
Abstract
Medicinal plants have been overtaken in the treatment of snake bites by serum therapy and are rarely considered efficacious remedies in biomedicine. Nevertheless, rural inhabitants rely on plant medical material and the attention of highly regarded local traditional healers when threatened by snakebite poisoning. This paper examines curative and preventive snakebite treatments, beliefs and practices collected from 100 Luo respondents. The informants reported the use of a number of herbal and non-herbal remedies including mystical therapies and 24 herbaceous plants whose aerial parts are preferred. Treatments involve cut, suck, and bind methods followed by application of plant leaf and root poultices held in place with strips of cloth or bark.
Introduction
People fear snakes of the families Elapidae (cobras and mambas) and Viperidae (vipers and adders) because of their highly irritable nature, elaborate poison apparatus, and toxic venom, which causes respiratory difficulties, persistent bleeding, and even death. Snakebites inflict great suffering on victims. Globally, the number of accidents involving snakes reaches one million, resulting in 600,000 envenomations and more than 20,000 deaths annually (Chippaux 1998).
With two groups of venom-spitting cobras and a great diversity of vipers, Africa is a global diversity center and focal point of cobra distribution and the Old World vipers (Ditmars 1946; Fitz Simmons 1970). The Republic of Kenya has a fair share of these snakes—97 species—of which four are endemic, distributed in almost every part of the country. Most areas of the Nyanza province of Kenya provide niches conducive to reptile life. A sinister reputation surrounds seven local venomous snake species: Naja nigricollis (
Up to 80% of snakebite victims in Kenya first consult traditional practitioners before visiting a medical center (Snow et al. 1994). Direct testimony from victims attests to the perceived powers of traditional treatments. The success of traditional healers is vaguely understood to be partly due to the occult and sometimes mystical nature of their practice. In an attempt to examine their practices, which remain incompletely known, this paper pays attention to herbal and some nonherbal therapies used by traditional healers in managing snakebites among humans and livestock in the study area.
The Study Area
The study was carried out in Nyanza Province in Western Kenya. The province lies astride the equator, lat. 0°35′ S, long. 34°45′ E, bounded to the west by Lake Victoria and to the south by the Republic of Tanzania. It falls within the Lake Victoria regional mosaic plant belt of Africa, dominated by a graded vegetal landscape of relict tropical rainforest, bush grassland (Themeda-Hyparrhenia) and wooded grassland vegetation of the Combreto-Dodoneae-Balanites-Acacia matrix.
The Luo people are an agropastoral-cum-labor-migrant group of the Western Nilotic cluster of societies (Cohen and Atieno-Odhiambo 1989); their language, Dholuo, has a Nilo-Saharan eastern Sudanic affiliation. Many authors note their extensive local knowledge of medicinal value of plants that grow in their environment (Johns et al. 1990; Kokwaro and Johns 1998; Owuor 1999). Accounts of Luo culture and life are given by Ogot (1967), Whisson (1964), Kawango (1995), and Ocholla-Ayayo (1976). Luo disease etiology and therapies are embedded in indigenous religious beliefs, Christianity, and their
Herbal Antivenom Research
The perceived efficacy of traditional herbal snakebite remedies and related therapies evokes much interest among researchers. Most of the indigenous remedies reported in literature are root-derived. Various plants named “snakeroot” with long twisted “snaking” roots are preferred. Taylor (1970) notes that in North America and Asia, this name applies to at least five different plants supposed to be snakebite remedies: Aristolochia reticulata (Texas snakeroot), Ophiorrhiza mungos (snakeroot), Liatris spicata (button snakeroot), Eryngium aquaticum (white snake-root), and Asarum canadense (Canadian snakeroot, wild ginger).
However, this study shows the prevalence of foliar plant parts (
The fundamental supposition in medicinal plant research is that natural products from plants can complement serum therapy or alleviate the side-effects of modern snakebite therapy. The idea is spreading rapidly and widely with research successes, such as the pronounced activity of aqueous extracts and 12-methoxy-4-methylvoachalotine from Tabernaemontana catharinensis against South American rattlesnake venom (Batina et al. 2000); coagulative (prothrombin) activation of Mucuna pruriens seed extract (Guerranti et al. 2001); anti-inflammatory activity of Bidens pilosa flavonoids in laboratory animal studies (Geissberger and Sequin 1991; Jager et al. 1996); significant inhibition of lethality, myotoxicity, and venom enzyme activities of Naja kaouthia venom by aqueous Mimosa pudica root extracts (Mahanta and Mukherjee 2001); in vitro and in vivo antagonism of venom-induced haemorrhage, coagulant, defibrinogenating, and inflammatory activity of Vipera russellii and N. kaouthia venom by root extracts of Vitex negundo and Emblica officinalis (Alam and Gomes 2003); detoxification (in vitro) of Echis carinatus and Naja nigricollis venom by Guiera senegalensis leaf extract (Abubakar et al. 2000); isolation of Russell's viper venom-specific anti-inflammatory, antipyretic, and anti-oxidant active compounds from Hemidesmus indicus (Alam and Gomes 1998aAlam and Gomes 1998b); neutralization of Bothrops jararaca and Crotalus durissus terrificus venom toxicity by arturmerone fraction of Curcuma longa extracts (Ferreira et al. 1992); uncharacterized anti-inflammatory and analgesic compounds of Strychnos henningsii (Tits et al. 1991). Venom of the West African serpent Echis carinatus has been the subject of interesting investigation—ehretianone, a quinonoid xanthene, isolated by Selvanayagam et al. (1996) from Ehretia buxifolia root bark, displayed activity. Onuaguluchi (1989) further demonstrates Diodia scandens activity against E. carinatus venom.
It is important to note that these plants represent a fraction of the world's herbal envenomation pharmacopoeia and against this background the case for medicinal plant research is strengthened. Vasanthi and colleagues (2003) demonstrate that opportunities are not limited to terrestrial plants; brown seaweed Padina boergesenii and red seaweed Hypnea valentiae extracts were found to detoxify (in vitro) N. nigricollis venom. Remarkable mortality reduction was noted in rodents administered with extract-reconstituted venom injections compared to those challenged with venom only.
Methodology
One hundred respondents consisting of lay persons and specialist traditional practitioners were interviewed over an eight-month period. Questionnaires with both close and open-ended questions as in Martin (1995) were used to collect survey data. Specialist traditional healers interviewed ranged from 32–63 years of age. They owe their healing skills to training by knowledgeable kin, spirit inspiration, or
Results
The Luo have various beliefs about snakes. Though snakes are particularly linked with witchcraft, big snakes are associated with the underworld of dead people and are considered their messengers. The appearance of such snakes in settled areas prompts community speculation and magico-religious expectations. People still believe in
Snake attacks are reportedly sure, quick, sometimes unnoticed, and result in scratches and fang entry wounds. All interviewees described observations matching clinical ophitoxaemia—the wide spectrum of local and systemic manifestations that result from snake venom poisoning. Informants reported that the effects of snakebites including swelling or skin discoloration, shock, weakness, convulsions, shortness of breath, nausea, severe pain, paralysis, unconsciousness, and even death. The local people seek help through traditional herbal medicines.
Luo Herbal Snakebite Medicines
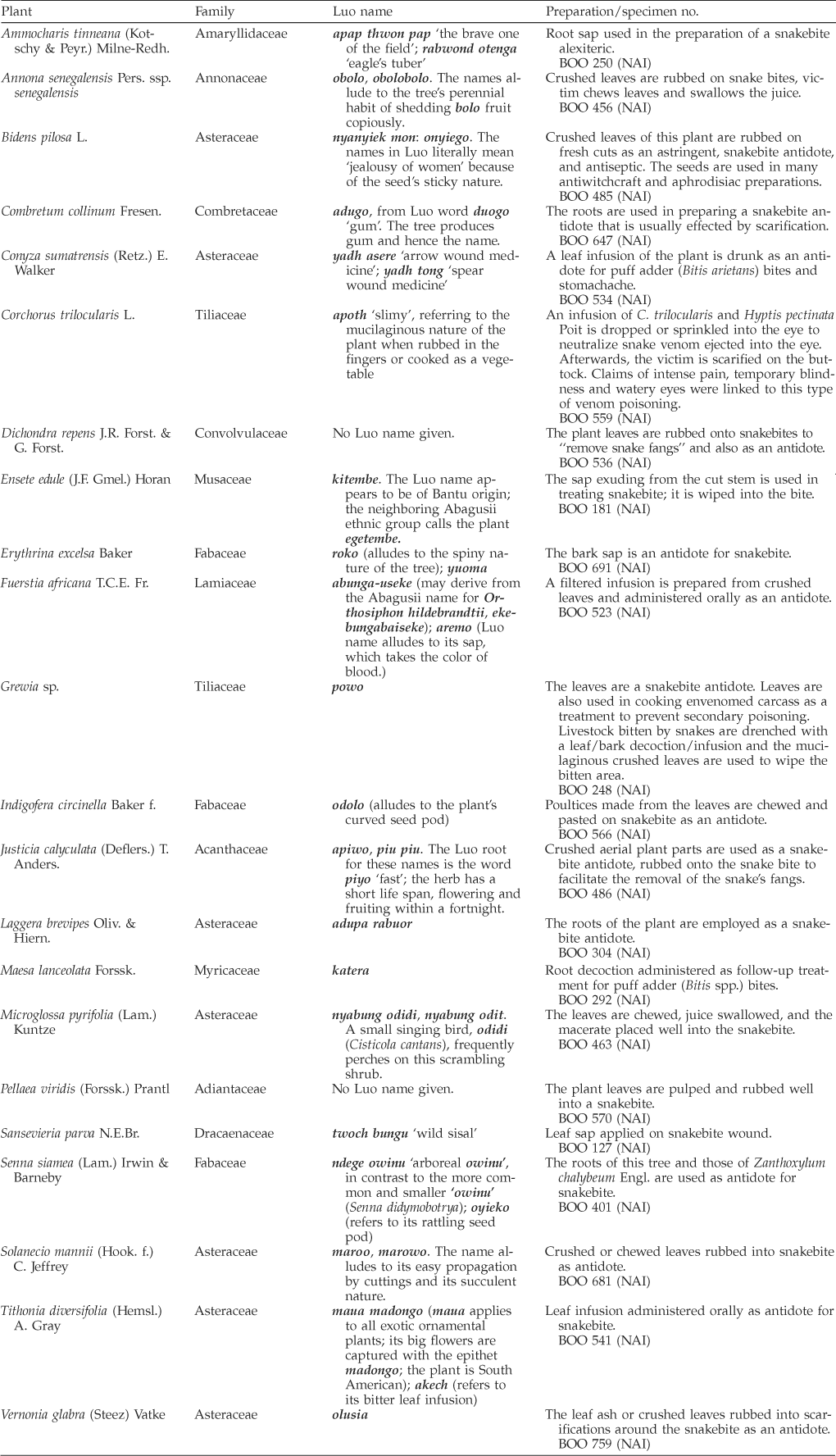
Twenty-four plants employed as snakebite medicine by the Luo people, including two exotic species (Senna siamea and Tithonia diversifolia), were collected and are listed alphabetically along with their local names and voucher specimen numbers in Table 1. Local plant names recorded in this study show slight variations from those presented by Kokwaro and Johns (1998) in the Luo Biological Dictionary. The plant names fit assumed ethnosystematic categories in Martin (1995); with primary (unitary), secondary (binomial), and complex (polynomial) names recorded. Stace (1996) posits that the dearth of local plant names is due to the value-based emphasis of folk taxonomies—a possible explanation why the fern, Pellaea viridis, with marginal importance as food, medicine, or animal forage lacked a local name response.
Plants used as snakebite medicine by Luo.
Indigenous Luo Snakebite Therapies
In this study it was found out that envenomation hazards are linked with traditional foraging and cultivation activities, similar to the findings of Chippaux (2000). Virtually all households engage in outdoor activities, especially subsistence agriculture. Nonetheless, as reported by 26 informants, the vulnerable members of the population are farmers, firewood collectors, hunters, and herders between the ages of 12 and 50 years. We could not ascertain snakebite frequency because of insufficient records, but the general view in the study area was that frequency of snakebite incidents is medium to high.
Traditional treatment for snakebites begins in the field immediately after the victim is bitten. Fresh medicinal plant preparations are prepared and administered within a half hour. Bands are tied above and below the bitten area to slow the spread of venom. Incisions are then made across the main wound area using a razor blade or a lancing pin. The bitten area is then sucked with the mouth until blood flows freely. This practice is believed to drain the poisoned blood. Thereafter, some healers cauterize the wound with heated broken clay pot pieces or put potassium permanganate crystals on it before placing or rubbing plant materia medica into the bite. The medicine is held in place with strips of cloth or bark. The poultice can be replaced frequently. In other treatments, infusions or decoctions are administered orally after attention to the bite. Eighty-three percent of the oral administrations reported in the study were infusions. All respondents claimed no side effects or overdose due to traditional medication. This claim has implications for the most difficult problems of allergy and organ function loss encountered in modern serum treatments and the “cut and suck” snakebite therapy. Similar treatment procedures appear in medicinal plant compendia from other parts of eastern and southern Africa (Kokwaro 1976; Watt and Breyerwandijk 1962) as well as in West Africa (Ayensu 1978; Burkill 1985; Oliver-Bever 1986).
Generally, plant material procured from dry environments was considered more efficacious due to habitat hardiness. Healers credit the pharmacological action of Conyza sumatrensis and Bidens pilosa to haemostatic and antiseptic action. B. pilosa has been shown to have anti-inflammatory activity (Geissberger and Sequin 1991; Jager et al. 1996). Painkillers, largely administered orally, increase urination and sweating, resulting in poison release. Pure substances from plants shown to protect mice from ophitoxaemia are generally nitrogen-free, low molecular-weight compounds: phenolics, phytosterols (bamyrin and sitosterol) and triterpenoids (Alam and Gomes 1998a, Alam and Gomes 1998b; Haruna and Choudhury 1995; Perreira et al. 1994; Selvanayagam et al. 1996). However, Batina et al. (2000) report an odd case of a nitrogen-containing substance, the alkaloid 12-methoxy-4-methylvoachalotine. These substances possess venom-inactivating, analgesic and anti-inflammatory action (Ferreira et al. 1992; Vilegas et al. 1997).
In addition, the Luo people believe in instantaneous mystical snakebite healing. Such healing is performed by touching the
Since the latter half of the twentieth century, some Luo, as a result of missionary efforts, adopted the Christian faith. Nonetheless, they maintained submission to their god, Nyasaye, and reverence to spirits of the departed. Soon enough, suspicion and lack of dialogue between Luo and Christian belief led to breakaway African Independent Churches in the 1930s (Barrett 1982). Adherents of these churches practice Christian healing rites. Healing by touching performed by
Preventive snakebite treatments were also reported; one such treatment involves scarifications with
Lack of commercial antiserum and high cost of biomedical services, together with the cultural acceptability of local therapies, further motivate the resort to traditional treatments. The situational approach of William I. Thomas and Florian Znaniecki explains and illustrates the conditions of rural people and persistence of traditional medicine in most developing countries (Bogardus 1963). Human behavior is viewed as situationally defined—when the patient is confronted with a snakebite in an unprepared state the phenomenon assumes the aspect of a crisis. In South Nyanza, where this study was conducted, there are inadequate health facilities (Sindiga 1995). Consequently, in deciding between traditional and modern methods, patients generally choose the closest source of relief.
Discussion
Although herbal remedies are espoused as inexpensive alternatives or complementary to antivenom serum and potential sources of new treatments, their status remains weak due to insufficient evidence of their safety and efficacy. Yet serum therapy may have serious side effects: fever, rash; severe and sometimes fatal allergic reactions due to production contaminants (horse or chick proteins) (Russell 1989). Krifi et al. (1999) note the inadequacy of purification by enzyme digestion and other contaminant extraction procedures. Moreover, Consroe et al. (1995) report that even purified immunoglobulin antivenom evokes hypersensitivity. Therefore, by failing to seek new envenomation cures we may be in danger of ignoring potentially valuable remedies. It seems the search for pharmacological deliverance from snake venom is far from over. More substantive and careful investigation of traditional therapies is critical to determine their viability as alternatives.
Among the Luo, the choice of snakebite remedies and local perceptions of the efficacy of the medicines that are used consistently by healers reflect their physiological activity. Johns et al. (1990) conducted a study using consensus and validation techniques among Luo interviewees; they found that 5% (2 out of 37) of the snakebite remedies fit their consensus criterion—confirmation through independent reports from three or more individuals. In our independent, similar study of snakebite remedies, 9 out of 24 (38%) were independently reported by three or more individuals. As the two studies show, the use of a variety of species could well be a feature of the body of traditional snakebite remedies. The greater the consensus among herbalists and laypersons about the efficacy of particular plants in the treatment of snakebite, the more likely it is that these remedies will prove to have bioactive chemicals.
Conclusion
Traditional medicine continues to be used by the Luo people in rural western Kenya against snakebites. We note that poor hospital infrastructure, lack of antiserum, high medical fees, and a deep-seated confidence in local healers based on cultural conceptions and values are responsible for continued medicinal plant use among the Luo people. The success of local practitioners lies in their knowledge of the consequences of a snakebite, the patient's confidence in their treatment, and their grasp of the snakebite situation, all of which give the victim hope and help recovery from fright in such a dire time. The chemical and pharmacological properties of their therapies remain uninvestigated. The lack of interest in traditional snakebite therapy by biomedical practitioners lies partly in the complexity of the art of mystical healing.
Footnotes
Acknowledgments
Special thanks and cordial acknowledgement go the healers interviewed in the districts of Suba, Migori, and Homa Bay; this information is their property. We would also like to express our thanks to the field research team of volunteers, field assistants, and local administrative officers in the study sites for their support. The University of Nairobi and the Earthwatch Institute provided financial support for the fieldwork.