
Abstract
Allegedly to incorporate advances generated by research in the last 15 years, the World Health Organization (WHO) and the American Psychiatric Association (APA) have decided to revise the International Classification of Diseases (ICD) and the Diagnostic and Statistical Manual of Mental Disorders (DSM) respectively. Altering the classification system is a costly and time-consuming exercise that has an important bearing on research, teaching and clinical practice as well as influencing other facets of society such as the courts. Learning to use a new taxonomy is also cumbersome.
Preparations for DSM5 began in 1999. The chair and vice chair of the task force to oversee its development were appointed in 2006, members of the 13 work groups were announced in 2008, and DSM5 is expected to be approved by the APA and published in 2013. Work group members were required to sign a confidentiality agreement and the APA set strict standards concerning conflicts of interest.
“Taxonomy is described sometimes as a science and sometimes as an art, but really it is a battleground.” 1 Development of DSM5 has not been without controversy, as were its predecessors. For example, Robert Spitzer, former chair of the work group for DSM-III and DSM-III-R, and Allen Frances, chair of the DSM-IV task force, criticized the confidentiality agreements and urged the APA's board to make the revision process more transparent. 2 , 3 The posting on the internet of the draft answers some of the criticisms.
This article seeks to make practitioners aware of the proposals by summarizing the changes without delving on their merit or otherwise. Readers wishing to know more, such as the proposed diagnostic criteria for specific diagnoses or the rationale behind changes, should go to the internet posting (http://www.dsm5.org/Pages/Default.aspx). A revision of ICD-10 is also underway, but proposed changes are not yet available. The WHO has put in place a system to allow stakeholders to make suggestions (http://extranet.who.int/icdrevision). The ICD-11 approach is more open-ended than DSM5, which only allowed 2 months for comments (closing 20 April 2010). There is a commitment to make ICD-11 and DSM5 as compatible as possible.
OVERALL STRUCTURE
Dimensional assessment
One of the aims was to provide practitioners with quantitative measures of important clinical areas (e.g., depressed mood, anxiety, anger, substance use, sleep problems) that may be relevant beyond specific diagnostic labels (‘cross cutting’). This dimensional assessment: (i) is designed to be used at the initial evaluation to establish a baseline, and on follow-up visits to track change; (ii) does not relate to any specific disorder and does not serve as a screening test for DSM diagnoses; (iii) relies on self-report ratings by patients or informants; and (iv) may be useful even before a formal diagnostic evaluation is conducted, such as assessing for depression in primary care, identifying suicidal ideation, or rating personality traits.
In this endeavour, DSM5 proposes to follow the NIH's Patient-Reported Outcome Measurement Information System™ (PROMIS; www.nihpromis.org). This system consists of short questionnaires that can be used to establish a patient's status in comparison to national norms. Cross-cutting assessment consists of a brief set of items (‘Level 1’ assessment) that link to a more thorough examination on a domain (e.g. sleep), if warranted. The initial assessment could be completed by the patient or informant on a single sheet of paper or computer screen. If any of the domains is rated as clinically significant, additional questions would be asked (‘Level 2’ assessments).
Multiaxial diagnosis
The task force recommends collapsing the existing axes I (clinical disorders), II (personality disorders), and III (general medical conditions) into one axis that contains all psychiatric and general medical diagnoses. This change would make DSM5 more consistent with the ICD, but is a departure from the DSM philosophy of the last 30 years.
PROPOSED NEW DIAGNOSES
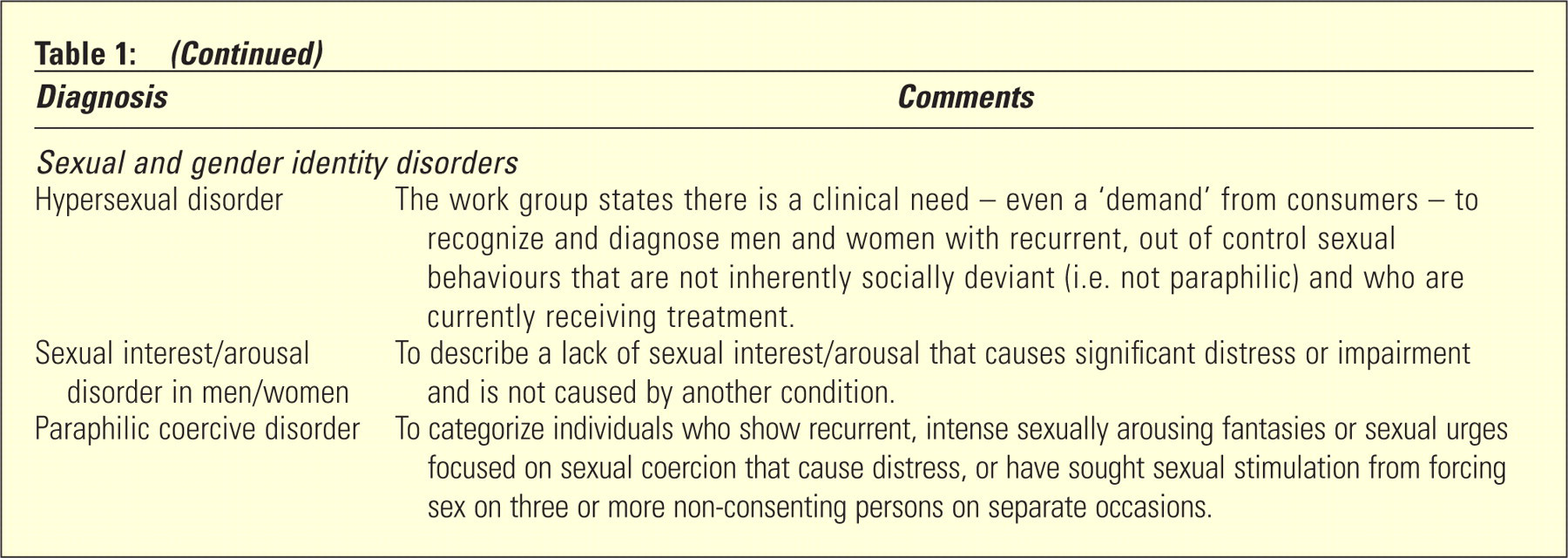
The most significant additions proposed for DSM5 are listed in Table 1. Some of these changes have already attracted professional attention, 4 , 5 while others (e.g. paraphilic coercive disorder) have been criticized in the media. 6
Some of the proposed new diagnoses for DSM5 (source: http://www.dsm5.org/Pages/Default.aspx)
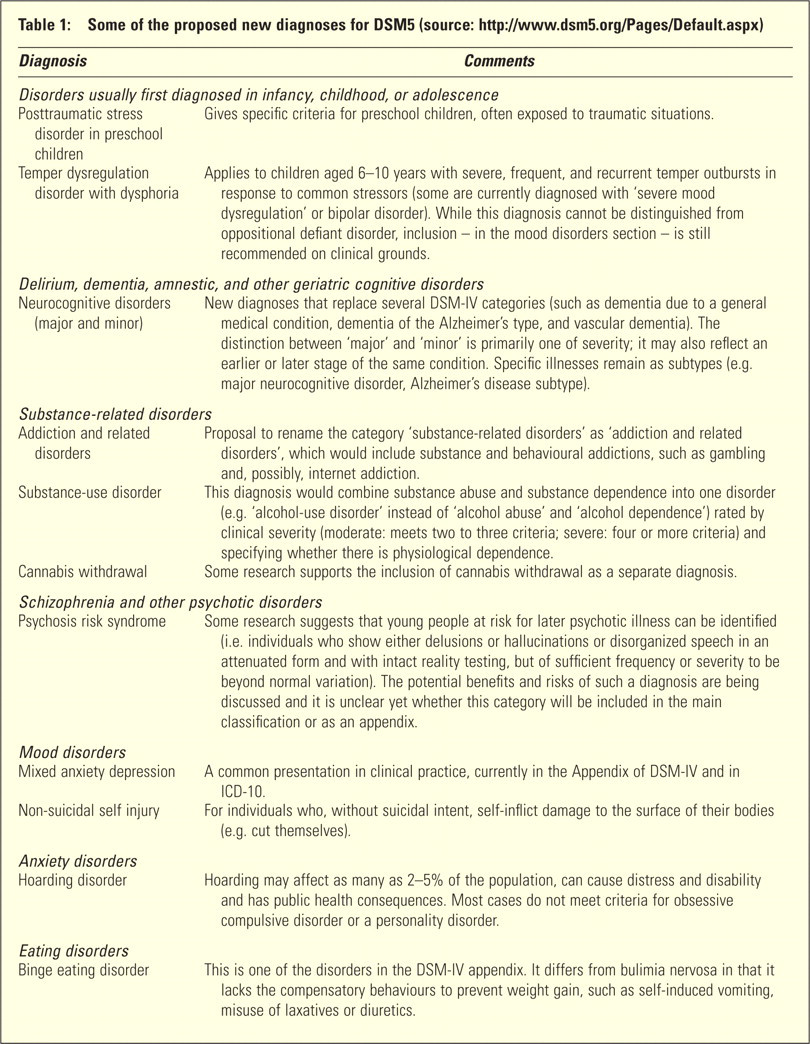
DSM5 also recommends abandoning a number of DSM-IV diagnoses. For example, the major neurocognitive disorders replace several DSM-IV categories (such as dementia due to a general medical condition, dementia of the Alzheimer's type, and vascular dementia), and a diagnosis of substance-use disorder subsumes both substance abuse and substance dependence, which disappear.
OTHER PROPOSED CHANGES
Child and adolescent disorders
The work group is considering several options for attention deficit hyperactivity disorder: (i) maintaining the present criteria but without subtypes; (ii) discontinuing the predominantly hyperactive/impulsive and predominantly inattentive subtypes; and (iii) creating a new attention deficit disorder (ADD) diagnosis with the same inattention criteria as in DSM-IV predominantly inattentive subtype but with no hyperactive/impulsivity symptoms. There is a proposal to also broaden the age of onset from the current age 7 to before age 12.
A ‘callous unemotional’ specifier is proposed for conduct disorder – on the basis that conduct-disordered children who show lack of remorse or guilt, are unable to show empathy, or display shallow or superficial emotions, have a worse outcome. The label of mental retardation is to be changed to intellectual disability. ‘Autism spectrum disorders’ becomes the new name for a group comprising autism, Asperger's disorder, childhood disintegrative disorder, and pervasive developmental disorder not otherwise specified. The rationale is that distinctions among these conditions are inconsistent over time, vary across sites, and are often associated with severity, level of language or intelligence rather than with the specific features of the disorder.
Substance-related disorders
Substance-related disorders are to be renamed ‘addiction and related disorders’, which would comprise substance and behavioural addictions – such as gambling and, possibly, internet addiction – and resulting in the disappearance of the current ‘dependence’ categories. The term ‘dependence’ is to be used to refer only to physiological dependence. Thus, tolerance and withdrawal symptoms would not be counted for the diagnosis of substance use if they appear during appropriate medical treatment with prescribed medications.
Schizophrenia and other psychotic disorders
Apart from the creation of the controversial 4 category of ‘psychosis risk syndrome’ (Table 1), changes include removing the schizophrenia subtypes (i.e., paranoid, disorganized, catatonic, undifferentiated) on the basis that they lack validity and clinical usefulness. However, catatonia is to be added as specifier in any disorder within the schizophrenia and the mood disorders groups, on the grounds that catatonia is often not recognized or treated.
Diagnostic criteria for schizophrenia are simplified slightly. The main change is a recommendation for all patients to be cross-sectionally rated from 0 (not present) to 4 (present and severe) according to nine dimensions: hallucinations, delusions, disorganization, abnormal psychomotor behaviour, restricted emotional expression, avolition, impaired cognition, depression, and mania.
Mood disorders
There are few changes in the depressive disorders – regrettably, the label ‘major depression’ remains. It is proposed that symptoms for hypomania and mania must be present most of the day, nearly every day (to be consistent with the criteria for depression) and “represent a noticeable change from usual behaviour”. This operationalizes episodicity more clearly, particularly in children and adolescents.
Anxiety disorders
This section is to be renamed ‘anxiety and obsessive-compulsive spectrum disorders’. Separation anxiety disorder (currently in the child and adolescent section), body dysmorphic disorder (currently a somatoform disorder), tricotillomania (currently an impulse control disorder) and, possibly, tic disorders are to be moved to this section.
Somatoform disorders
Somatoform disorders are to disappear and a new section, ‘somatic symptom disorders’, created to include somatoform disorders, psychological factors affecting medical condition, and factitious disorders. This change is intended to reflect the key role of physical symptoms or concern about medical illness in the clinical presentation. However, it does not assume a shared aetiology. Somatization disorder, hypochondriasis, undifferentiated somatoform disorder, and pain disorder are to be grouped into a new category: complex somatic symptom disorder. The term ‘complex’ indicates that symptoms must be persistent and must include both somatic symptoms and cognitive distortions.
Eating disorders
Binge eating disorder is to be added (Table 1). Pica, rumination, and feeding disorder of infancy or early childhood are to be relocated from the child and adolescent section into this section.
Sleep disorders
Substantial changes are proposed for this section, mainly reflecting the inclusion of conditions such as Kleine Levin syndrome, obstructive sleep apnoea, and restless leg syndrome. The reason given for this is “to educate non-expert sleep clinicians (such as psychiatrists and general medical physicians) about sleep disorders that have mental as well as medical/neurological aspects”.
Personality disorders
The work group recommends a revised definition of personality disorder (PD) – failure to develop a sense of self identity and the capacity for interpersonal functioning in the context of the individual's cultural norms and expectations, which have persisted for several years and are not the result of other disorders. Five specific PDs are proposed: borderline, antisocial/psychopathic (possibly with subtypes), schizotypal, avoidant, and obsessive-compulsive. Personality functioning is to be rated from no impairment (0) to extreme impairment (4). PDs would be diagnosed using a combination of core impairment in personality functioning and specific pathological personality traits. Six broad, higher-order personality trait domains (negative emotionality, introversion, antagonism, disinhibition, compulsivity, schizotypy) with 4–10 lower-order, more specific ‘trait facets’ are to be considered. As it stands, the PDs section is difficult to follow, complex, and it is unclear how it will work in practice.
CONCLUSION
It would appear from the proposed changes that 15 years of research have made only a modest contribution to psychiatric taxonomy. The changes proposed seem far from drastic: the main diagnostic categories and disorders remain largely the same as in DSM-IV. Many of the modifications entail moving specific disorders from one section to another, deleting disorders that have had little use in practice, or changing the name. The substance related disorders and PDs sections have been changed the most. It remains to be seen whether the proposed new diagnostic categories, as shown in Table 1, will make it to the final version. The architect of DSM-IV, 7 who seems on a crusade to discredit DSM5, believes that several of the proposed new diagnoses (e.g. binge eating, mixed anxiety depression, minor neurocognitive problem, risk of psychosis, and temper dysregulation), as well as changes to existing diagnoses (e.g. attention deficit hyperactivity disorder, bipolar disorder, and major depressive disorder) “could potentially set off at least eight new false positive epidemics of psychiatric disorder.”
Footnotes
Acknowledgements
Jennifer Bergen is thanked for her suggestions and editing.
The author reports no conflicts of interest. The author alone is responsible for the content and writing of the paper.