
Abstract
Aggression and self harm are two common but problematic behaviours found on a psychiatric ward. Aggressive behaviour includes verbal abuse and physical aggression (e.g. hitting, kicking, spitting, punching etc). An Australian study reports between 41% and 90% of child and adolescent inpatients either threaten or actually assault other patients or staff members during a psychiatric admission. 1 This is not surprising when one considers that aggressive behaviours are also one of the most common reasons for referral in young people presenting to a child and adolescent mental health inpatient service. 2 Self harm can be deliberate or non-deliberate. Deliberate self harm may be defined as “a direct behaviour that causes minor to moderate physical injury, that is undertaken without conscious suicidal intent, and that occurs in the absence of psychoses and/or organic intellectual impairment”. 3 One study reported that 47% of children and adolescents harmed themselves while resident in a psychiatric inpatient unit. 4 Adverse outcomes of aggression and self harm include injuries and distress to both patients and staff. One survey found that 43% of nursing staff stated that they felt unsafe in their work place after experiencing violence. 5 These high frequencies are of concern and indicate the need to prioritise the provision of a safe environment for both patients and staff of mental health inpatient units.
Seclusion should only be used as a final option in situations that pose a significant danger to the child and others. 6,7 Seclusion is typically locked-door confinement in a safe room. 8 It is often a consequence of aggression or self harm behaviour. Seclusion may be used inappropriately for punitive or convenience purposes. 9 Many inpatient settings have begun to explore mechanisms for reducing the use of restraint and seclusion while maintaining staff and patient safety. 10 In the last decade the use of seclusion has been questioned, with no controlled studies supporting the use of seclusion or restraint in clinical practice. 11 Previous studies have shown a significant reduction in seclusion/restraint in child and adolescent inpatient units due to programming changes on the unit. 6 One of the interventions that appears to be successful in reducing the use of restraint is collaborative problem solving therapy. This therapy aims to find social and cognitive pathway impairments and tries to provide the patient with problem-solving skills. 12 Case studies have shown that multi-strategy methods reduce seclusion and restraint numbers. 13 Staff training has also been found to be a vital component of reducing seclusion in an inpatient environment. 9 This is likely to be because staff training improves staff communication and leads to more consistency in behavioural management. 9
Concern about seclusion has been raised because of the possible adverse consequences of its use. 10 Fatalities are the most extreme adverse outcome of seclusion. 10 Many patients and staff have been injured following seclusion. 14,15 Apart from the physical injuries that result from seclusion, there is increasing concern for the psychological impact on the children and staff involved in the young person's care following seclusion. 8 Several studies have suggested that the use of seclusion might be counter therapeutic. 7,9 There is also literature that suggests that seclusion and restraint, typically employed to reduce aggression and maintain safety, actually heighten aggressive behaviour and place staff at greater risk of assault and injury. 10
The use of seclusion to manage aggression has also been found to have a number of limitations. There is little evidence that seclusion changes aggressive behaviour or even serves any therapeutic function. 9 New treatment approaches aim to lower the use of seclusion and restraint. 16 This is demonstrated in the study that was conducted by Dean and colleagues 9 where standardized behavioural management reduced the frequency of aggressive behaviours, staff injuries, use of restraint and use of security services. However, it is logical that the best way to minimize seclusion while keeping a safe environment is to lower the frequency of aggressive or self-harming behaviour on the ward.
Despite the high prevalence of aggression and self harm on psychiatric wards and the serious consequences of these behaviours, these areas are relatively under researched. Interventions for self harm that have found some empirical support include problem-solving therapy, cognitive behavioural therapy and dialectical behaviour therapy. 17,18 Dialectical behaviour therapy is one of the most promising of these as it directly targets suicidal behaviour, behaviours that interfere with treatment delivery, and behaviour that severely compromises the client's quality of life. 19 To prevent aggression, suggestions in the literature include risk assessment, staff training programs, de-escalation approaches and behavioural modifications methods, 8 although as yet there is no clear evidence as to the effectiveness of these interventions. 6 Bowers et al. 20 reviewed environmental factors on the ward and concluded that staff factors have a strong influence on rates of adverse incidents in wards. These factors are the degree to which staff positively value patients, their ability to regulate their own emotional reactions of anger and fear towards patients, and provision of an effective structure of rules and routines for patient conduct.
This study describes the trends of aggression, self harm and use of seclusion on a child and adolescent mental health inpatient unit over a 3 and a half year period (2006–2009). The study also details the ward milieu changes (e.g. changes in staffing levels and number) over this time, and describes various treatment interventions that had been implemented. The present study evaluated the impact of ward milieu changes and treatment interventions on the incidence of self harm, aggression and seclusion in a child and adolescent mental health inpatient unit. It was hypothesized that these changes would result in a reduction in self harm, aggression and seclusion.
METHOD
Setting
The paediatric mental health ward has eight beds for ages 6–16 years. The first beds were opened in May 2004 but it was not until the end of 2004 that all eight beds were open 7 days a week.
Participants
Patients were included in the study if they were admitted between January 2006 and August 2009 inclusive and had at least one incident of self harm or aggression reported in the Incident Information Management System (IIMS). De-identified nursing work schedules were collected for 1 year (2006–2007) and correlated with the number of incidents per shift.
Data collection
Data on adverse events were collected using IIMS. IIMS is an electronic program used by nurses and psychiatrists for reporting adverse incidents. Date, time, a description of the incident and the outcome for the patient are reported. The IIMS database was reviewed for events of self harm, aggression and seclusion during 2006–2009. Cases of absconding or medication errors were excluded.
The following is an example of an incident reported in IIMS: “Patient inserted a refill part of a ballpoint pen completely under the skin of his lower left leg”. This incident was categorized as self harm. An aggressive incident included both physical (kicking, hitting etc.) and verbal (insulting, threatening, screaming etc.) aggression. The episode needed to be severe enough to be reported as an incident, so verbal aggression was only reported if severe and disruptive.
Data analysis
The total number of episodes per month of self harm, seclusion and aggression were graphed using Microsoft Excel (2007). These data served as dependent variables for linear regression models, with the 44 months of study as the independent ordinal variable. To correct for the outliers a sensitivity test was performed. Slope (Beta) and P for trend values (P ≤ 0.05) were obtained through linear regression. Analyses were conducted using SPSS version 17. The beginning and end of various interventions was superimposed on the graphs.
The various interventions that were implemented on the ward during the study period included: staff training in use of seclusion and restraint and dialectical behaviour therapy (DBT), a therapy that targets self harm and suicidal behaviours; 11 a behavioural program where patients earned greater freedom and more access to activities for safe and appropriate behaviour; and an activity program where all but the most unwell patients had five sessions of structured exercise a week.
RESULTS
Frequencies of aggression and self-harm
During 2006–2009 a total of 475 incidents were reported in IIMS, comprising 292 events of aggression (61%) and 139 of self harm (29%). Forty-four incidents (9%) were excluded because they were not aggression or self harm.
A total of 294 children, 61% female, were admitted to the unit during the study period. Of these patients, 84 were aggressive during hospitalization (29%) and 34 harmed themselves while on the ward (12%). The average age of the patients at the time of the incident was 13 years (SD = 2), with 62% of those who were aggressive and 82% of those who harmed themselves being female. The three most common diagnoses were depression (52%), conduct disorder (35%) and posttraumatic stress disorder (29%). There was no significant change in diagnostic groups over the period of the study.
During the study period, a decreasing trend can be seen for all types of incidents (Figures 1 and 2). However, in the first 6 months of 2009 the rates of seclusion and aggression started to increase again.
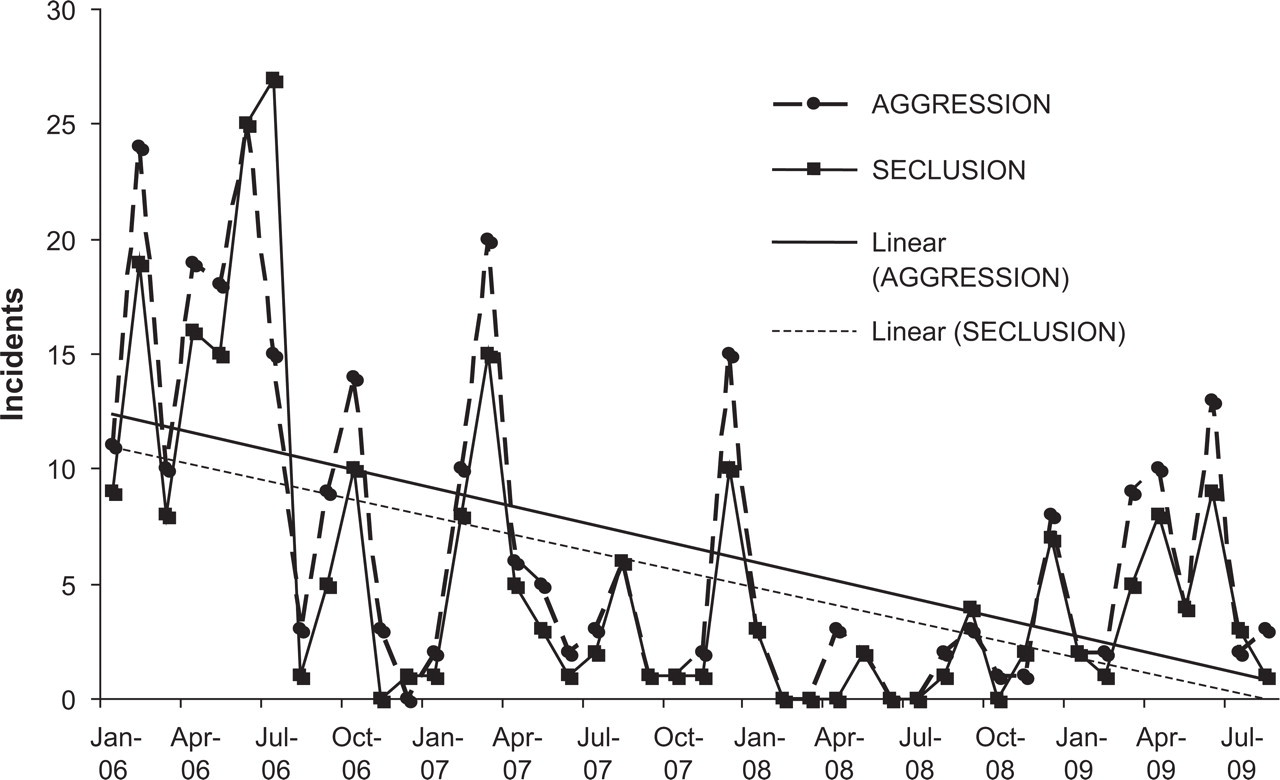
Trends of aggression and seclusion over time.

Trends of self harm over time.
An analysis of the regression lines indicates that aggression and seclusion significantly decreased over time (respectively aggression: Beta= 0.25, P for slope < 0.0001; seclusion: Beta = 0.24, P for slope < 0.0001). These results suggest that 25% of the variance in aggression can be explained by time. For seclusion, 24% of variance was explained by time.
There was a reduction in aggression (150 incidents to 23 incidents per year representing a 6.5-fold reduction) and seclusion (from 135 to 20 incidents per year representing a 6.8-fold reduction). Seclusion and aggression were highly correlated (Pearson correlation: 0.37, P < 0.0001); seclusion followed 73% of aggressive events.
There was a threefold reduction in events of self harm, from 60 incidents in 2006 to 20 incidents in 2008 (Figure 2). Seclusion was used in 35% of self harm events.
Patients with multiple incidents were common. A decrease in patients with multiple incidents (defined as more than five per month) was observed. In 2006 there were 13 patients with multiple incidents compared to two patients in 2008. To check if these patients were not biasing the trend lines, a sensitivity test was performed. All patients with more than 10 incidents within 1 month were excluded from the regression analysis. Regression results were highly similar, indicating that the outliers did not have an undue influence on the trend lines.
Ward interventions
During the study period three different interventions were commenced on the ward (Figure 3). The behavioural program was implemented on the ward by the end of 2007. DBT and the activity program both started in May 2008. During this period the frequency of adverse events was relatively low. However, an increasing trend was seen in the first 6 months of 2009. Average rates of adverse events increased from 4.7 incidents per month during DBT to 7.7 incidents per month while DBT was temporarily stopped (November 2008 to May 2009). For seclusion, the average almost doubled, from 2.2 incidents during DBT to 4.1 incidents.
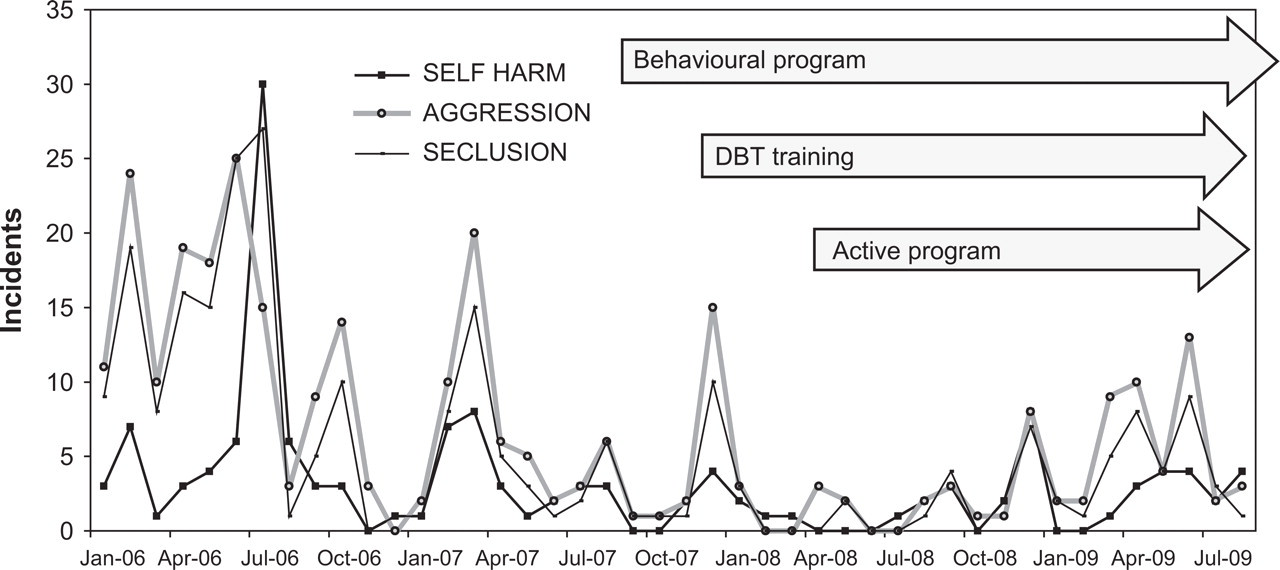
Interventions on the ward.
Staff
During the last 3 years, different changes occurred on the ward in terms of staff composition and staff training (Figure 4). In 2006 the current Nurse Unit Manager began working in that role. This resulted in a change of leadership, the commencement of a full complement of nursing staff and the beginning of staff training. Training for nurses at this time included aggression management (de-escalating potentially aggressive episodes in patients), restraint training and DBT. Figure 4 shows a significant decrease from July 2006 after full staffing, new nurse manager and the commencement of staff training.
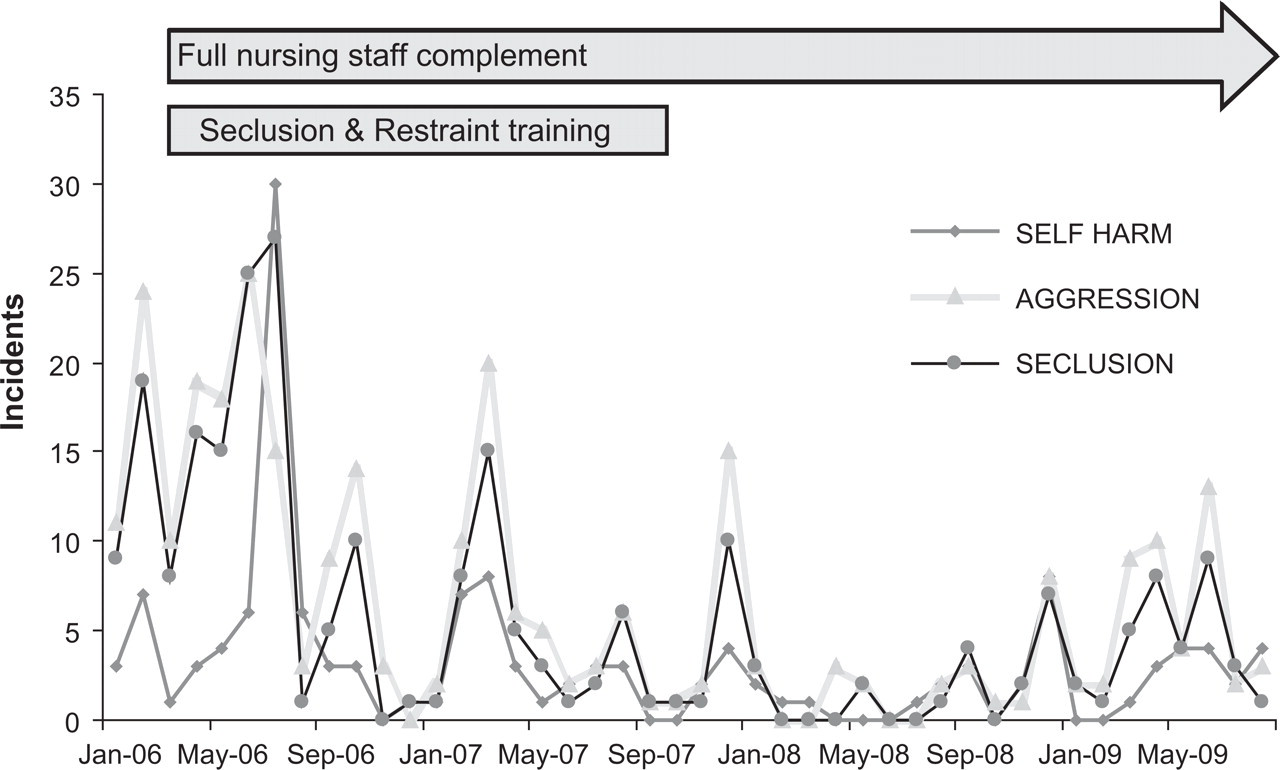
Seclusion, self harm and aggression rates over time as a function of staff factors.
The total amount of adverse events and seclusions that occurred when each staff member was on duty were calculated for 1 year to determine if there was a correlation between particular staff members and incidents of aggression. These figures were corrected to allow for accurate comparisons between full-time and part-time staff. The average number of incidents per nurse was 24 for seclusions (range: 4–52; SD = 11) and 36 for aggressive/self harm incidents (range: 6–70; SD = 14). One nurse had 70 incidents of aggression/self harm and 52 events of seclusion, both of which were more than two standard deviations above the mean. Another nurse only had six incidents of self harm/aggression, which was less than two standard deviations below the mean. Thus, there were two nurses out of 19 nurses who had significantly different rates of seclusion and aggressive/self-harm incidents from the other nursing staff (P < 0.05). Agency staff did not differ in average numbers of incidents from permanent staff.
DISCUSSION
The high incidence of self harm and aggression in young people admitted to psychiatric inpatient units has major implications for the prevention and management of these problems. This retrospective study was designed to investigate whether in the past 3 years various interventions, individual staff members and changes in staff composition and leadership on a children's hospital inpatient psychiatric ward were linked to self harm, aggression and seclusion rates. A significant decrease in aggressive incidents and use of seclusion was observed, while there was a trend for rates of self harm to decrease. There was no one unique factor explaining the decrease in incidents, but rather a combination of factors.
Having a full complement of nursing staff who had all completed some basic training is likely to have contributed to the decrease in adverse incidents. Previous research has shown that rates of adverse incidents increased when permanent staff took leave. 18 The importance of the institutional culture is often underestimated. As Levin 21 points out, “Staff can help the patient remain stable and calm when the milieu itself is stable and calm”. Staff who feel well trained, self confident and are open to emotions are able to engage with patients more ably and are in a better position to implement behavioural therapies. Thus, staff training is of great importance, and is likely to have contributed to the decrease of adverse incidents observed in our study.
Another crucial issue is that of finding the isolated staff member with significantly more adverse incidents and more use of seclusion on his or her shifts. This person might have different treatment approaches to their colleagues and is possibly either more critical or more fearful of the patients than other staff. This is a difficult but crucial issue to consider when managing an inpatient unit. While additional training can help such staff members acquire skills, their attitudes will be more difficult to change. An approach such as Levin's, where staff are encouraged to look for the meaning behind the behaviour, may be of more use. 21
The activity program and behaviour program also could have contributed to the decrease in aggression, self harm and seclusion. Past research has found that maintaining a therapeutic milieu that keeps patients engaged and occupied reduces the potential for aggression 7 and builds self confidence. 22
Finally, an apparent increase in rates of incidents was seen when the DBT program was temporarily ceased. Previous research has indicated that DBT effectively reduced self-harming behaviour. 23 This study also suggests that DBT may also reduce aggressive behaviour in patients. It would make sense that the strategies used by DBT, including tolerating negative affect without acting out, and believing that the patient is doing the best that they can in the current circumstances, could also reduce aggressive behaviour when an adolescent feels angry. Such beliefs could also help a staff member respond to an angry child in a calmer fashion.
Limitations
The main limitation of our study was that it was based on formal records of adverse incidents reported by nurses. It is known that these records are often incomplete and might be subject to bias due to different thresholds for reporting between different staff members. The second limitation was that multiple interventions were implemented in the same time period, which made it difficult to decide which interventions made a significant difference. We also did not include an objective measure of staff adherence to the DBT model.
CONCLUSION
Although the generalisability of the findings are limited by the study's retrospective nature and reliance on formal records, the study provides a snapshot of a natural setting in which trends emerged with therapies such as DBT, staff training and staff composition contributing to lower rates of seclusion, self harm and aggression. Further research of a prospective nature is required to more formally test different interventions. A more detailed measure of individual staff–patient interactions would also be useful.
Footnotes
Acknowledgements
We would like to thank Dr Jenny Peat for her assistance with statistical analysis and Dr Lucres Nauta for the supervision of EB and LK at the Vrije Universiteit.
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.