
Abstract
Epidemiological surveys show a high prevalence of mental illness in Australia. 1,2 As mental health literacy improves with community awareness campaigns, 3 general practitioners (GPs) remain at the primary care forefront of assessment and management. While GP training has clearly improved in the identification and treatment of mental illness, many GPs value specialist input.
Recognizing the need to support GPs in working with mentally ill consumers, the Australian Government made significant additions to the Medicare schedule, including referrals to registered mental health practitioners, 4 and Items 291 5 and 293. 6 These enable GP referral to psychiatrists for one-off assessments, incorporating a written management plan provided to consumer and GP.
In South Australia (SA), a service called GP Psychiatric Assessment SA (GPPASA) was developed cooperatively between the SA Department of Health, the Royal Australian and New Zealand College of Psychiatrists (SA Branch) and SA Divisions of General Practice (SADI). Previous articles have documented the value to GPs of specialist assessment, 7 and psychiatrist satisfaction in providing such a service. 8
However, no publications could be found on consumers’ (and carers’) views of this service, nor on one-off assessments. As the end goal is to improve the patient's mental health, it is appropriate to explore consumer views. Consumer involvement and input is an important factor in the modification and improvement of provision of mental health services. 9
This study explores consumers and carer views of Item 291 assessments, and whether the goal of improvement in mental health was being achieved.
METHOD
A steering group comprising GP, psychiatrist, consumer and carer developed an evaluation plan. A project officer was employed under a grant, and ethics approval was sought and obtained. The intake worker receiving calls at the GPPASA single point of contact was trained to ask the referring GP to invite participation from the referred consumer. When appropriate, consumers were contacted by the project officer, provided with detailed project information and then signed consent.
The project officer met the consumer on three occasions, for quantitative and qualitative data collection.
general levels of satisfaction with the overall process, including understanding of what was to be gained;
whether expectations were met, particularly around provision and implementation of a management plan;
whether implementation of the management plan promoted improvement, or caused problems.
Interviews were recorded using a tape recorder, transcribed verbatim and analysed for themes.
RESULTS
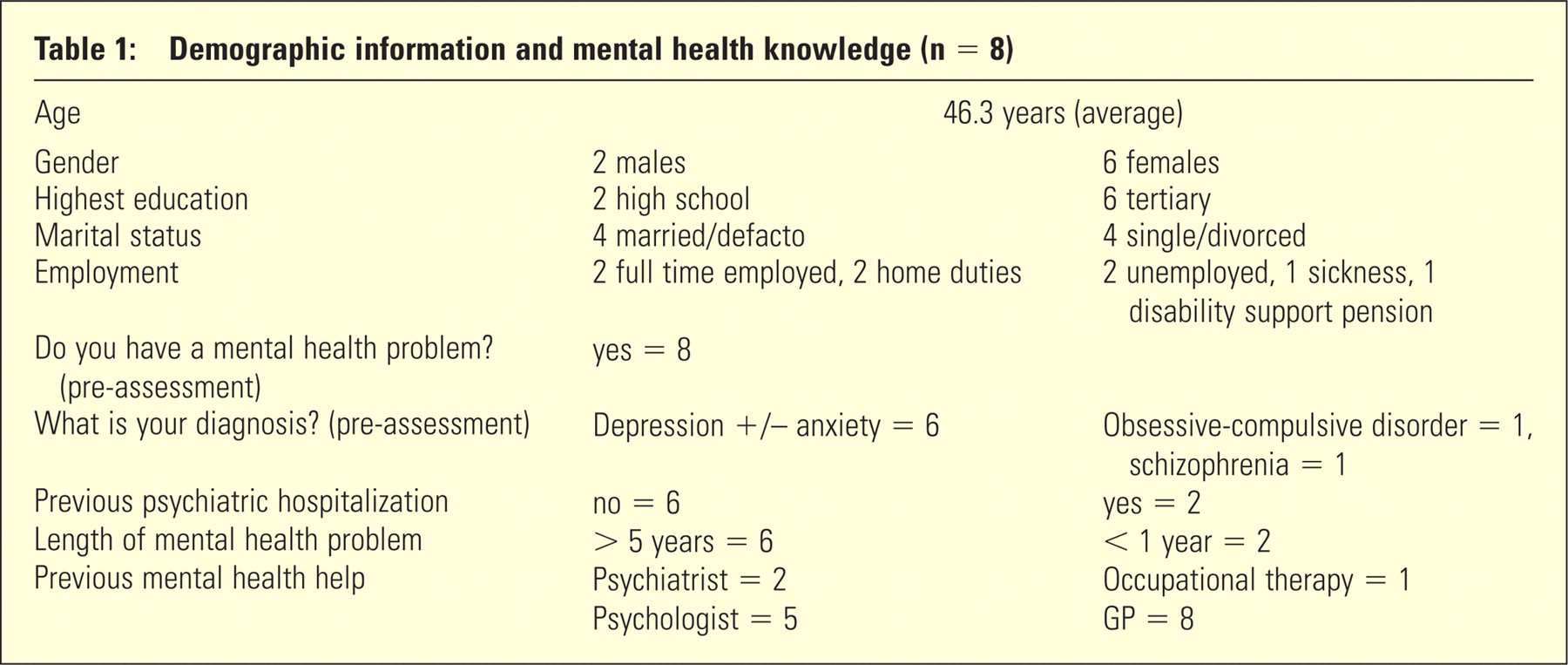
Eight consumers and one carer completed the demographic items and interview. Four consumers completed data collection at all collection points. Demographics and mental health knowledge are shown in Table 1.
Demographic information and mental health knowledge (n = 8)
Qualitative data
Eight consumers undertook the semi-structured interviews. Themes included:
All understood the process of referral: GPs had explained that the appointment was for a one-off assessment.
All were pleased about psychiatric referral, with several welcoming a second opinion: the psychiatrist had specialized training, providing extra expertise.
All had discussed the management plan with the psychiatrist at interview although two had not received a written plan.
All had seen their GP 2 weeks following assessment.
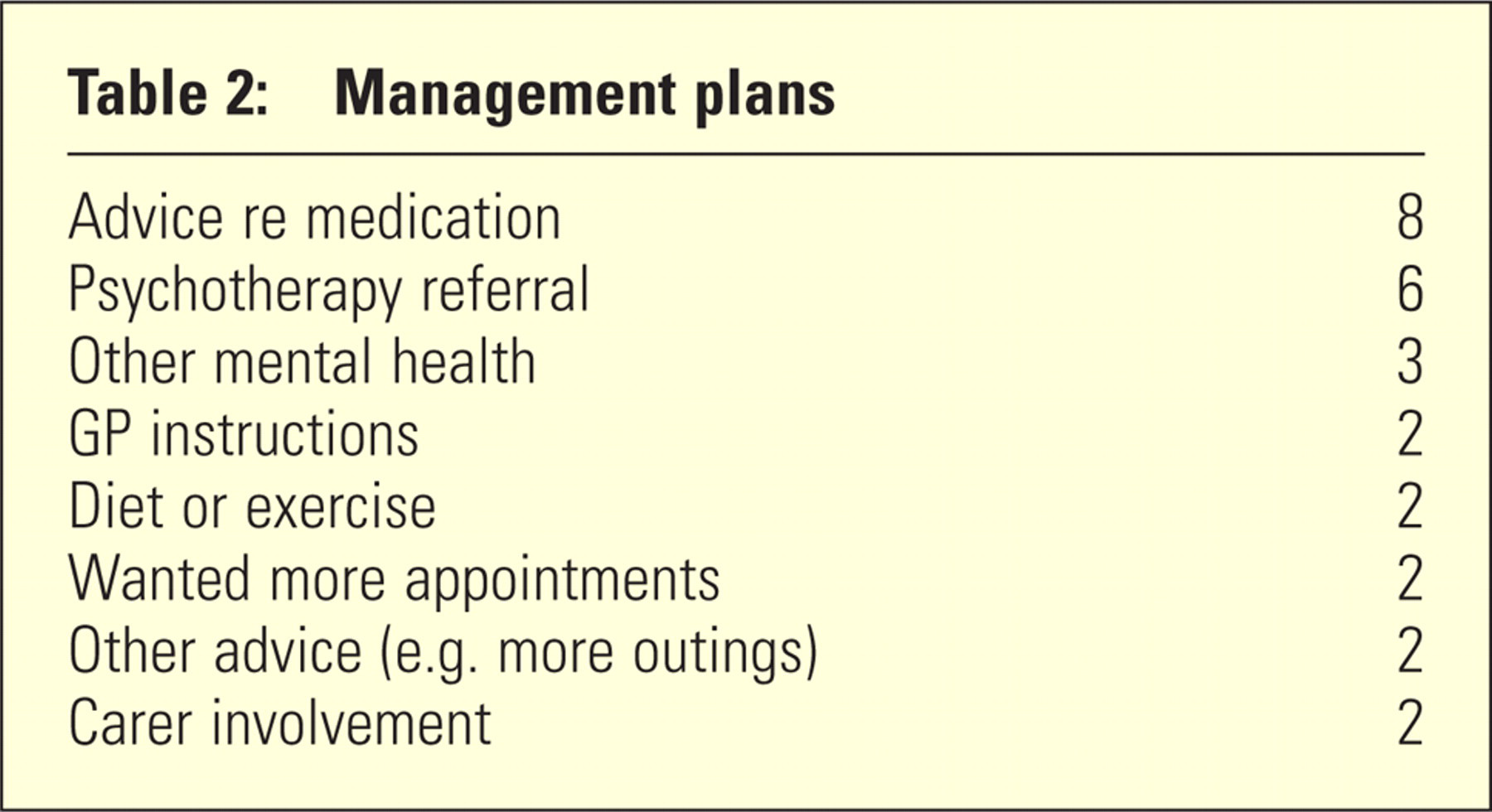
Management plans included changes of medication, either substituting a new medication, or increasing existing medications. Three consumers were satisfied with clarity of diagnosis and a well-articulated management plan (Table 2).
Psychological therapy was suggested in six cases and was already being implemented in five of these. One appreciated referral to a comprehensive outpatient program.
Some consumers preferred further psychiatric follow-up but others saw one appointment sufficient – they were happy with GP and, if suggested, psychology follow-up.
Several enjoyed better understanding of their mental illness generally and the role of medication. One had benefited by subsequent telephone clarification of medication issues with the psychiatrist.
Regarding management plan implementation, seven patients indicated smooth progress, although one indicated it was too early to see positive results.
Consumers valued the opportunity to have a thorough review of their mental health and overall lives: Comments included “Just understanding … medication … just the ins and outs of what … to do”, and “Finally got a diagnosis that I should be on this …. and that was a relief to me. Yeah … it was lucky that he agreed with the doctor … they were on the same page”.
Management plans
Few negative outcomes were mentioned, although several opportunities were offered at interview.
One consumer voiced concerns her GP was not active enough in following the psychiatrist's plan and suggested GP education regarding this.
One consumer did not feel they improved (“…what he said, I know it already … I'm not satisfied … I feel nothing happened like I'm still the same …”).
One psychiatrist was 90 minutes late.
One person was unhappy that the suggested mental health follow-up was unmanageable because of distance from home.
Quantitative data
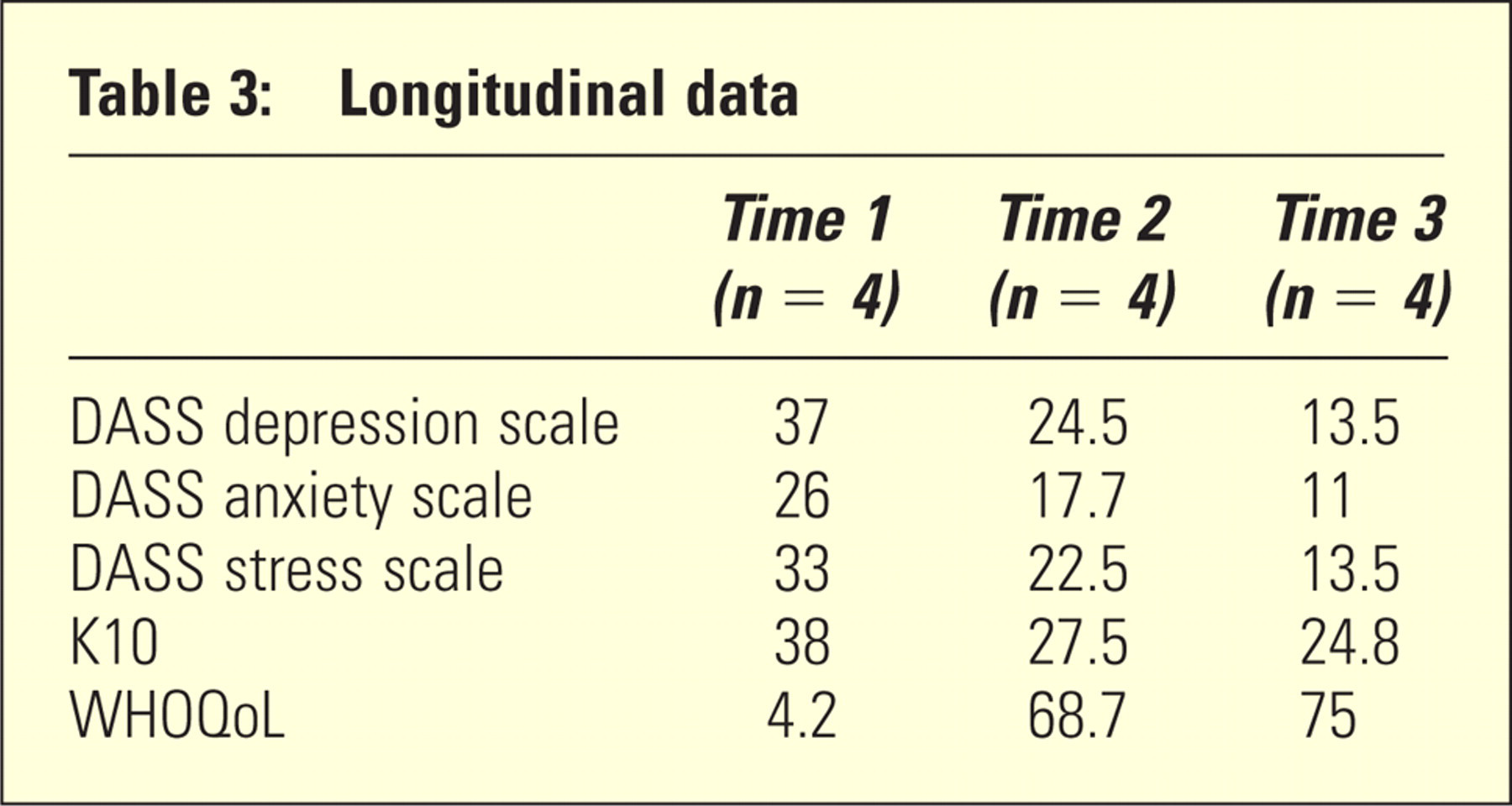
Consumer enrolment and follow-up was problematic, with only four consumers providing information at all three planned time points (Table 3).
Longitudinal data
DISCUSSION
Consumer and carer enrolment was disappointing. The study team reviewed the process and considered combined problems in project design and staffing, changes of intake workers, and consumer and carer reluctance – a previously identified problem. 10 Enrolment remained low, compromising meaningful quantitative analysis. The success of GPPASA in providing assessment appointments often within days of referral prevented consumer contact prior to that assessment.
A sample size of six to eight is sufficient for qualitative research because it can provide adequate variation and depth 11 but one further qualification pertains to qualitative data: those consumers agreeing to undertake the rather laborious study process are perhaps those for whom the assessment carried more meaning, for instance if seeking a second opinion.
Statistical analysis of quantitative data was limited due to low numbers. The ‘extremely severe’ ratings provided at first assessment, prior to the psychiatrist assessment and management plan, moved to an average of normal/mild, with an improvement in quality of life shown on WHOQoL scales, suggesting that the appropriate target population of people with substantial mental health difficulties may be undertaking Item 291 assessments.
Demographically, at an average age of 46 years, this group were generally well educated with good mental health literacy; at pre-assessment, all accepted that they had mental health problems with some idea of diagnosis. Six of the eight documented mental health problems for more than 5 years, and only two had previously seen a psychiatrist, providing further evidence that Item 291 assessments are reaching an appropriate group.
Thematic analysis showed some consistent themes. The GPs had clearly explained the expectations of one-off assessments so consumers’ expectations were consistent with the intent of Item 291. The consumers had returned to see their GPs by 2 weeks following assessment, GPs had received a management plan, and implementation was proceeding. Consumers were mostly pleased with progress as well as the overall experience of assessment, voicing themes around being listened to and understood – “she was very thorough and very … nice”.
Combining the thematic analysis with the limited quantitative data and pre-assessment questionnaires, this study provides some tentative evidence that not only are Item 291 assessments reaching consumers with substantial mental health difficulties but also that consumers value the assessments and the management plans which follow. While intended to provide the GPs with support, Item 291 assessments must work for the consumer involved. It appears that in this study the goal was being achieved for most of these consumers. Carer involvement in the whole process, both with the psychiatric assessments themselves and the study, was lacking so further comment in this regard can not be made.
This study complements previous research into new Australian initiatives in mental health. Given the prevalence of mental illness, 1,2 and the burden placed on consumers with these conditions and on GPs who are the primary point of contact, successful strategies which help consumers, carers and their treating teams are valuable. 12
More studies with larger numbers examining consumer views and outcomes would be beneficial.
Footnotes
Acknowledgements
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.