
Abstract
“Attention to health is life's greatest hindrance”
Plato (427BC–347BC)
METABOLIC SYNDROME
‘Metabolic syndrome’ refers to a cluster of risk factors (abdominal obesity, dyslipidaemia, hyperglycaemia and hypertension) that, when grouped together, are associated with an increased risk of cardiovascular disease and type 2 diabetes. 1 The presence of metabolic syndrome is associated with a two to threefold increase in cardiovascular disease mortality, fivefold increased risk to develop type 2 diabetes, and twofold increase in overall mortality. 2–4
Metabolic syndrome is highly prevalent among chronic psychiatric disorders, particularly schizophrenia (Table 1). Within Australia, rates for metabolic syndrome in psychiatric populations (range 54–68%) 5,6 are up to twice that of the general population (range 29–34%). 7–9 There is also a trend of increasing premature mortality due to cardiovascular illness in people with schizophrenia, 10–13 such that it is the largest single natural cause of death and a significant contributor to the associated reduction in life expectancy. 13
Prevalence rates of metabolic syndrome in psychiatric populations
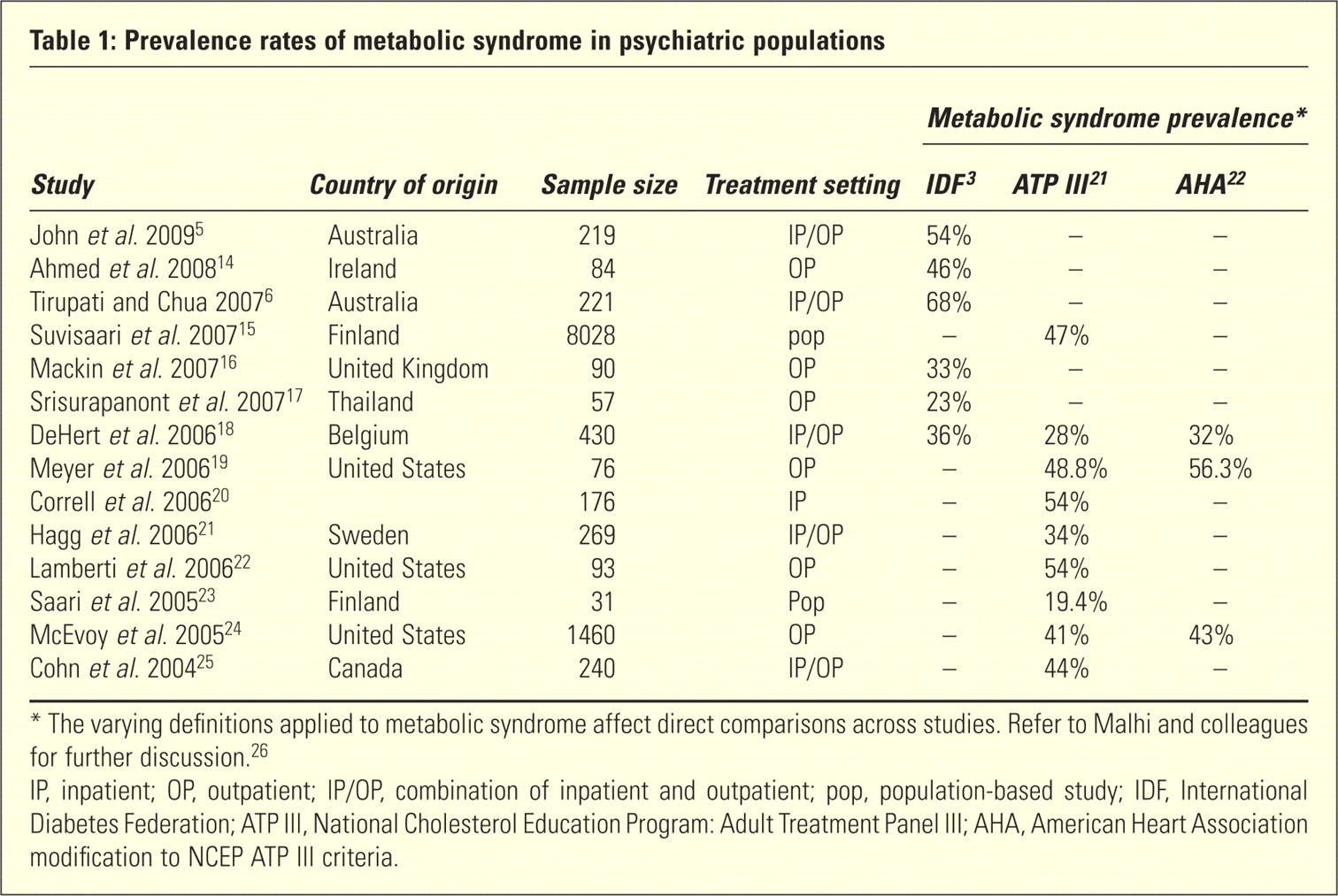
∗ The varying definitions applied to metabolic syndrome affect direct comparisons across studies. Refer to Malhi and colleagues for further discussion. 26
IP, inpatient; OP, outpatient; IP/OP, combination of inpatient and outpatient; pop, population-based study; IDF, International Diabetes Federation; ATP III, National Cholesterol Education Program: Adult Treatment Panel lII; AHA, American Heart Association modification to NCEP ATP III criteria.
The largest study to date on the prevalence of metabolic syndrome in patients with schizophrenia was conducted in the United States as part of the Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE), 24 a multisite prospective study involving 1460 patients with schizophrenia. The trial assessed the effectiveness of antipsychotic medications in targeting symptomatic, metabolic, neurocognitive and functional outcomes and found that the outpatient prevalence of metabolic syndrome was 43%. Across both genders and in almost all age groups (except age 50–59 years), prevalence rates were higher in the schizophrenia population compared to the general population and it was noted that females were particularly vulnerable to central obesity and metabolic syndrome. Furthermore, as observed in the wider population, increasing age was associated with a greater likelihood of metabolic syndrome.
PHYSICAL HEALTH PROBLEMS IN SCHIZOPHRENIA
The reasons for the increased prevalence of physical health problems in schizophrenia are not fully understood, but are likely to stem from a combination of biological and genetic vulnerabilities along with lifestyle factors and the side effects of prescribed psychotropic medications, in particular, those medications that may result in marked weight gain. 27,28
Considering each of these putative factors in turn, studies comparing neuroleptic-naïve patients with first-episode schizophrenia to matched controls have identified metabolic differences in patients with schizophrenia, including reduced insulin sensitivity, 29 increased prevalence of impaired glucose tolerance 30 and hepatic insulin resistance. 31 Schizophrenia is associated with poorer lifestyle habits, including poorer quality diet, reduced exercise and increased rates of smoking. 32 Smoking increases the risk of complications such as respiratory and cardiovascular disorders 27 and in schizophrenia is associated with worse clinical outcomes including longer duration of illness and greater antipsychotic use. 33 This may be due to the rate of cigarette smoking in people with schizophrenia being up to four times higher than that of the general population (prevalence estimates of 62% in psychiatric samples compared to 16% in the general population) 34 and a tendency for heavy smoking that generates high levels of nicotine in the bloodstream. 35 Consequently, it has been suggested that both lifestyle interventions and smoking cessation should be routinely included as part of a broader approach to mental health intervention. 33,36
These largely intrinsic factors in schizophrenia that contribute to poor physical health are added to, and exacerbated by, iatrogenic factors, in particular antipsychotic medications. 37,38 In this regard, there is strong evidence that some of the atypical antipsychotics pose a greater risk for cardiometabolic adverse effects and are perhaps more damaging than conventional antipsychotics. 39,40
CLOZAPINE
Among the atypicals, clozapine is perhaps the most effective treatment for schizophrenia. It is usually prescribed second- or third-line because its blood levels need to be monitored. However, along with olanzapine, it is also the most likely atypical to produce significant weight gain 41 and therefore, not surprisingly, its use is associated with high rates of metabolic syndrome. 21,22,42
Clinically, clozapine's range of receptor interactions underpins its unique therapeutic profile and its production of hyperlipidaemia contributes to metabolic syndrome. Interestingly, the effects of duration of clozapine treatment on metabolic syndrome are not known and findings from research studies remain unclear. In one study, the risk for metabolic syndrome was not found to be related to the length of treatment, 14 but increasing risks have been reported in other trials. 22,43,44 In other research, the 10-year mortality rate from cardiovascular disease in patients taking clozapine was estimated at 9%, with the increase in risk factors escalating over time. 43
AIM AND HYPOTHESES
This study was conducted to examine data obtained within a naturalistic clinical setting, namely a cohort of non-acute inpatients at a psychiatric hospital, to identify the prevalence of metabolic syndrome and its putative precursors. In particular, clozapine – a common treatment in this schizophrenia population – was of interest to the investigators. It was hypothesized that clozapine use would be a significant predictor of poor metabolic health and that other clinical factors would also play a determining role.
METHOD
Subjects
In 2008, as part of routine clinical monitoring for all inpatients of Macquarie Hospital (a psychiatric rehabilitation hospital in Sydney, NSW), an annual cardiometabolic survey was conducted. The survey involved all 168 non-acute inpatients of the hospital. Data from one patient was excluded as he did not have an Axis I psychiatric diagnosis. All remaining patients had a primary psychiatric illness, with more than 95% of patients diagnosed as having DSM-IV schizophrenia or schizoaffective disorder.
Informed consent was not required as all data were obtained as part of routine clinical monitoring for the hospital. Approval was obtained from Northern Sydney Central Coast Human Research Ethics Committee to undertake the analysis and publish relevant findings.
Data collection
On a nominated day, all inpatients were weighed, waist circumference measured, height recorded and blood pressure measured by a psychiatric nurse. In addition, the most recent blood results over the previous 12 months were retrieved via the hospital's Medical Director program. The hospital pharmacy provided information on atypical antipsychotic use and medications used to treat cardiometabolic conditions (hypertension, hyperglycaemia, dyslipidaemia). Information regarding use of typical antipsychotics, lithium and valproate was also collected by the nursing staff, as was the smoking status of patients and the estimated number of cigarettes smoked daily. The information obtained at the annual screen is summarized in Table 2.
Summary of information collected at annual screeninga
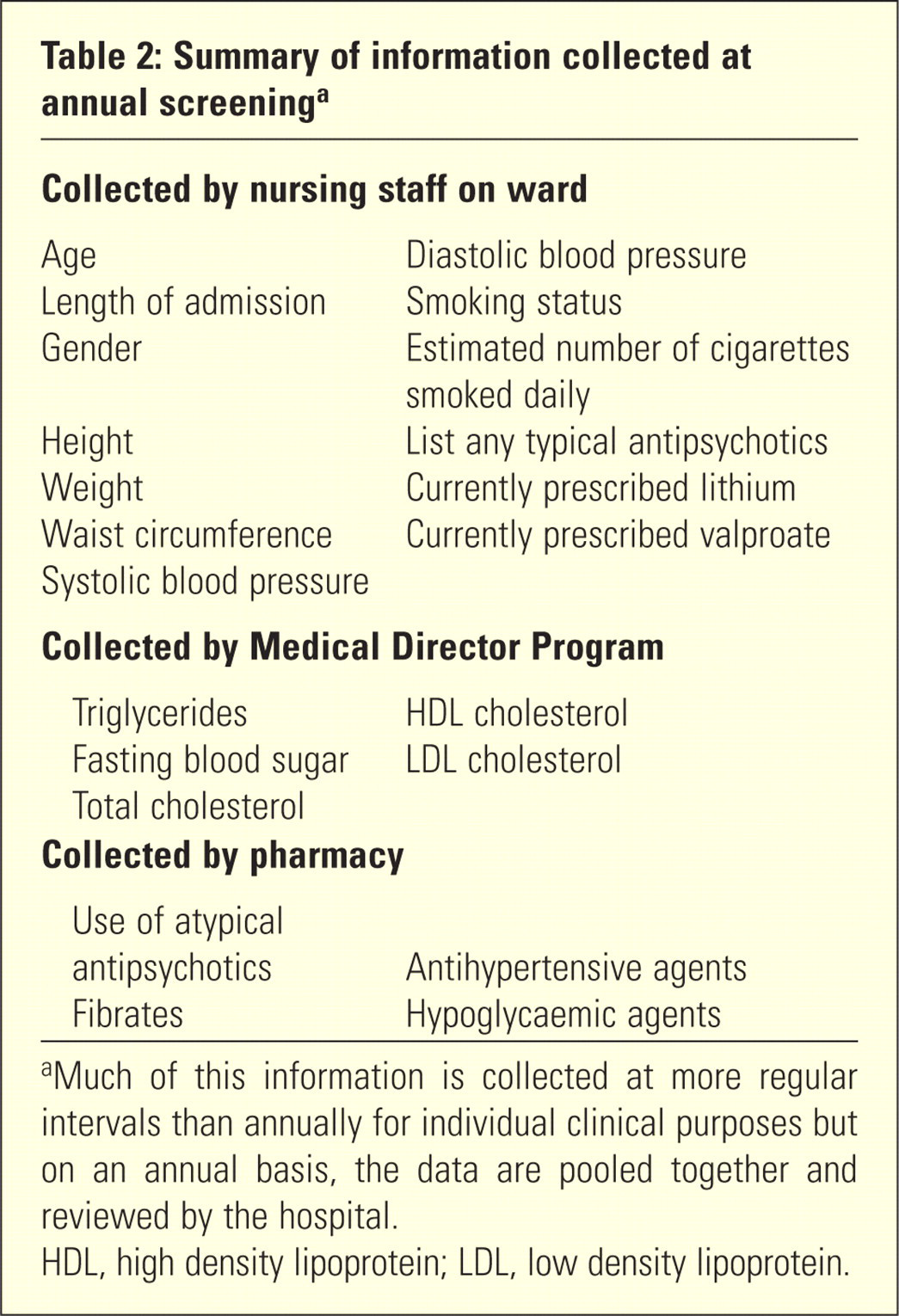
aMuch of this information is collected at more regular intervals than annually for individual clinical purposes but on an annual basis, the data are pooled together and reviewed by the hospital.
HDL, high density lipoprotein; LDL, low density lipoprotein.
Body mass index (BMI) was assessed and classified according to National Health and Medical Research Council guidelines. 45 Metabolic syndrome and its defining variables were diagnosed according to the criteria defined by the International Diabetes Federation (IDF). 1 In addition to applying cut-off levels for impairment, patients taking antihypertensive medication were considered to meet the blood pressure criterion as were patients taking antidiabetic medications (insulin and/or hypoglycaemic medication) and/or those with a diagnosis of type 2 diabetes considered to have met the blood glucose criterion. Similarly, patients taking fibrates were considered to meet the triglycerides criterion. In this context, the use of statins was also carefully considered due to their effect on lowering triglycerides and to a lesser extent raising high-density lipoprotein (HDL) cholesterol. However, statins are not typically prescribed for this purpose and therefore, to avoid the risk of false positive identification of metabolic syndrome, the use of statins was not attributed to either the impaired triglyceride or impaired HDL cholesterol categories. It is important to note that there are inconsistencies in the literature as to how medications are attributed to each of the risk categories, or indeed whether to include them at all. This, along with the existence of varying diagnostic criteria for metabolic syndrome, limits the ability to make direct comparisons across studies. 26 The approach adopted in this study was a pragmatic consensus view that reflects the majority approach when applying the IDF definition.
The data set used in this project was obtained from routine clinical care and therefore in some instances the data were incomplete. Of the 17 risk factors, including individual cardiometabolic risk factors and defining criteria for metabolic syndrome, the average compliance rate was 95.4% (range 79.2–98.8%). Subsequent descriptive data and statistics are based on the available data for each variable.
Biological measures were not acquired at a designated time and reflect the patient's most recent test results in the previous 12 months. As confirmed by clinical staff, 95% of blood glucose levels were fasting. Atypical antipsychotic use, including clozapine, and the duration of treatment was confirmed through pharmacy records. The scales used to weigh patients varied across wards but to gauge an acceptable level of agreement (Cron-bach alpha 0.693), two people were weighed and compared on all scales.
Data analysis
Forward entry binary logistic regressions were performed to examine which medications predicted metabolic syndrome, and the predictive power of five independent variables (age, gender, length of hospital admission, medication usage and smoking status) on metabolic syndrome. Forward sequential multiple regression analyses were performed to examine the relationship between the five independent variables (medication use, age, gender, smoking status and length of hospital admission) and cardiometabolic risk factors. These risk factors included BMI, waist circumference, triglyceride levels, blood glucose levels, systolic and dia-stolic blood pressure, total cholesterol, and both HDL and low-density lipoprotein (LDL) levels. In addition, chi-square analyses were performed to examine the relationship between the respective sets of independent and dependent categorical variables.
RESULTS
Demographic and clinical characteristics
Data from 167 patients were collated for this project, of whom 113 (67.7%) were males and 54 (32.3%) females. Patients were aged between 19 and 80 years, with an average age of 48.46 years (SD = 15.04). One hundred and five patients (63.6%) were smokers and 20 patients (12%) were diagnosed with diabetes.
Seventy-nine patients (47.3%), almost half of the sample population, were being administered clozapine. Of these, 63 were taking clozapine in conjunction with another antipsychotic and/or lithium or valproate (Figure 1). Twenty-six patients (15.6%) were taking olanzapine, 29 (17.7%) quetiapine, 36 (21.6%) risperi-done, 16 (9.6%) amisulpride and four (2.4%) were taking aripiprazole and ziprasidone respectively. Interestingly, 42 (25.1%) were taking haloperidol and 15 (9.0%) were taking chlorpromazine. Furthermore, 18 (10.8%) were taking lithium and 87 (52.1%) were taking valproate. Note, only those medications taken by more than 10 patients were included in subsequent analyses.
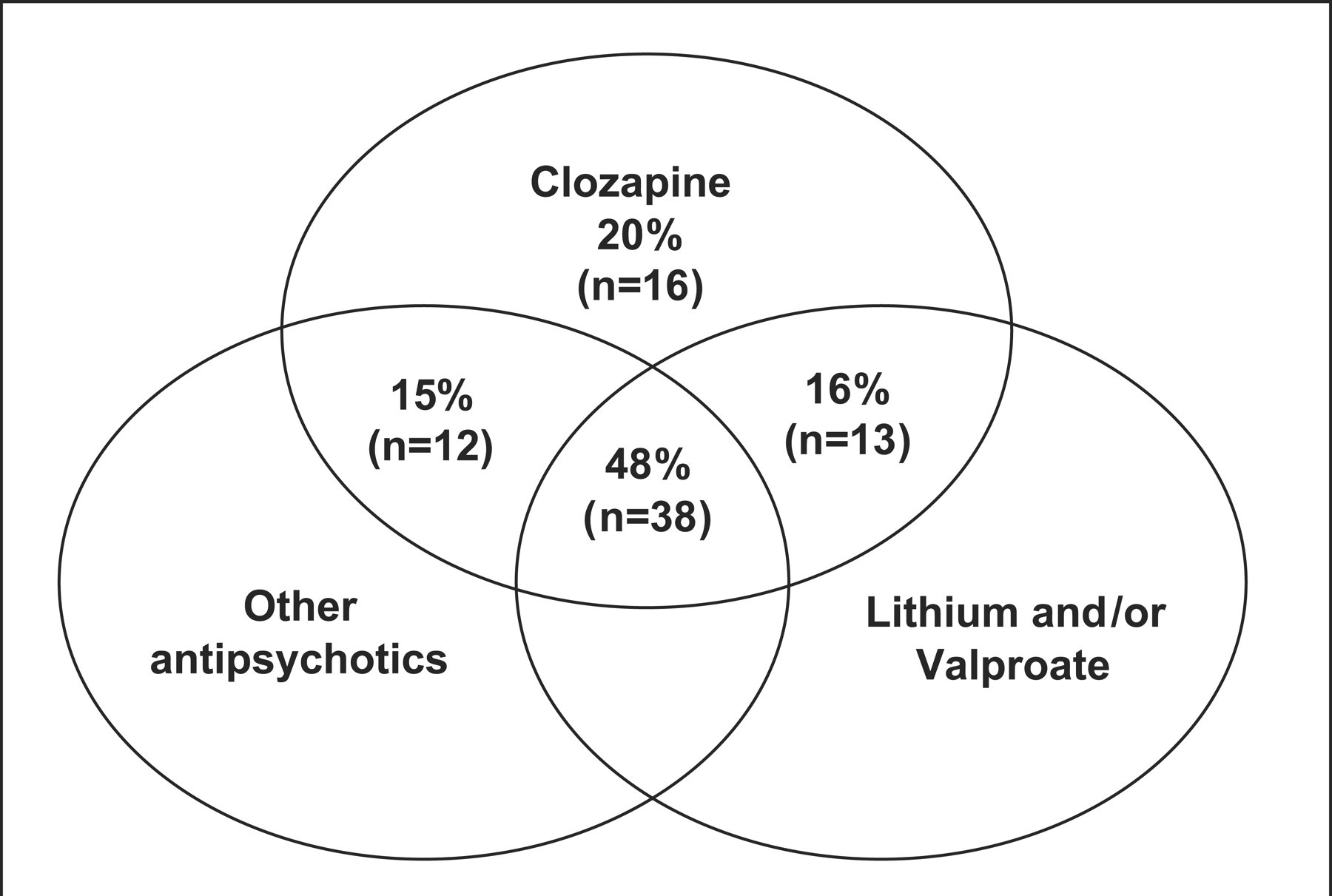
Pattern of clozapine administration: clozapine and use of multiple medications. Other antipsychotic = Patient was taking one or more of the following antipsychotics: olanzapine, risperidone, quetiapine, amisulpride, aripiprazole, ziprasidone, haloperidol, chlorpromazine, zuclopenthixol, fluphenazine, trifluoperazine.
Prevalence of metabolic syndrome and associated risk factors
Using the IDF criteria, the prevalence of metabolic syndrome in our population is 52.4%. However, if medications used to treat metabolic abnormalities are not included within the criteria, the prevalence decreases to 46.4%. Prevalence rates for individual cardiometabolic risk factors and for those meeting IDF metabolic syndrome criteria are provided for total samples and gender (Table 3), and for 10-year age groups (Table 4).
Prevalence of metabolic syndrome and cardiometabolic risk factors, total sample and by gender
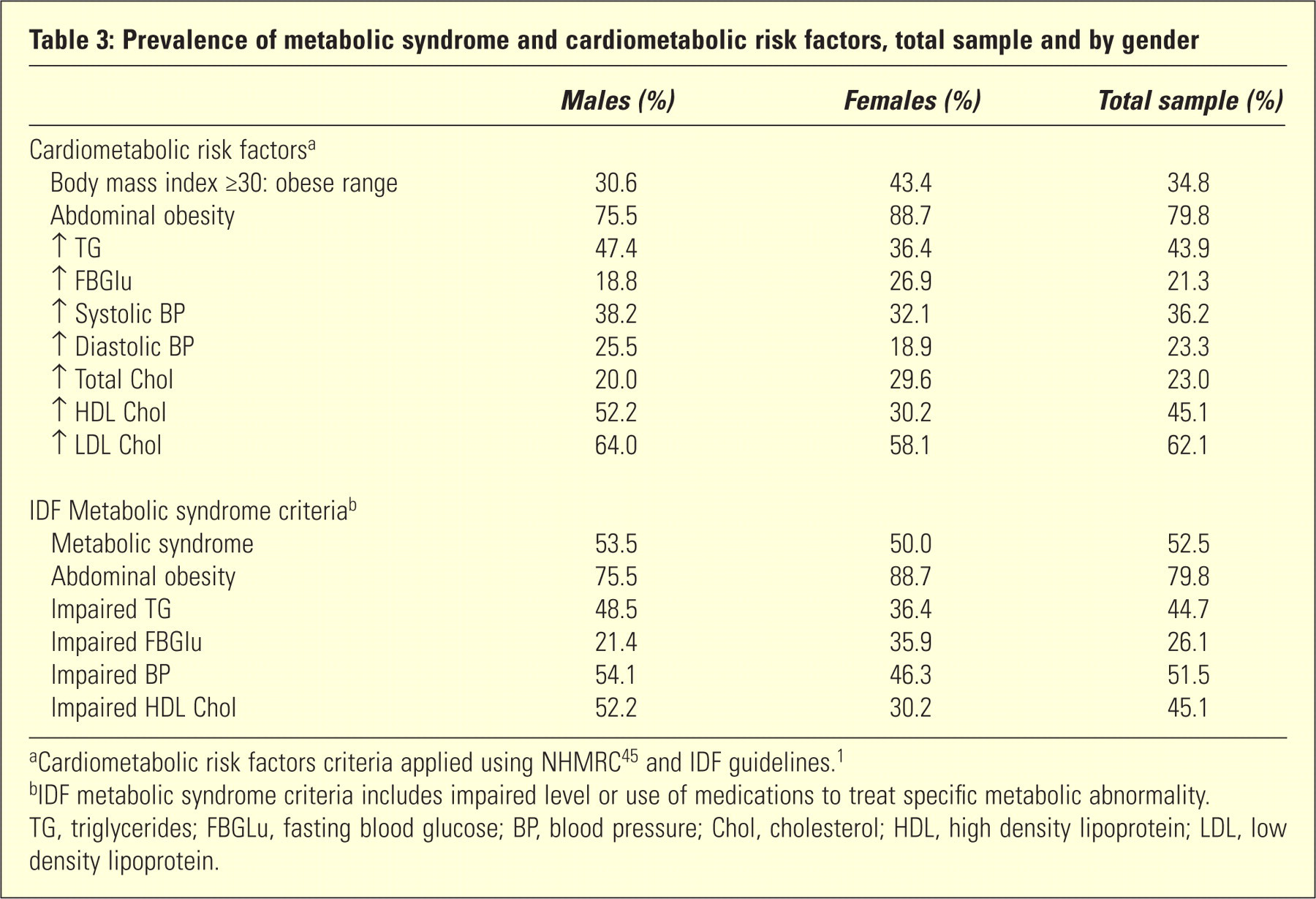
aCardiometabolic risk factors criteria applied using NHMRC 45 and IDF guidelines. 1
bIDF metabolic syndrome criteria includes impaired level or use of medications to treat specific metabolic abnormality.
TG, triglycerides; FBGLu, fasting blood glucose; BP, blood pressure; Chol, cholesterol; HDL, high density lipoprotein; LDL, low density lipoprotein.
Prevalence of metabolic syndrome and cardiometabolic risk factors by age group
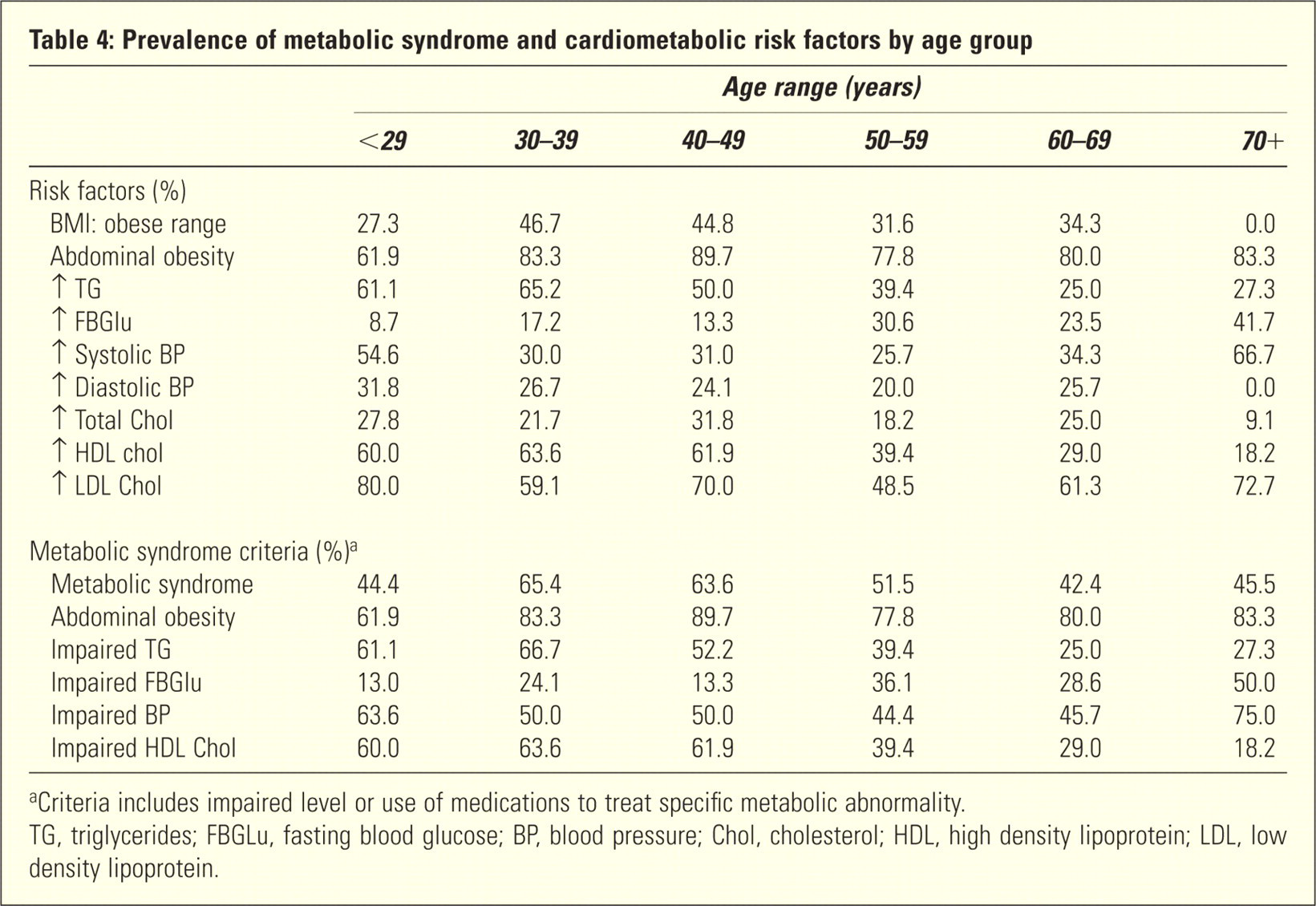
aCriteria includes impaired level or use of medications to treat specific metabolic abnormality.
TG, triglycerides; FBGLu, fasting blood glucose; BP, blood pressure; Chol, cholesterol; HDL, high density lipoprotein; LDL, low density lipoprotein.
Predictors of metabolic syndrome
Medication use
The results of binary logistic regressions showed that clozapine was the only medication to significantly predict metabolic syndrome (χ 2 = 3.89, df = 1, p = 0.049, Nagelkerke R 2 = 0.036, Exp(B) = 1.948, classification rate = 58.0%), whereby those taking clozapine were more likely to have met criteria (61%) than those not taking clozapine (46%).
The effect of clozapine taken in combination with other medications was then examined. Binary logistic regressions showed that clozapine taken in combination with at least one other antipsychotic, in combination with lithium and/or valproate, or when taken in combination with at least one other antipsychotic alongside lithium and/or valproate, did not add further predictive power to clozapine taken alone (p > 0.05).
Thus, clozapine was the only medication that significantly predicted metabolic syndrome, and hence subsequent analyses focused solely on this medication.
Length of admission, age, gender, clozapine use and smoking status
The results of binary logistic regressions are listed in Table 5. Of these, duration of admission was the strongest predictor of the metabolic syndrome, followed by clozapine use. Specifically, patients with a shorter duration of hospital stay were more likely to have metabolic syndrome as were those taking clozapine. After duration of admission and clozapine use were entered, smoking status, age and gender did not significantly predict metabolic syndrome (p >0.05).
Logistic regression analyses – predictors of the metabolic syndrome

Predictors of cardiometabolic risk factors
A summary of the multiple regressions are tabulated (Table 6) and illustrated schematically in Figure 2.
Multiple regression analyses – summary of significant predictors of cardiometabolic risk factors
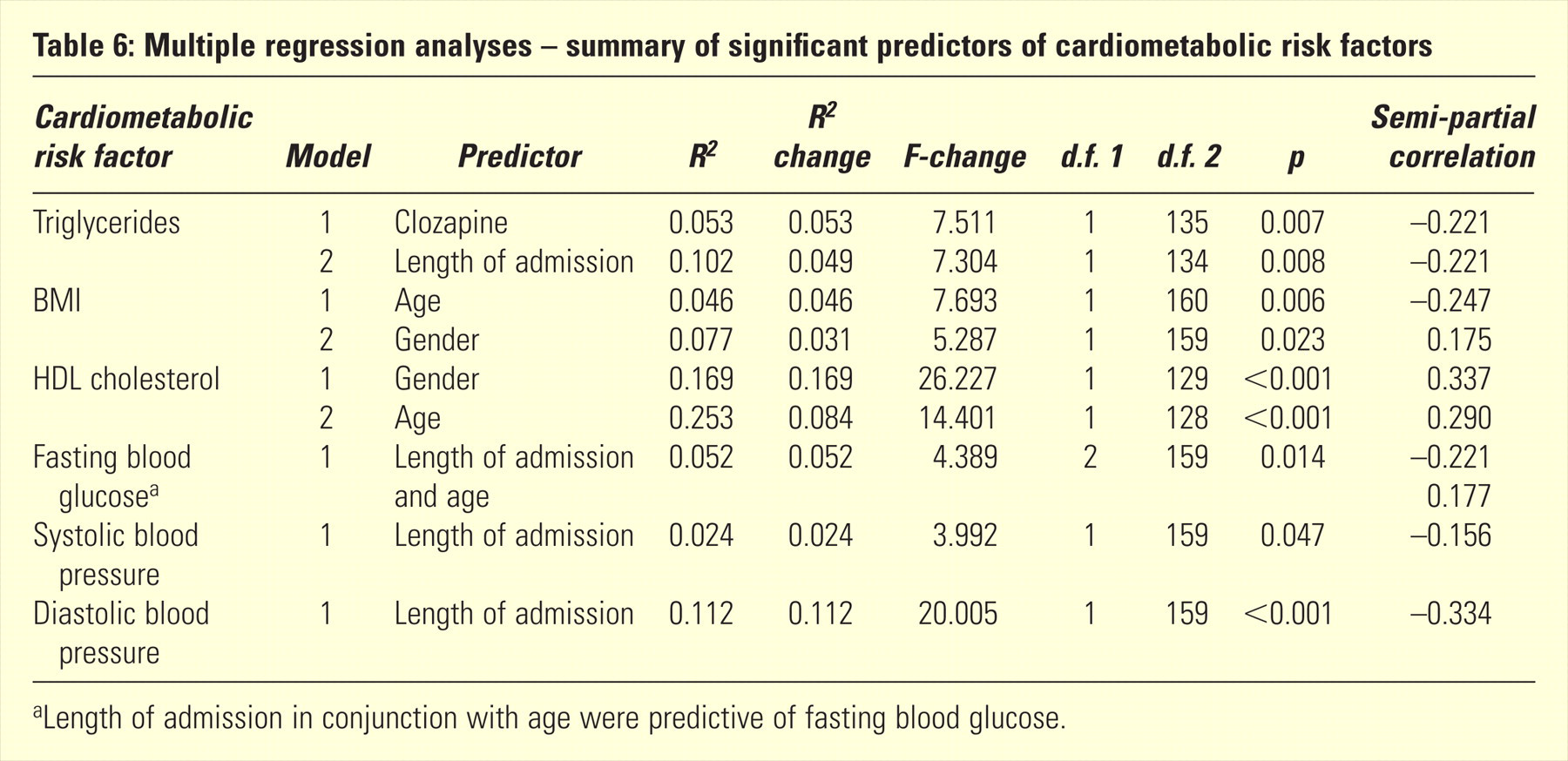
aLength of admission in conjunction with age were predictive of fasting blood glucose.
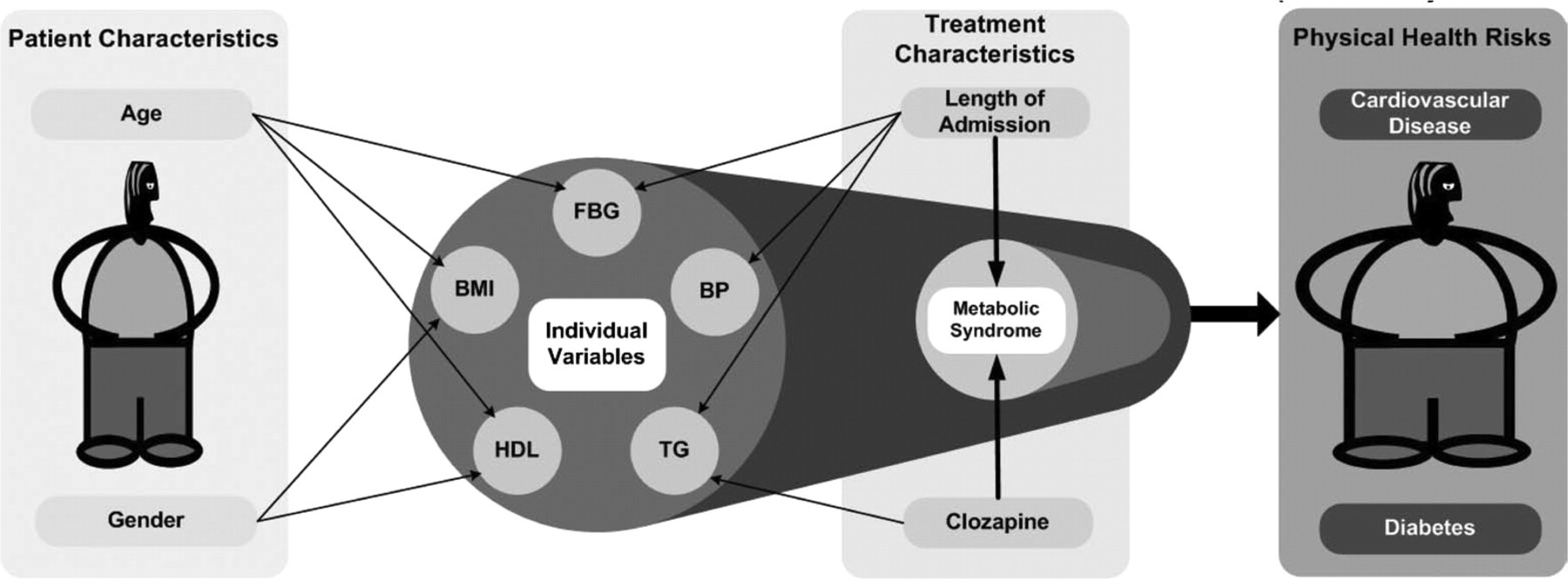
Predictors of cardiometabolic health risk. Direction of predictors: Age: younger age predicted increased BMI and reduced HDL, older age predicted impaired FBG. Gender: females predicted increased BMI, male predicted reduced HDL. Length of admission: shorter length of admission predicted elevated FBG, increased BP, elevated TG and presence of metabolic syndrome. Clozapine use predicted elevated triglycerides and presence of metabolic syndrome. FBG, elevated fasting blood glucose; BP, increased systolic and diastolic blood pressure; TG, elevated triglycerides; HDL, reduced high density lipoprotein cholesterol; BMI, increase in body mass index.
Length of admission was predictive of systolic blood pressure, diastolic blood pressure, fasting blood glucose and triglycerides. In all instances, a shorter length of admission was associated with higher levels.
Clozapine use was predictive of elevated triglycerides and associated with reduced HDL cholesterol (χ 2 =7.51, df = 3, p = 0.049). However, when analyses controlled for other factors such as length of stay, age, gender and smoking status, clozapine use was not a significant predictor of reduced HDL cholesterol.
Smokers were more likely to have reduced HDL cholesterol (χ 2 = 6.95, df = 1, p = 0.009) but this was no longer significant after controlling for age, gender, length of stay and clozapine use.
While age did not predict the metabolic syndrome, there were some age differences in regard to individual risk factors. Age significantly predicted BMI, HDL cholesterol and fasting blood glucose. Younger age was predictive of a higher BMI and lower HDL. Conversely, older age was predictive of high fasting blood glucose.
With regard to gender, this was a predictor of BMI and HDL cholesterol. Females were more likely to have higher BMI levels while males were more likely to have lower levels of HDL cholesterol.
Duration of clozapine treatment
Duration of clozapine treatment did not significantly affect cardiometabolic health (p > 0.05). As illustrated in Figure 3, the results suggest that the negative cardiometabolic effects observed in patients on clozapine emerge early in the course of treatment and are then sustained over a long period of time such that changes occur within the first year of treatment and remain evident for at least 10 years.
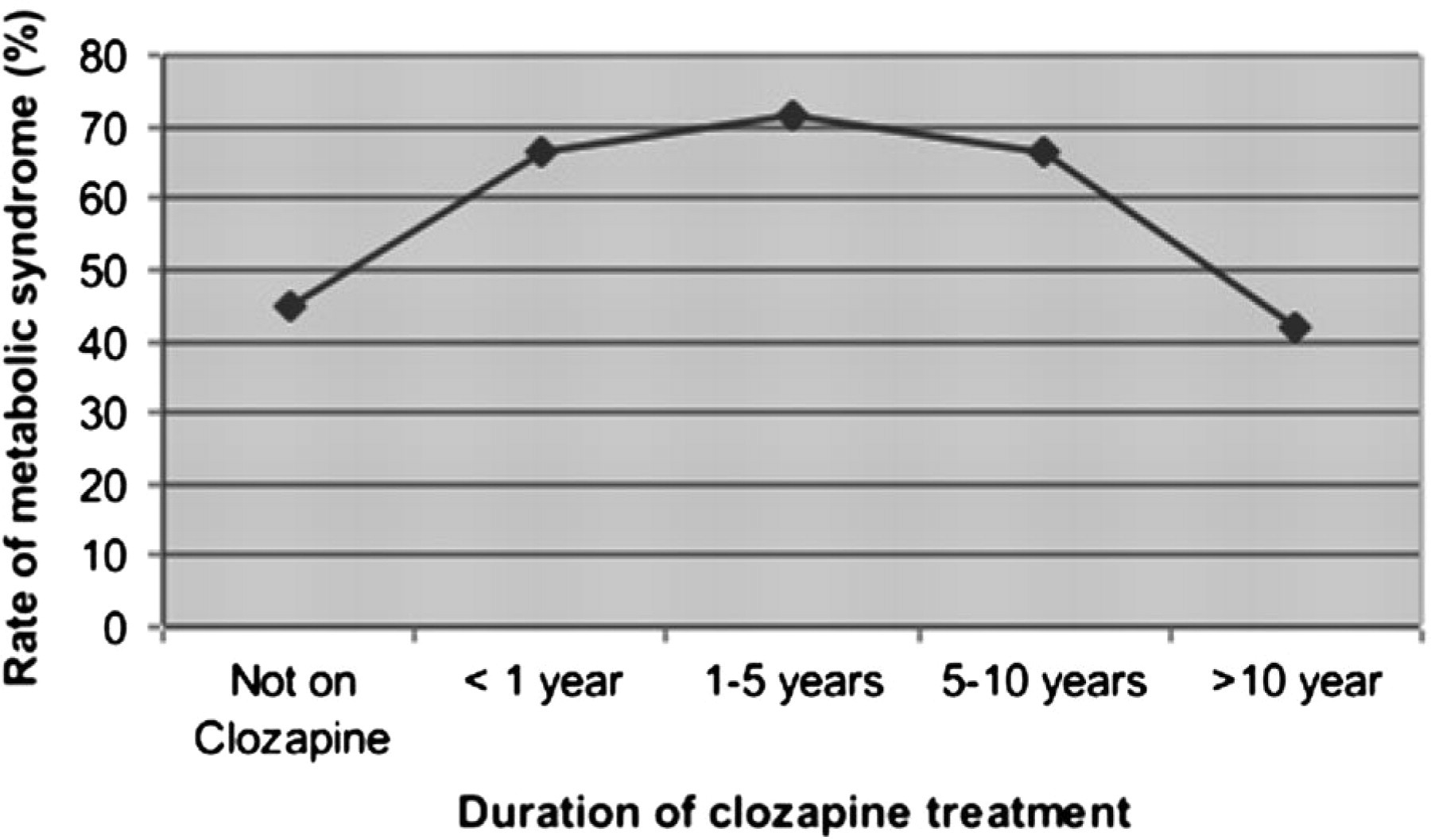
Prevalence of metabolic syndrome in relation to duration of clozapine treatment.
DISCUSSION
Metabolic syndrome is widely acknowledged although, as indicated earlier, its definition lacks uniform agreement. It confers serious disability by way of cardiometabolic risk that limits quality of life and can result in premature death. It is therefore a serious potential consequence of effective treatment that needs to be considered and better understood.
In treating schizophrenia, most guidelines advocate the use of atypical antipsychotics and at some point specify the use of clozapine. 46,47 In practice, clozapine is widely regarded as perhaps the most efficacious atypical antipsychotic and its use in difficult to treat patients reflects its greater potency. However, in conjunction with its favourable therapeutic profile, clozapine also confers considerable risk. It is the medication that is most likely to produce weight gain (particularly abdominal obesity) and metabolic syndrome, and is the one agent that requires greater monitoring because of the risk of neutroprenia. This poses a significant dilemma: the treatment with the greatest potential clinical benefit in the management of schizophrenia is also the one that is possibly the most damaging in the long-term as a consequence of its cardiometabolic effects. Yet, the treatment of schizophrenia, by the nature of the illness, necessitates lifelong antipsychotic medication. Furthermore, the characteristics of those who stand to obtain most benefit from clozapine treatment should also be considered. Patients with treatment-refractory schizophrenia tend to also have a greater degree of cognitive impairment which negatively affects functioning, including living skills and physical health and in turn can increase the risk of poor cardiometabolic health. 48
In this context, the present study is important because it examines the ‘real-world’ use of clozapine in treating schizophrenia and its implications for metabolic syndrome. The findings highlight the high rate of cardiometabolic health risk in non-acute psychiatric inpatients, with over half of the patient population satisfying criteria for metabolic syndrome. The prevalence of metabolic syndrome is almost twice that of the Australian general population, 7–9 but is comparable with other rates reported for psychiatric populations. 5,6,24,25 Olanzapine, also known to cause marked weight gain, was not associated with increased rates of metabolic syndrome in this sample. However, this is not altogether unexpected given the comparatively small proportion of patients taking olanzapine in this population.
Interestingly, a shorter duration of hospital stay was the strongest predictor of metabolic syndrome, and in particular elevated blood pressure, fasting blood glucose and triglycerides. It is not obvious from the data why this is the case but it is possible that those with a longer duration of hospital stay may have benefited from the controlled hospital environment that more easily affords physical health monitoring and the implementation of healthier lifestyle options, such as a catered meal service with associated control of food intake and participation in exercise programs. Alternatively, the finding may reflect the changing characteristics of the patient population arising in the hospital with an increasing number of younger patients with high rates of dual diagnosis that have initiated medication presenting to community services.
While clozapine use significantly predicted metabolic syndrome, the prevalence of metabolic syndrome did not significantly differ according to the length of clozapine treatment, suggesting that such effects occur early in the course of the treatment. This further highlights the imperative for prophylaxis and early intervention when commencing clozapine treatment and proactive monitoring of physical health throughout management.
It is acknowledged that cross-sectional data constrains the strength of our conclusions as regards the duration of clozapine treatment. For instance, those who continue to take clozapine over a lengthy time period are reflective of a patient group able to tolerate side effects which could bias the comparison of those taking clozapine for longer versus shorter periods of time in favour of the former group by virtue of ‘enrichment’ with those doing well. However, upon closer inspection of our sample, this does not appear to be the case. Of the total sample, 54 patients had previously trialled clozapine but were no longer taking the drug and, in the preceding 15 years, records indicated that eight patients had died while taking clozapine. Of those who were no longer taking clozapine, the majority of patients had ceased the medication within a year (65%) and only two patients (4%) had stopped the drug after taking the medication for longer than 10 years. Consequently, the tolerability of clozapine appears to become known early in the course of treatment. Furthermore, the recorded instances of patient deaths while taking clozapine show that these occurred relatively evenly across the duration of clozapine treatment. Two occurred within the first year of treatment, three in period 1-5 years, two in period 6-10 years, and one after more than 10 years of treatment.
Of the individual cardiometabolic risk factors, clozapine predicted impaired triglycerides and was associated with reduced HDL cholesterol. This supports earlier findings that atypical antipsychotics, particularly clozapine, are associated with dyslipidaemia. 49 Of the biochemical measures, elevated triglycerides are considered to be a particularly sensitive marker of insulin resistance and the ratio between triglyceride and HDL cholesterol (≥3) is considered to be a better predictor of insulin resistance than fasting blood glucose alone. 50 The stronger association of clozapine use with biochemical markers, as compared to waist circumference or BMI, suggests that the negative health effects of clozapine are not simply a direct consequence of weight gain but that clozapine also appears to act directly on lipid dysregulation and insulin resistance. 43 , 51 , 52
With relatively high rates of metabolic syndrome evident across all age groups, an increase in the risk of metabolic syndrome with age was not found in the present study. In fact, in comparison to the general population, the rates of metabolic syndrome peaked two to three decades earlier in our sample. 25 , 53 Of note, younger age in this study predicted impaired HDL cholesterol and higher BMI, further reinforcing the point that physical health concerns need to be monitored and addressed from an early age.
Consistent with findings from CATIE, 24 there were no significant gender differences in the overall prevalence of metabolic syndrome, although females had higher rates of central obesity and males had more significant changes in biochemical markers of metabolic syndrome (e.g. HDL cholesterol).
Interestingly, in our sample smoking status approached significance as a predictor of metabolic syndrome and was associated with changes in HDL cholesterol. This is important as cigarette smoking is prevalent in people with schizophrenia 25,54 and is a known risk factor for cardiovascular disease and type 2 diabetes. In our study, 64% of the sample were smokers.
Limitations
The population cohort is itself somewhat unique in that it is a non-acute inpatient rehabilitation facility with very few studies reporting the incidence of metabolic syndrome in a wholly inpatient non-acute sample. However, having used a data set derived from clinical purposes, there are inherent limitations affecting the strength of the conclusions that can be made from this study. The accuracy and timing of the data collected are variable and were not subjected to the rigour of a specifically designed research paradigm. In addition, the cross-sectional nature of the data limits some conclusions, particularly in relation to the duration of clozapine treatment. It is also worth noting that the metabolic syndrome in special populations, such as young people, warrants further evaluation as does further investigation in the community setting, but this was beyond the scope of this study. 55 Also beyond the scope of this study was clozapine-induced myocarditis, which is attracting increasing attention. Despite these shortcomings, the findings from this dataset are comparable to well-controlled studies and the very nature of being a clinical sample highlights the very real cardiometabolic health risks that exist for people with schizophrenia.
Summary and conclusion
Schizophrenia is a debilitating life-long illness that demands psychosocial care alongside pharmacotherapy. Of the medications available, clozapine is perhaps the most effective treatment but one that comes at a price. The initiation of clozapine confers a significant cardiometabolic risk that is realized early in the course of the illness but can be effectively managed provided precautions and preventative interventions are taken. 56 Therefore, when treating schizophrenia, long-term inpatient management need not necessarily result in adverse cardiometabolic consequences.
Footnotes
Acknowledgements
In the past 3 years, Professor Malhi has served on a number of international and national pharmaceutical advisory boards, received funding for research and has been in receipt of honoraria for talks at sponsored meetings worldwide involving the following companies: AstraZeneca, Eli Lilly, Jansen-Cilag, Organon, Pfizer, and Wyeth. Professor Garry Walter has received educational grants from Eli Lilly, Janssen-Cilag and Pfizer, and travel assistance and an honorarium for a talk from Eli Lilly. Danielle Adams, Janice Plain, Michael Herman and Dr Carissa Coulston have no competing interests.