
Abstract
Inpatient psychiatric care is required for only a small proportion of adolescents with mental health problems. 1,2 When symptoms are sufficiently severe or increase despite intensive outpatient management, hospitalization may keep the adolescent safe from harm to self or others at times of high risk, improve symptoms and safety by providing a more active treatment environment, and prevent further deterioration of mental disorders by reducing exposure to external stressors. Diagnostic clarification and more comprehensive formulation of complex cases may also be achieved. However, among other potential difficulties, admission may have only a temporary beneficial effect, or may worsen problems for some conditions. 2 Admission may also remove adolescents from strong supports such as school and family. 3
Where possible, inpatient mental health care of adolescents should be provided in specialized child and adolescent units. 4 Nevertheless, for a range of reasons this does not always happen. In England and Wales, over a third of adolescent psychiatry admissions are to adult or paediatric wards rather than adolescent mental health units. 1 Admission of adolescent patients to adult mental health units has attracted criticism. 5 Adolescents may find such admissions traumatic and frightening, and subsequently may be stigmatized by the event. They may find adult patients unpredictable and a source of stress, yet sometimes also supportive. 6 Adolescents cared for in adult units also frequently complain of boredom. 7 A poor quality or harmful inpatient health care experience may lead adolescent patients to develop a lifelong aversion to mental health care. 8 Optimizing inpatient treatment of adolescents is therefore important because it may have long-term benefits in engagement and promoting patients' willingness to access care in future, as well as minimizing the longitudinal impact of mental disorders in this age group.
There is a paucity of data about caring for adolescents in adult inpatient units. 9 There are currently no specialized inpatient adolescent mental health beds in Northern Sydney Central Coast Area Health Service (NSCCHS), New South Wales, Australia. The Area, servicing an estimated 1 124 250 people representing 16.4% of the New South Wales population, 10 split on 1 January 2011 into two local health districts (LHDs). The geographic catchment area spreads north from Sydney Harbour to Lake Macquarie. Adolescent patients are admitted to general adult inpatient psychiatry services, including Psychiatry Emergency Care Centres (PECC units), under the care of adult psychiatrists with consultation from Child and Adolescent Mental Health Services (CAMHS), general medical paediatric wards or to specialized adolescent facilities of other area health services, which are usually a considerable distance from where patients and their families live. We aimed to gather information about the experience, attitudes and knowledge of clinical staff regarding the care of adolescent patients in adult mental health units within the then NSCCHS. The results of this study are intended to be used to inform the improved care of adolescent patients, and support and train clinical staff.
Method
Survey
Following a literature review and consultation with key stakeholders, including staff from adult mental health inpatient units and CAMHS, an initial survey was designed and piloted on a small group of clinicians. Ethics approval was obtained from the NSCCHS Hawkesbury and NSW Institute of Psychiatry Human Research Ethics Committees.
The survey was emailed to all clinical staff (medical, nursing and allied health) with email addresses recorded with their employer and who work in NSCCHS acute adult inpatient units which had admitted adolescent patients in the previous 12 months. These units were located in six hospitals. Three of the hospitals had PECC units which were also included in the survey. “Survey Monkey” software was used to collect responses.
The survey was voluntary and anonymous, with an option for the respondent to state where he/she worked. Consent was indicated by respondents actively clicking on a link in the covering email. During the recruitment period (November 2010 to March 2011), nursing unit managers (NUMs) were requested to email the survey link and covering letter to their nursing and allied staff (214 staff). All psychiatry medical staff employed within NSCCHS (n = 157, comprising 76 consultant psychiatrists and 81 psychiatry registrars) were also emailed the survey. Two reminders were sent to all staff. NSCCHS email lists did not allow researchers to identify the current location or position of medical staff, so psychiatry consultants and registrars working in other subspecialties were also emailed the survey. This allowed the survey to reach doctors who had cared for adolescents in adult wards during overtime shifts, on-call, or in a previous position within the last 12 months.
The survey collected demographic data, including staff level of experience caring for adolescent patients in adult units; “adolescent” was defined as a person aged 13 to 18 years. A vignette describing a14-year-old girl with major depression and a recent suicide attempt was followed by several questions. The survey explored how well equipped staff felt their units were to care for adolescents and whether a separate adolescent unit would be useful. The survey also covered whether there were situations where it was perceived that it may be appropriate to care for adolescents in adult inpatient acute units.
Data analysis
Basic descriptive analyses and a “between groups” analysis with the Kruskal-Wallis test were conducted. Data was analysed using the SPSS-PC Version 17 (SPSS, Chicago, IL, USA).
Open-ended questions were coded. The first author reviewed the qualitative data and created a coding frame. The first and third author then independently coded the responses. Any discrepancies in the coding were discussed and resolved.
RESULTS
Response rate
Surveys were sent out to 372 staff, and 108 responses were received (response rate 29%) (Tables 1 and 2). Eleven respondents did not complete the full survey. Of the 372 surveys 157 were sent to medical staff, of whom 55 replied (response rate 35.0%). It was not possible to identify the response rate from individual hospitals, and hence from allied health and nursing staff. Twenty-two respondents named the facility at which they worked; of these respondents, the greatest maximum number from the same facility was five.
Size (and percentage of the total number) of professional and hospital groups contacted
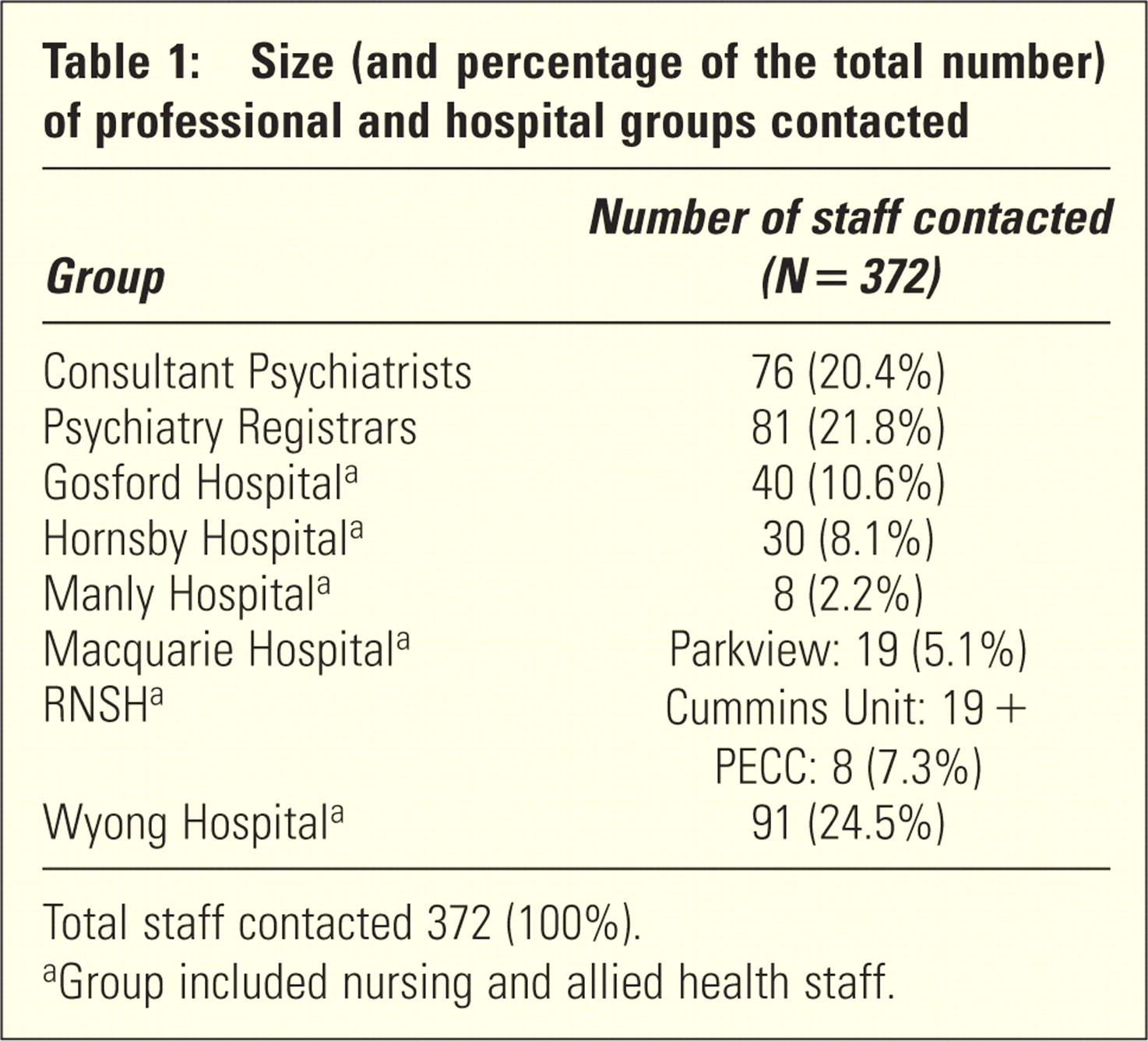
Total staff contacted 372 (100%).
Group included nursing and allied health staff.
Demographic details of respondents
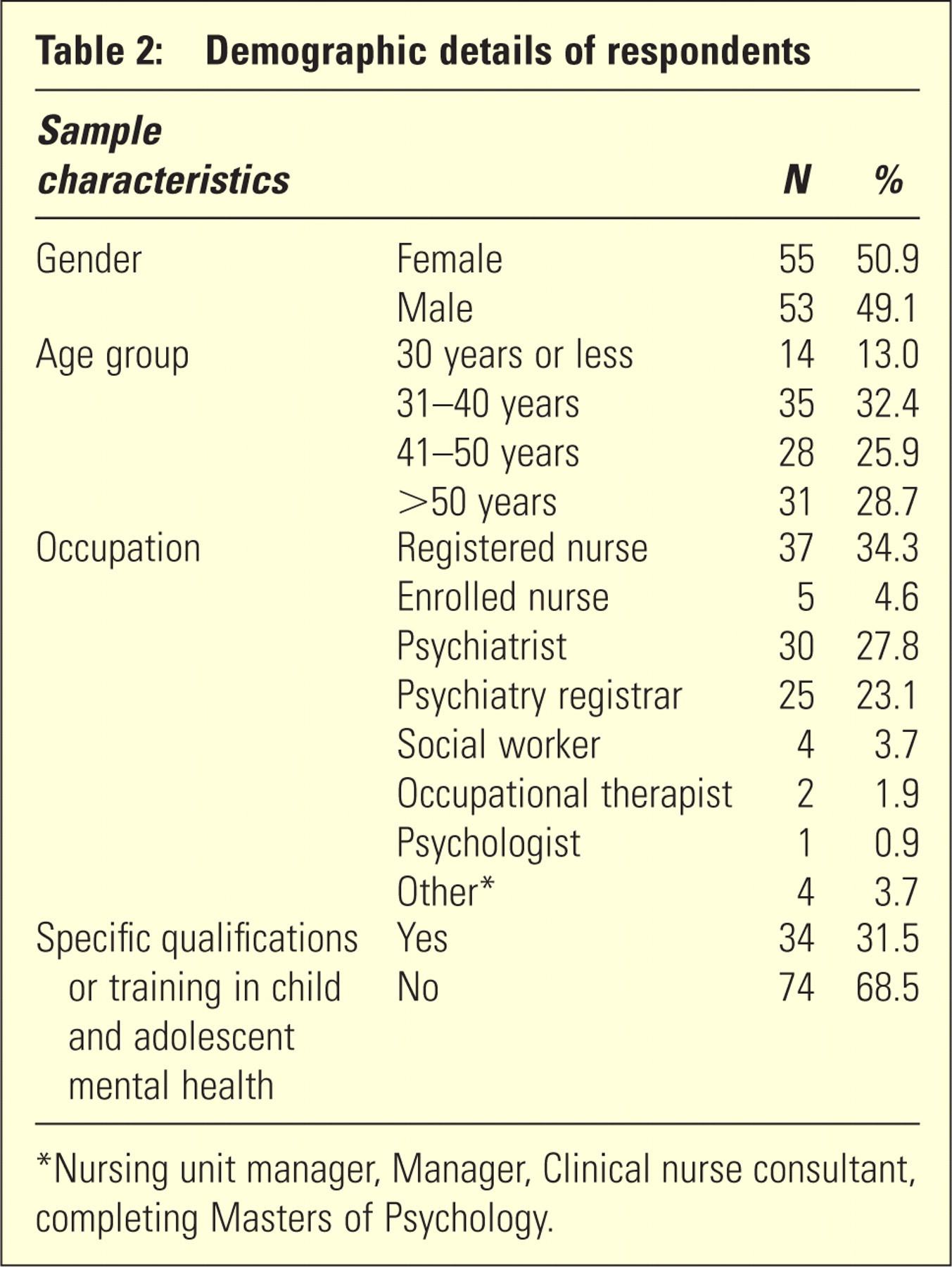
Nursing unit manager, Manager, Clinical nurse consultant, completing Masters of Psychology.
The majority of respondents had personal experience managing adolescent patients in their unit (n = 79, 78.2%) and had cared for more than three adolescents in their unit (n = 63, 62.3%); 17 (16.8%) had not cared for adolescents and 21 (20.8%) had cared for one or two adolescents in their facility. A slight majority of respondents (n = 49, 53.3%) estimated that the average length of stay for adolescents in their facility was less than a week; other estimates were 1–2 weeks (n = 26, 28.3%), 3–4 weeks (n = 11, 12%) and greater than 4 weeks (n = 6, 6.5%).
The majority of respondents believed that their facility was “not at all” (n = 31, 30.7%) or “only a little” (n = 58, 57.4%) equipped to care for adolescents. Ten respondents (9.9%) felt their unit was moderately equipped and two (2%) believed their facility was very well equipped to care for adolescents. The responses to this question from consultant psychiatrists, psychiatry registrars and nursing staff were compared and no statistically significant differences were found (chi-square = 1.37, n = 94, df = 2, p = 0.5).
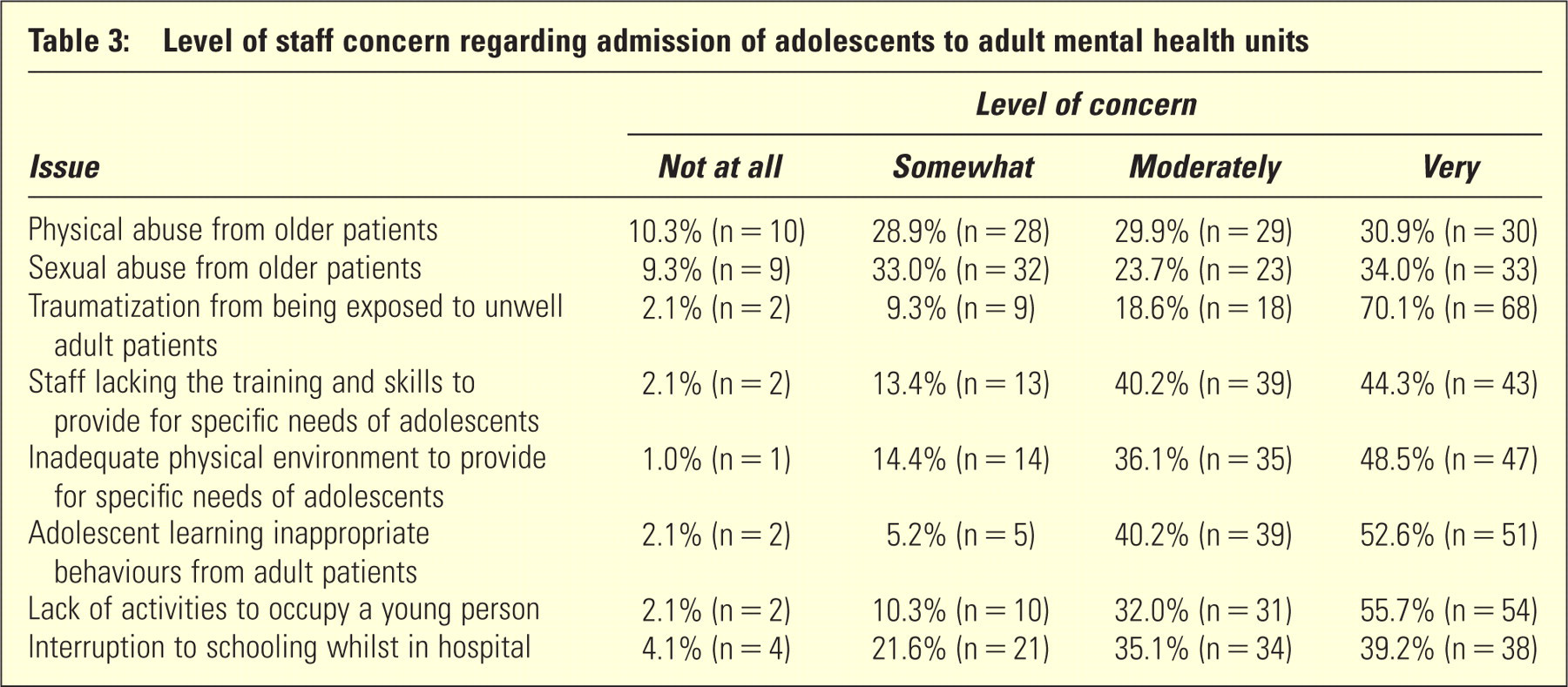
The majority felt “moderately confident” (n = 40, 39.6%), or “very confident” (n = 17, 16.8%) to care for the patient described in the vignette, while 10 respondents (9.9%) felt “not at all confident” and 40 (33.3%) felt only “a little confident” to care for the patient. No statistically significant differences were found on comparing the responses of consultant psychiatrists, psychiatry registrars and nursing staff (chi-square 2.16, n = 90, df 2, p = 0.3). Of the 101 who answered this question, 90 respondents also answered the open question, “What concerns, if any, would you have about this patient being admitted to your facility?” (Table 3). There was a broad range of themes in the answers. The most frequently cited themes were: safety/vulnerability of adolescent patients (n = 48) (this theme included concerns about risk of harm from adult patients, such as violence, sexual assault and vulnerability to exploitation), lack of resources to care for adolescent patients in adult wards (n = 36) (this included the need for greater access to CAMHS and lack of multidisciplinary staff resources), negative impact on adolescents from being with unwell adult patients (including distress from seeing unwell adults and learning maladaptive behaviours from them) (n = 29), adult inpatient units being an unsuitable environment for patients of this age (n = 23), and staff lacking training, skills and confidence to care for adolescent patients (n = 20). Respondents also reported lack of age-appropriate activities in the ward and schooling.
Level of staff concern regarding admission of adolescents to adult mental health units
Another frequently cited theme was concerns related to one-to-one nursing (encompassing comments on one-to-one nursing being counterproductive for adolescents, although necessary for their safety, and staff employed for this task potentially lacking training or English language skills) (n = 12).
Infrequently cited themes included concerns about behaviours including deliberate self harm, impulsivity, regression and acting out (n = 5), the long-term impact of the admission on the adolescent, including future engagement with mental health services (n = 4), different therapeutic approaches of adult compared to adolescent wards (including less emphasis on family therapy) (n = 4), negative impact on staff from these admissions (including increased time demands, dealing with difficult families, staff distress) (n = 4), and finally being in a contained environment may be unhelpful or unnecessary for the adolescent patient (n = 4).
Rarely cited themes pertaining to concerns about admitting adolescents to adult units were lack of peers of a similar age, the admission may be a negative experience for the adolescent, the admission may delay necessary treatments that are not available in adult wards, difficulties with discharge planning, the patient's legal status, adverse drug reactions in adolescent patients who may be medication naïve, distress caused to parents and siblings, and the impact on adult patients.
The majority of respondents believed the objectives of adolescent admissions to their facility were met “only a little” (n = 46, 47.4%) or “not at all” (n = 16, 16.5%). Thirty-three respondents (34.0%) felt the objectives of adolescent admissions were moderately met, and a minority felt the objectives were fully met (n = 2, 2.1%).
More than half the respondents considered that adolescents admitted to their unit received good (n = 46, 47.4%) or excellent (n = 4, 4.1%) quality care. Forty respondents (41.2%) felt the quality of care was barely adequate. Seven respondents (7.2%) felt adolescents did not receive good quality care. The responses from consultant psychiatrists, psychiatry registrars and nurses (including registered and enrolled nurses) to this question were compared and no statistically significant difference was found (chi-square = 3.84, n = 94, df = 2, p = 0.1).
Eighty-one (83.5%) respondents felt a separate child and adolescent a unit would be a “big” improvement to the area health service. Twelve respondents (12.4%) believed it would be a moderate improvement, while a minority (n = 3, 3.1%) felt it would be only a little improvement or no improvement (n = 1, 1%).
Seventy-four respondents believed there are some situations when it is more appropriate to admit adolescents to adult units than adolescent units, even if adolescent beds were available.
A list of possible reasons was given in the survey instrument. The most commonly endorsed reason was “for a young person living a more adult lifestyle (for example, they had left school and were no longer living with parents)” (n = 42). Thirty-eight respondents agreed admission to an adult unit is appropriate “when the adolescent is likely to be aggressive to other patients”, 35 agreed with “for better containment of an acutely unwell adolescent”, 24 endorsed “when the adult facility is geographically closer to the adolescent's family”, and 20 respondents endorsed “when the admission is likely to be very brief”.
Twenty-six respondents cited other reasons, including: in situations where it is necessary for the adolescent's own safety (e.g. when the patient is at high risk of deliberate self-harm) (six respondents), for the safety of other child and adolescent patients (including where the patient is at increased risk of perpetrating sexual assault or violence) (four respondents), and adolescents approaching adulthood with a presentation that is more suited to an adult mental health service model of care (three respondents).
Several respondents stated that adolescents should not be admitted to adult inpatient mental health units or that they should only be admitted when there are no adolescent beds available.
DISCUSSION
To our knowledge, this is the first survey that has explored staff views regarding the admission of adolescent psychiatry patients to adult mental health units. The majority of staff who completed the survey had experience looking after such patients and the concerns that they raised are consistent with those previously identified in the literature. 1,5–8,11 Respondents were generally not in favour of adolescents being managed in adult units apart from in exceptional circumstances. Overall, staff believed that such units were ill equipped to care for adolescent patients, that the objectives of an admission were frequently unmet, and that a specific child and adolescent unit would be preferable.
The survey found that staff harboured concerns about many different aspects of adolescent admissions to adult units, including: safety issues of adolescent patients, the psychological impact on adolescents of being in a ward with many unwell adults (including experiencing distress and learning maladaptive behaviours), and a generally negative impact on the patient, their family, visiting peers, staff and other adult patients. Regardless of the ward to which teenagers are admitted, they are vulnerable due to their age and the circumstances leading to their admission. A frequently expressed concern of staff was that such vulnerability is heightened with admission to an adult ward. Providing adolescent beds (in adult wards) in a designated area, improving access to services and staff in CAMHS and providing age appropriate activities may lessen some of the concerns related to caring for adolescent patients in adult units. The results of this study may maintain momentum for the development of a specialized adolescent psychiatry unit across the two LHDs.
The majority of respondents reported acute adolescent admissions tended to be short (less than a week), which is consistent with the literature. 12 However, a few respondents estimated that the average length of stay for adolescents in their unit was greater than four weeks. Assuming length of stay estimates were reliable, further exploration to identify the reasons for these longer admissions is required to determine whether shorter admissions could be safely achieved or more timely acceptance of referrals be agreed to by existing specialist adolescent units.
It was noteworthy that when the views of the professional groups with the largest number of responses (nursing staff, consultant psychiatrists and psychiatry registrars) were compared – in areas of confidence, perceptions of quality of care for adolescents and how well equipped staff perceived their unit to be in caring for adolescents – no statistically significant differences were found. This “like-mindedness” across professional disciplines supports the robustness of the findings, and perhaps also speaks of the cohesiveness of multidisciplinary staff and their conviction for change.
It was reassuring to note that despite staff concerns about the lack of specialist facilities and skills, the majority of respondents believed that they could confidently care for the adolescent in the vignette and more than half of respondents felt adolescents received good or excellent quality of care in adult units. Nearly a third of respondents had specific training or qualifications in child and adolescent psychiatry. However, a significant proportion of respondents indicated that the lacked confidence and specific training, suggesting a need for strategies to address this. This may involve increased staff training (particularly on topics such as family-based interventions and psychologically based treatments for adolescents), supervision and increased liaison with, and input from CAMHS services.
Despite the concerns raised in this staff survey, NSCCHS receives few complaints regarding the care of adolescents in adult inpatient units and few incidents are reported pertaining to inpatient adolescent care. The use of PECCs for adolescent admissions has been an unexpected service adaptation which appears to have been generally accepted by most interested parties as an acceptable short-term strategy.
A greater understanding of this topic may be achieved if this survey was adapted for the health professionals who refer adolescents for hospital admission, and for the adolescents themselves and their families. If a specialized adolescent unit is opened in the future, it would be valuable to repeat the study to ascertain if and how staff opinions have changed.
Study limitations
The low response rate and absence of an adolescent psychiatry unit in NSCCHS limit the extent to which these results can be generalized to other health services; comparative benchmarking data from other services about rates of admission of adolescents to adult units are lacking. 13 Nevertheless, the absence of an adolescent unit in the area for this population may also suggest that respondents had greater experience caring for adolescent patients under these circumstances and hence increased awareness of the issues surrounding this topic. Because the characteristics of staff who did not complete the survey were not available, the sample who responded may not reflect the characteristics of all clinical staff. Similarly, we were unable to link responses with specific hospital units within the service. It is possible units were variously over- or under-represented in the data obtained and that results may therefore not validly generalize to the whole service. It is possible that staff who were more concerned about the care of adolescents in adult mental health units may have been more motivated to complete the survey. This could have created a sampling bias if the respondents were not representative of all clinical staff.
CONCLUSION
There is a lack of research examining the care of adolescent patients in adult mental health units. To our knowledge, this is the first survey addressing this topic. Generally, staff were not in favour of admitting adolescent patients to adult mental health units, apart from in exceptional circumstances such as for a “young person living a more adult lifestyle” or “when the adolescent is likely to be aggressive to other patients.”
Overall, staff felt these units are ill-equipped to care for adolescent patients, that the objective of these admissions is frequently unmet and that a specific child and adolescent unit would be preferable. Staff harboured concerns about many different aspects of care for adolescents in adult inpatient units. These included concerns about the safety/vulnerability of the adolescent and worries about the impact on the adolescent from being on a ward with many unwell adults.
Although it was reassuring that the majority of staff felt confident to care for adolescent patients, a large number still lacked confidence. Frequently cited concerns included a lack of resources and staff lacking the skills and training to care for adolescent patients in this setting. These concerns could be addressed, at least partly, by providing adolescent beds (in adult wards) in a designated area, providing age-appropriate activities, improved staff training, supervision, increased liaison with/input from CAMHS or a separate specialized adolescent unit.
ACKNOWLEDGEMENTS
The authors thank staff for completing the survey, and Catherine Wiltshire and Stephen Koder for their helpful comments on an early draft of the paper.
DISCLOSURE
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.