0.05).
Results
Patient demographics and characteristics of the 38 patients included (19 Draf-III, 19 Draf-IIa) are shown in Table 1. The two groups had a similar distribution of demographics, comorbidities, including polyps, asthma, aspirin intolerance, history of depression, and tobacco use. CRS with nasal polyps was a more common indication for Draf-IIa versus Draf-III (42.1 versus 5.3%; p = 0.02), whereas AERD was a more common indication among patients who underwent Draf-III, compared to Draf-IIa (26.3 versus 0%; p = 0.03). The patients who underwent Draf-III more commonly had a previous sinus surgery versus Draf-IIa (84.2 versus 31.6%; p = 0.03). All of the patients who underwent Draf-IIa underwent full (maxillary, ethmoid, sphenoid, and frontal) surgery compared with 15 of 19 (79%) of the patients who underwent Draf-III. Both patients who underwent primary Draf-III initially presented with extensive frontal sinus pathology, specifically AERD and large frontal mucocele, which required more extensive dissection for exposure to completely address the underlying pathology and minimize the need for additional procedures by creating a large common midline drainage pathway. Preoperative overall, and frontal-specific (2.5 ± 1.3 and 2.0 ± 1.6; p = 0.32) mean Lund-Mackay scores were similar between Draf-III and Draf-IIa groups, respectively (Table 1). Although overall preoperative mean SNOT-22 scores were similar between Draf-III and Draf-IIa groups (44.1 ± 27.6 and 36.3 ± 25.4, p = 0.37); patients who underwent Draf-III demonstrated higher baseline psychological dysfunction versus Draf-IIa (13.9 ± 11.1 versus 6.8 ± 6.6; p = 0.02).
Patient characteristics
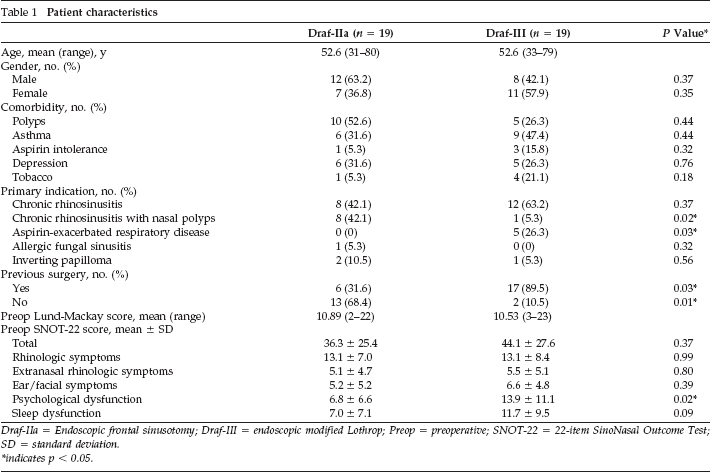
Draf-IIa = Endoscopic frontal sinusotomy; Draf-III = endoscopic modified Lothrop; Preop = preoperative; SNOT-22 = 22-item SinoNasal Outcome Test; SD = standard deviation.
indicates p < 0.05.
Comparison of the mean change from baseline SNOT-22 scores
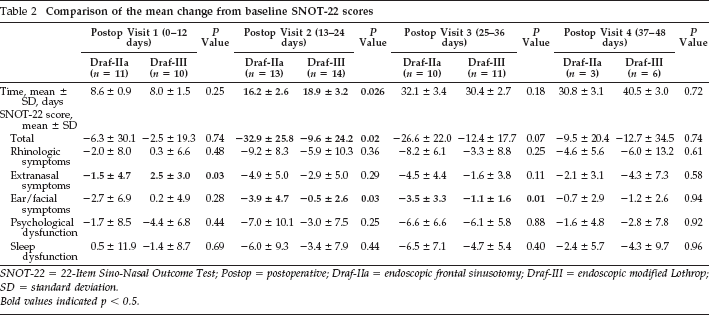
SNOT-22 = 22-Item Sino-Nasal Outcome Test; Postop = postoperative; Draf-IIa = endoscopic frontal sinusotomy; Draf-III = endoscopic modified Lothrop; SD = standard deviation.
Bold values indicated p < 0.5.
The total mean duration of follow-up was similar between the groups, (5.3 ± 2.0 weeks versus 4.9 ± 2.0 weeks; p = 0.53). The patients who underwent Draf-III had significantly more mean follow-up clinic visits than did the patients who underwent Draf-IIa (4.9 ± 1.7 versus 3.3 ± 0.8; p < 0.005), debridements (4.2 ± 2.0 versus 2.3 ± 0.8; p < 0.005), and antibiotic treatment days (24.4 ± 11.8 days versus 15.6 ± 6.4 days; p < 0.05). The patients who underwent Draf-III had more complications than those who underwent Draf-IIa, all of which were epistaxis and required evaluation and control in the emergency department (three events versus one event; p = 0.73). The mean change in SNOT-22 scores from baseline to each time point and for each subscore are summarized in Table 2.
Although the mean pre-operative and post-operative SNOT-22 scores were higher than Draf-IIa at each time point, the mean scores improved for both groups over the follow-up duration (−12.7 ± 34.5 for Draf-III and -9.5 ± 20.4 for Draf-IIa, p = .74) (Figs. 1 and 2). When evaluating domain/subscores, the patients who underwent Draf-III demonstrated worsening of extranasal symptoms, whereas the patients who underwent Draf-IIa versus Draf-III demonstrated a mean ± SD improvement (2.5 ± 2.3 versus 1.5 ± 4.7; p = 0.03) at the first postoperative visit. However, the patients who underwent Draf-III demonstrated less improvement versus Draf-IIa in mean ear/facial symptom score at the second (−0.5 ± 2.6 versus -3.9 ± 4.7; p = 0.02) and third postoperative visits compared with Draf-IIa and -1.1 ± 1.6 versus -3.5 ± 3.3; p = 0.01).
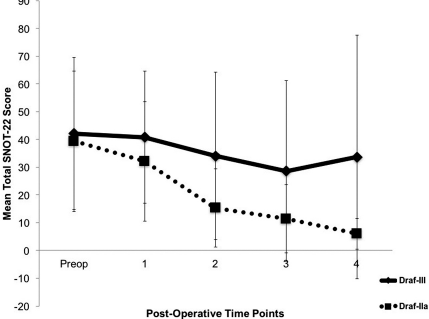
Longitudinal Mean Total SNOT-22 Score for Draf-IIA and Draf-III Patients. Values indicate the mean total SNOT-22 score for each treatment group (Draf-IIA and Draf-III) at preoperative assessment and each of the follow-up time points. Error bars indicate one standard deviation from the mean. Time point 1 includes days 0-12, time point 2 includes days 13-24, time point 3 includes days 25-36, and time point 4 includes days 37-48. Independent samples t-test was done to detect differences between the mean values between treatment groups (Draf-IIA vs Draf-III) showed no significant between group differences in mean values at level P <.05. Abbreviations: SNOT-22, Sinoasal Outcomes Test.
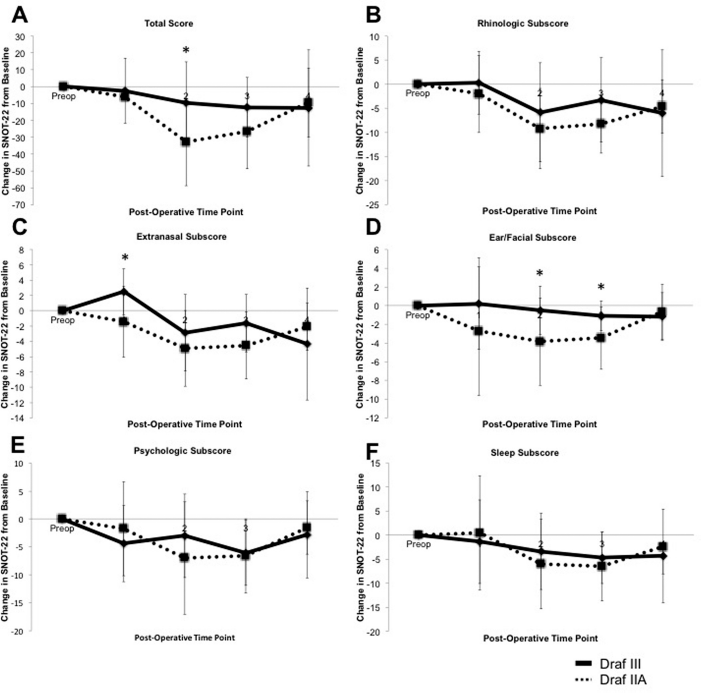
Longitudinal Mean Change in SNOT-22 Total and Sub-scores from Baseline Preoperative Assessment Values indicate the mean difference between follow-up time point and baseline preoperative assessment, such that negative values indicate an improved SNOT-22 score. Error bars indicate one standard deviation from the mean. Time point 1 includes days 0-12, time point 2 includes days 13-24, time point 3 includes days 25-36, and time point 4 includes days 37-48. Independent samples t-test was done to detect differences between the mean values between treatment groups (Draf-IIa vs Draf-III). A = total score, B = rhinologic sub-score, C = extranasal sub-score, D = ear/facial sub-score, E = psychologic sub-score, F = sleep sub-score. *Indicates significantly different mean values at level P < .05. Abbreviations: SNOT-22, Sino-nasal Outcome Test.
Discussion
Although the Draf-III surgery has improved treatment of recalcitrant frontal sinus disease with favorable safety and long-term results, surgeons generally consider the associated postoperative sinonasal morbidity as more significant than less-extensive interventions. 5 The extent of frontal sinus surgery has been anecdotally considered as inversely related to postoperative morbidity, and, as such, remains controversial. Here, we described the short-term (<8 weeks) sinonasal morbidity in patients who underwent Draf-III and compared this group with an age and radiographically (Lund-Mackay) matched group of patients who underwent a less-extensive frontal sinus intervention (Draf-IIa). The results demonstrated that patients who underwent Draf-III required more antibiotics and more debridements, and experienced a greater burden of symptoms within the SNOT-22 domain that captured facial pain/pressure within the first 2 postoperative months.
We anticipated that the increased tissue trauma and secondary intention healing associated with the use of a drill would result in a more arduous recovery. Wide bony dissection, inherent to extended frontal sinus surgery, contributes to prolonged crust formation and edema, as described in the phases of mucosal healing. 12 We found that the impact of this protracted course had significant clinical implications for the patient. In our cohort, patients who underwent Draf-III required more mean postoperative visits (4.9 ± 1.7 versus 3.3 ± 0.8; p < 0.005), in-office debridements (4.2 ± 2.0 versus 2.3 ± 0.8; p < 0.005), and days of antibiotic therapy (24.4 ± 11.8 days versus 15.6 ± 6.4 days; p < 0.005) versus Draf II-a within a similar follow-up time period (5.3 ± 2.0 weeks versus 4.9 ± 2.0 weeks; p = 0.53). Given these results, patients who underwent Draf-III should be appropriately counseled regarding the potentially increased intensity of postoperative management and propensity for postoperative infection to establish expectations and help guide treatment selection.
Moreover, we found that the implications of Draf-III on quality of life were substantial. Although both the Draf-III and Draf-IIa groups achieved a minimally clinically significant difference over the study period, defined by a mean improvement in SNOT-22 score of >9 (−12.7 ± 34.5 and -9.5 ± 20.4, respectively; p = 0.74), further analysis demonstrated temporal variability in quality-of-life domains as well. 13 Specifically, at the first postoperative visit (∼1 week after surgery), the patients who underwent Draf-III experienced worsening of extranasal symptoms compared with Draf-IIa (2.5 ± 3.0 versus -1.5 ± 4.7; p < 0.05), defined as cough and postnasal and thick nasal discharge. This time period corresponded to the blood clot and/or crusting and edematous phase of mucosal healing.12,14 Postoperative dysfunctional ciliary motility and stasis of secretions may compound these symptoms. 15
Analysis of the present data also demonstrated delayed recovery in ear/facial symptoms (sneezing, ear fullness, dizziness, ear pain, and facial pain/pressure) in Draf-III compared with Draf-IIa at the second-and third- postoperative visits, which corresponded to ∼2 and 4 weeks after surgery, respectively. The delayed recovery of ear/facial symptoms in patients who underwent Draf-III was likely a reflection of the prolonged facial pain/pressure associated with secondary intention healing within a drilled-out neo-ostium. Interestingly, this difference equilibrated between the groups by the last postoperative visit (∼5 weeks after surgery). However, because the patients who underwent Draf-IIa and were doing well at their third postoperative visit were not asked to follow up in the clinic until 3 months after surgery, the patients who presented at this fourth visit were more likely to have experienced delayed recovery, thereby introducing a selection bias.
Overall, we demonstrated significant clinical and quality-of-life morbidity associated with the Draf-III cohort above and beyond that which was associated with Draf-IIa (bilateral) frontal sinus surgery. This increased burden of recovery associated with the Draf-III was expected, given the extent and degree of secondary intention healing and sinus dysfunction related to the drilled-out neo-ostium and exposed bone. These findings are valuable because they were the first to directly compare and characterize the burdens of recovery between these two frontal sinusotomies in age and radiographically matched patients. Patients who undergo Draf-III should be counseled to expect a more painful and involved recovery compared with a Draf-IIa frontal sinusotomy. In addition, surgeons should anticipate a more-intensive recovery in terms of follow-up, debridement, and medical therapy.
The present data were not without limitations and the findings only begin to provide insight into the precise role of Draf-III and Draf-IIa frontal sinusotomies in clinical practice. The nonrandomized and retrospective design of this study exposed it to potential selection bias and confounding. With regard to selection bias, a randomized study design is theoretically feasible, but enrollment would be difficult because patients may be randomized to a more challenging recovery and a stepwise escalation of Draf-III for Draf-IIa failure demonstrated efficacy in previous studies. Furthermore, Draf-IIb has been demonstrated to be a safe and effective alternative to Draf-III in appropriately selected patients, which complicated the rationale behind randomization. 16
In addition, although there was no statistical difference in preoperative total SNOT-22 between the groups, there were more patients with AERD in the Draf-III group and, as such, the postoperative characteristics may have been influenced by the disease rather than by the intervention. Similarly, more patients in the Draf-III group had previously undergone surgery and, therefore, may have been inherently less likely to demonstrate improvement on quality of life compared with patients who underwent Draf-IIa that was mostly primary surgery. 17 Also, this study had a relatively small sample size, and the procedures were performed at a single institution with a single surgeon. Moving forward, a multi-institutional and multisurgeon investigation into these differences is warranted, but, until that time, the present study reflected the best available evidence on the topic.
Conclusion
To our knowledge, this was the first study to compare the short-term clinical management and patient-reported outcome measures of Draf-III and Draf-IIa (bilateral) frontal sinus surgery. Analysis of the results demonstrated increased frequency of follow-up and interventions (debridements and antibiotics) as well as a more-prolonged patient-reported recovery associated with Draf-III compared with Draf-IIa. Although Draf-III is a safe and effective frontal sinus procedure, counseling patients who may require this intervention should include a detailed discussion of the burden of postoperative care and recovery, particularly as it becomes more accepted as a primary intervention.