
Abstract
Purpose: The purpose of this study was to retrospectively evaluate the clinical and radiographic outcomes of the medium and long-term results of Bionx bioabsorbable screw fixation of the ankle syndesmosis in unstable ankle injuries. Materials and Materials: Between May 2001 and July 2006, 75 patients underwent syndesmotic fixation with a bioabsorbable screw. All patients had closed primary ankle fractures or dislocations with syndesmotic instability. Open reduction and internal fixation of the ankle fracture was performed using current standard orthopaedic technique. Patients were followed clinically and radiographically from 12 to 74 months with the mean being 32.5 months. Results: Seventy of 75 patients (93%) returned for the final evaluation. Mean AOFAS Ankle-Hindfoot score was 90 of 100 and mean VAS for pain was 1.8 out of 10 at the time of final followup. No patients in this population showed radiographic syndesmotic instability, loss of mortise congruency, or post-traumatic arthritis in the sigmoid notch area at final followup. No patients required revision surgical fixation of the syndesmosis. Conclusion: This study demonstrates that the use of bioabsorbable screw for syndesmotic fixation is associated with satisfactory restoration of ankle function and syndesmotic stability.
Introduction
Rotational ankle injuries can often involve the distal tibiofibular syndesmotic ligament complex. Trauma to the syndesmosis ranges from stable sprains to complete disruption with distal tibiofibular diastasis and instability. In turn, syndesmotic instability may present as either a solely ligamentous injury or with an unstable ankle fracture-dislocation. The traditional management of unstable syndesmotic injuries is to stabilize the distal tibiofibular interval with a stainless steel screw. 16 However, this treatment is not without shortcomings. As patients resume weightbearing, the screw is at risk for breakage and can become a source of pain. 1,11,23,30 To avoid this complication, many advocate removal of the syndesmotic screw prior to failure. 38 However, this second surgery is not without its own morbidity and financial cost. In addition, if the screw is removed too early and before there is complete syndesmotic healing, patients can develop recurrent ankle syndesmotic instability. 27
To obviate these shortcomings of steel screws, bioabsorbable fixation of the syndesmosis has been proposed as an alternative. The first kind of absorbable screws used to treat syndesmotic injuries were made of polyglycolic acid (PGA). 13 However, these devices displayed significantly high rates of osteolysis and foreign body reactions due to their rapid rate of hydrolysis. 3,19 To overcome this fault, the absorbable screws are now composed of polylactic acid (PLA) which has a much slower rate of reabsorption and lower incidence of foreign body reaction. 35 While the PLA screws are not as strong as steel screws, their use has distinct advantages in managing syndesmotic injuries. 6,28,33 As screws, they can stabilize the distal tibiofibular joint to allow for ligament healing. As the syndesmosis heals and the PLA screws resorb, stress is transferred from the screws to the ligaments. 6,14 Without the continued immobilization at the syndesmosis that a retained steel screw would provide, patients can regain stable and uninhibited distal tibiofibular motion. 25 There is no need for an additional surgery as the screws are absorbable. Although the PLA screws have weaker mechanical properties than steel, they are sufficient for treating syndesmotic injuries in which patients are initially nonweightbearing. 26
There is limited literature regarding the medium and long-term followup of bioabsorbable syndesmotic screw fixation in unstable ankle injuries. Thordarson et al. treated 17 patients with PLA syndesmotic screws with followup limited to 11 months. 34 Hovis et al. treated 23 patients with PLA syndesmotic screws with a longer mean followup time of 34 months. 14 The two other studies since Hovis et al.'s involve similar population sizes with similar short to medium-term followup. 15,31
The purpose of this study was to evaluate the clinical and radiographic outcomes of the medium and long-term results of bioabsorbable syndesmotic screw fixation in a larger patient population within a single surgeon's (S.M.R.) practice at Thomas Jefferson University Hospital. Our hypothesis was that the bioabsorbable screw fixation for syndesmotic instability reliably allows patients to regain ankle and syndesmotic function and stability.
Materials and Methods
This study was conducted in a retrospective manner. Inclusion criteria included patients with closed primary ankle fractures or dislocations with distal tibio-fibular instability that received surgical treatment from May 2001 through July 2006. These dates were chosen to allow for a minimum of 1-year followup. Exclusion criteria were patients who had preexisting ankle hardware, an open fracture, degloving injuries, pathologic fractures, and Charcot neuroarthropathic fractures. This study was performed with appropriate IRB approval and consent. No funding was obtained from any outside source for this study.
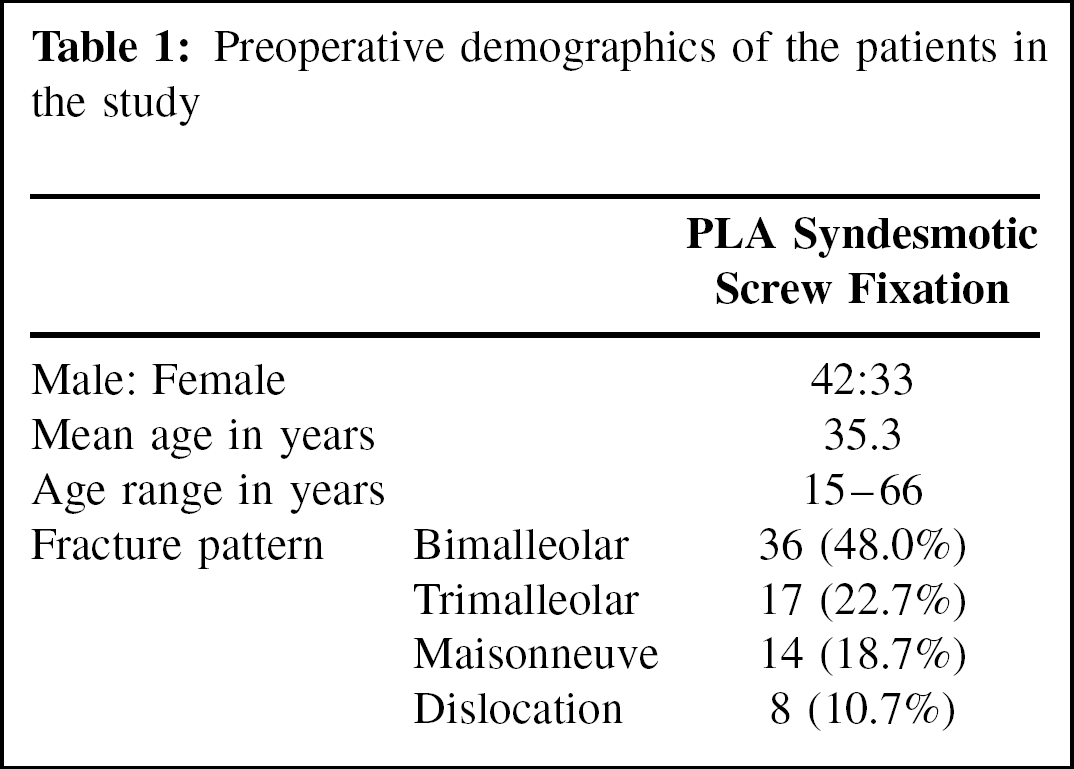
During the period from May 2001 through July 2006, 89 patients underwent fixation of an ankle fracture utilizing bioabsorbable syndesmotic screw fixation. Seventy-five patients satisfied the inclusion criteria of the current study and were invited for further follow up review. All underwent surgery by a single surgeon (S.M.R.) who continues to use bioabsorbable screws for syndesmotic fixation. Forty-two patients were male and 33 were female. The patients were between 15 and 66 years with the mean age being 35.3 years. The right ankle was involved in 32 cases and the left in 43 cases (Table 1). Preoperative diagnoses included 36 patients with bimalleolar ankle fractures, 17 with trimalleolar ankle fractures, 14 with Maisonneuve injuries, and eight with ankle dislocations. The patients in the bimalleolar and Maisonneuve groups included those with either a medial malleolar fracture or deltoid ligament instability. Among those with bimalleolar fractures, six patients had Weber type B and 30 patients had Weber type C fibula fractures on preoperative radiographs. Among those with trimalleolar fractures, 4 patients had Weber type B and 13 patients had Weber type C fibula fractures on preoperative radiographs (Table 1). Seventy of the 75 patients in this study presented for final evaluation with a mean followup time of 32.5 (range, 12 to 74) months. This accounts for 35 patients with bimalleolar ankle fractures, 16 with trimalleolar ankle fractures, 12 with Maisonneuve injuries, and seven with ankle dislocations.
Preoperative demographics of the patients in the study
Patients were invited to return for a final clinical and radiographic evaluation. Clinical syndesmotic stability was assessed with both the squeeze test and the Kleiger maneuver (external rotation stress applied at the ankle with the knee in 90 degrees of flexion). 4,12,20 Postoperative satisfaction and function was scored according to the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot scoring system and pain was assessed by a Visual Analog Scale (VAS). 18 Patients were then asked to rate their outcomes of their procedures as poor, fair, good or excellent. Ankle radiographs were assessed from their preoperative images and final weightbearing studies for mortise congruency and syndesmotic diastasis. Radiographic syndesmotic instability was defined with a tibio-fibular clear space and overlap greater than 5 mm and less than 10 mm respectively at 1 cm proximal to the distal tibia plafond on the anteroposterior (AP) X-ray. 8,29 Observed postoperative complications including need for further revision surgeries were documented.
The Statistical Package for the Social Sciences (version 11.0; SPSS, Chicago, IL) was used for the statistical analysis. ANOVA (analysis of variance) was performed to evaluate the significance of differences in postoperative data among the 4 different types of ankle injuries. A p value of less than 0.05 was defined to be statistically significant.
Surgical procedure
Open reduction and internal fixation of the ankle fracture was performed once the soft tissue swelling had resolved using current standard orthopaedic technique. 5 The bioabsorbable screw used for this study was the Bionx (Bionx, Blue Bell, PA) 4.5-mm Smart Screw which is made of PLA (Figure 1). The syndesmosis was tested for stability intraoperatively prior to screw placement in all cases. For patients with bimalleolar and trimalleolar ankle fractures, a Cotton test was performed after fracture fixation to check for syndesmotic stability. 32 In those with Maisonneuve injuries that involved a medial malleolar fracture, the syndesmosis was tested intraoperatively with an external rotation stress following fracture fixation. 2,4 If the syndesmosis displayed intraoperative instability, it was held reduced with a large bone tenaculum compressing the distal tibio-fibular joint. With the ankle in neutral dorsiflexion, the bioabsorbable screw was placed across the syndesmosis. When plate fixation was utilized, one syndesmotic screw was used (Figure 2). Two screws were used for the Maisonneuve fractures when no plate fixation was required. Four cortices of fixation was obtained whenever possible, with the distal screw placed 2 cm proximal to the tibial plafond. Approximately one-third to one-half of the screw head is usually removed using a hot cautery to debulk the large head size.

The PLA Bionx 4.5-mm Smart Screw used in this study.

In this patient, the PLA screw is placed through a hole in the fibular plate. The drill hole for the syndesmotic screw is tapped before screw insertion.
Postoperative regimen
After surgery, patients were prohibited from weightbearing on their affected ankle for 6 weeks. At 6 weeks, patients were allowed to progressively bear weight in increments of 50% of body weight in their fracture boots every 3 weeks. They were also allowed to begin active and passive range-of-motion (ROM) exercises of their ankle at this time. At 12 weeks after surgery, patients were allowed to wean out of their fracture boots and increase their level of activity as tolerated.
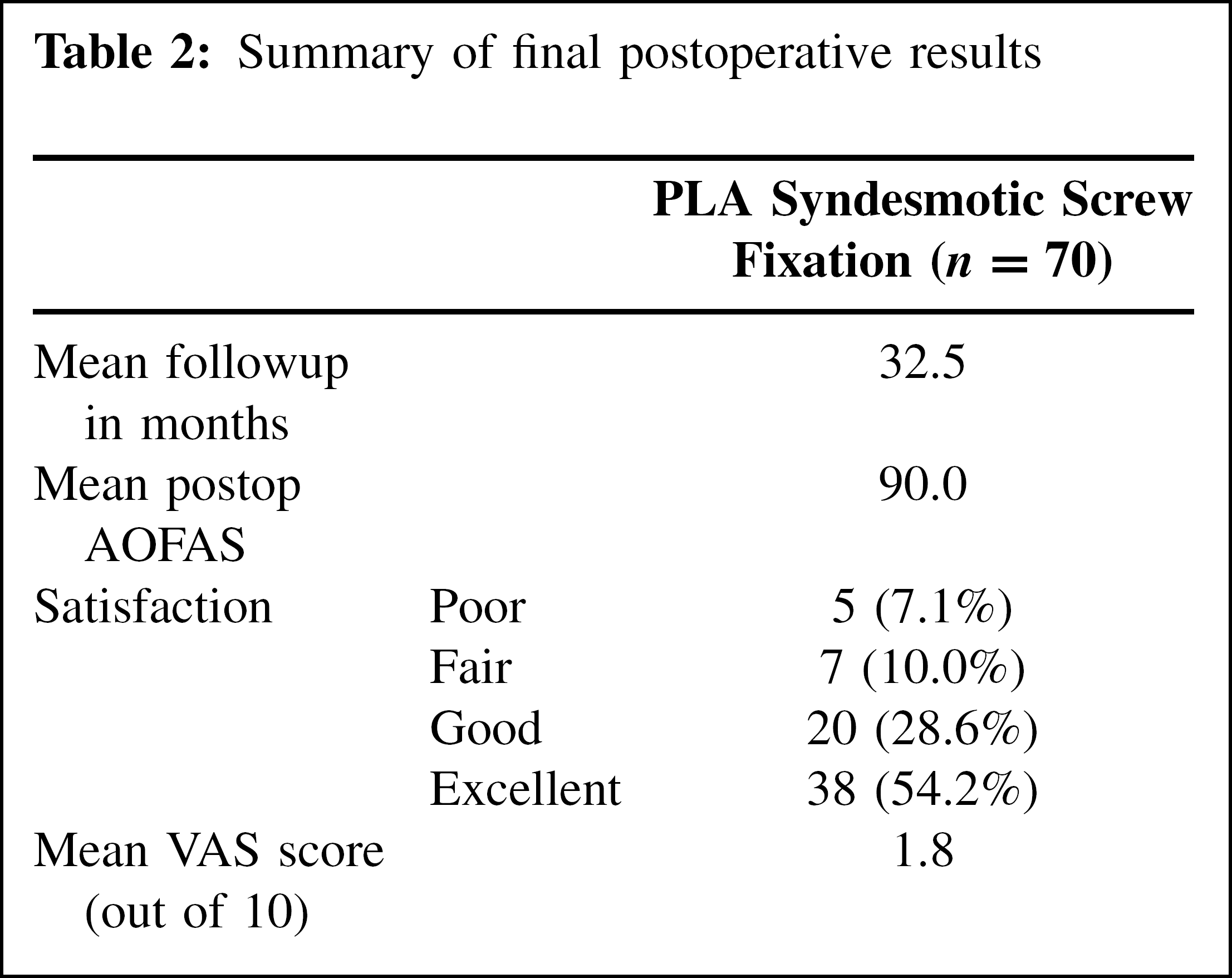
Summary of final postoperative results
Results
Clinical stress testing of the syndesmosis did not reveal any instability or pain in 66 of 70 patients (94%). Four patients (6%) had mild pain on syndesmotic stress, but no clinical instability. No patients showed radiographic syndesmotic instability, loss of mortise congruency, or post-traumatic arthritis in the sigmoid notch area at final followup.
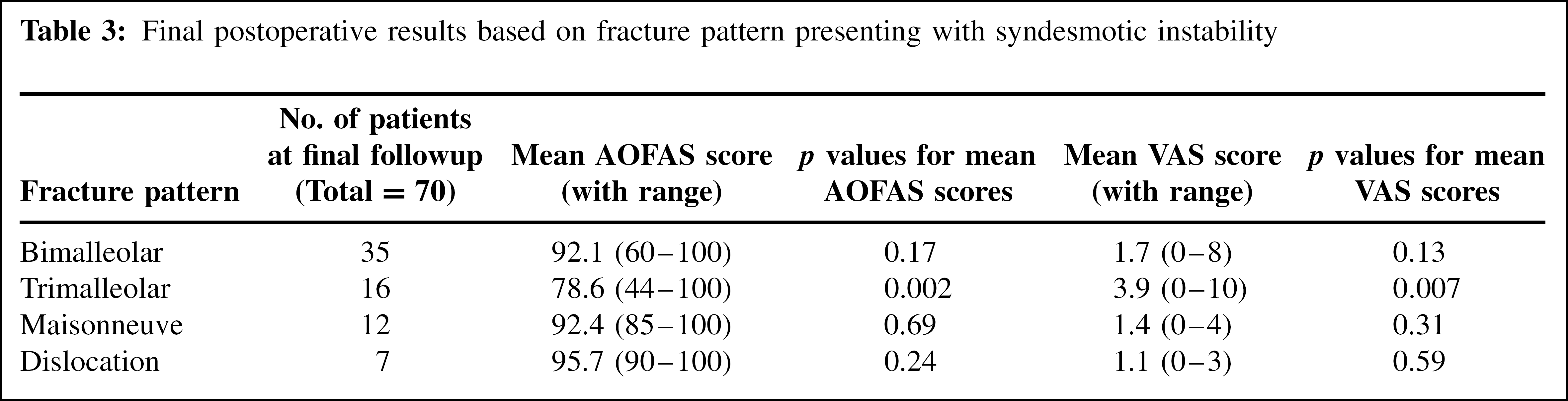
AOFAS and VAS scores were assessed for all patients at the time of final followup. For the entire population, the mean AOFAS Ankle-Hindfoot score was 90 of 100 (range, 44 to 100) and VAS was 1.8 out of 10 (range, 0 to 10) (Table 2). 38 patients (54.2%) rated their outcome as excellent, 20 as good (28.6%), 7 as fair (10%), and 5 as poor (7.1%) (Table 2). The mean AOFAS scores for the patients with bimalleolar ankle fractures, trimalleolar ankle fractures, Maisonneuve injuries, and ankle dislocations were 92.1, 78.6, 92.4, and 95.7, respectively. The mean VAS scores for those with bimalleolar ankle fractures, trimalleolar ankle fractures, Maisonneuve injuries, and ankle dislocations were 1.7, 3.9, 1.4, and 1.1 respectively. When the mean AOFAS and VAS scores of all 4 groups were compared, the trimalleolar ankle fracture group exhibited differences that are statistically significant (p < 0.05). The p values for the difference in mean AOFAS and VAS scores between the trimalleolar fracture group and the other 3 groups were 0.002 and 0.007, respectively (Table 3).
Two of the 70 patients (2.9%) developed irritation at the head of the screw which had not fully resorbed. These two were treated with removal of the screw head remnant under local anesthesia at 8 and 11 months, respectively, without complications. No patients required revision surgical fixation of the syndesmosis. No wound complications or sterile abscess formation were seen in our study population.
Final postoperative results based on fracture pattern presenting with syndesmotic instability

Preoperative (A) and final postoperative (B) radiographs at 36 months of a trimalleolar ankle fracture with syndesmotic instability. Note that while the tract for the bioabsorbable syndesmotic screw remains visible, the patient's medial and tibiofibular clear space is reduced.
Discussion
The treatment of distal tibiofibular syndesmotic instability remains surgical and usually involves screw compression of the distal tibiofibular interval. Traditionally, this has been performed with a stainless steel screw. However, using a steel screw to stabilize the syndesmosis has its faults. As patients resume weightbearing, the steel screw has been shown to interfere with normal motion at the distal tibiofibular joint. 23 When subject to enough stress, the screw can break. 1,11,23,30 Some have argued that retained steel syndesmotic screws cause minimal problems even in the event of mechanical failure. 22 Others have reported instances of pain following steel syndesmotic screw breakage. 1,30 To avoid the likelihood of steel syndesmotic screw failure and subsequent pain, many have traditionally advocated routine screw removal. 17,38 However, this requires an additional surgery which is not without its own risks. In addition, if the screw is removed before there is complete ligament healing, patients can develop recurrent instability. 27
In the past several years, different types of implants have been proposed as an alternative to achieve syndesmotic fixation. Some authors have used a syndesmotic staple with success rates comparable to steel screws. 9,37 Missbach-Kroll et al. described using two 1.6-mm Kirschner wires to stabilize the syndesmosis with 81% of patients having good results at final followup. 21 Others have begun to study flexible suture constructs such as the Arthrex Tightrope (Arthrex, Naples, FL) to fix the syndesmosis. In a comparative study using cadavers, Forsythe et al. found specimens with the Tightrope to exhibit significantly greater syndesmotic diastasis upon external rotation than those with steel screws. 10 Cotton et al. used the Tightrope to stabilize the syndesmosis in 25 patients with unstable ankle injuries and recently published good clinical and radiographic results within the first year of followup. 7 Certainly, these newer devices require further study with longer patient followup.
While bioabsorbable PLA syndesmotic screws have been used for several years, they have been examined in only a few studies. In a randomized, controlled, and prospective study, Thordarson et al. compared PLA to steel syndesmotic screw fixation in 32 patients with PER ankle fractures. 34 They reported no significant difference in outcome between patient populations. However, the study population was limited to one type of injury mechanism and followup was less than 1 year. In a prospective and non-comparative study, Hovis et al. treated 23 patients with PLA syndesmotic screws. 14 All patients had either good or excellent results at a longer mean followup time of 34 months. However, their PLA population size was similar to that of Thordarson et al.'s. Sinisaari et al. compared PLA to steel syndesmotic screw fixation in 30 patients in a retrospective study. 31 While they report good outcomes with the use of PLA screws, their followup ranged between 12 and 23 months from surgery. More recently, Kaukonen et al. compared PLA to steel syndesmotic screw fixation in a randomized, prospective, and blinded study involving 40 patients. 15 This paper detailed longer patient followup ranging from 17 to 51 months after surgery. However, patients'outcomes were not evaluated with the use of a scoring system. Rather, both groups of patients were compared using final ankle plantarflexion-dorsiflexion range of motion, swelling, and radiographic syndesmotic stability. In fact, none of the previously mentioned literature used a VAS to assess patients'postoperative pain.
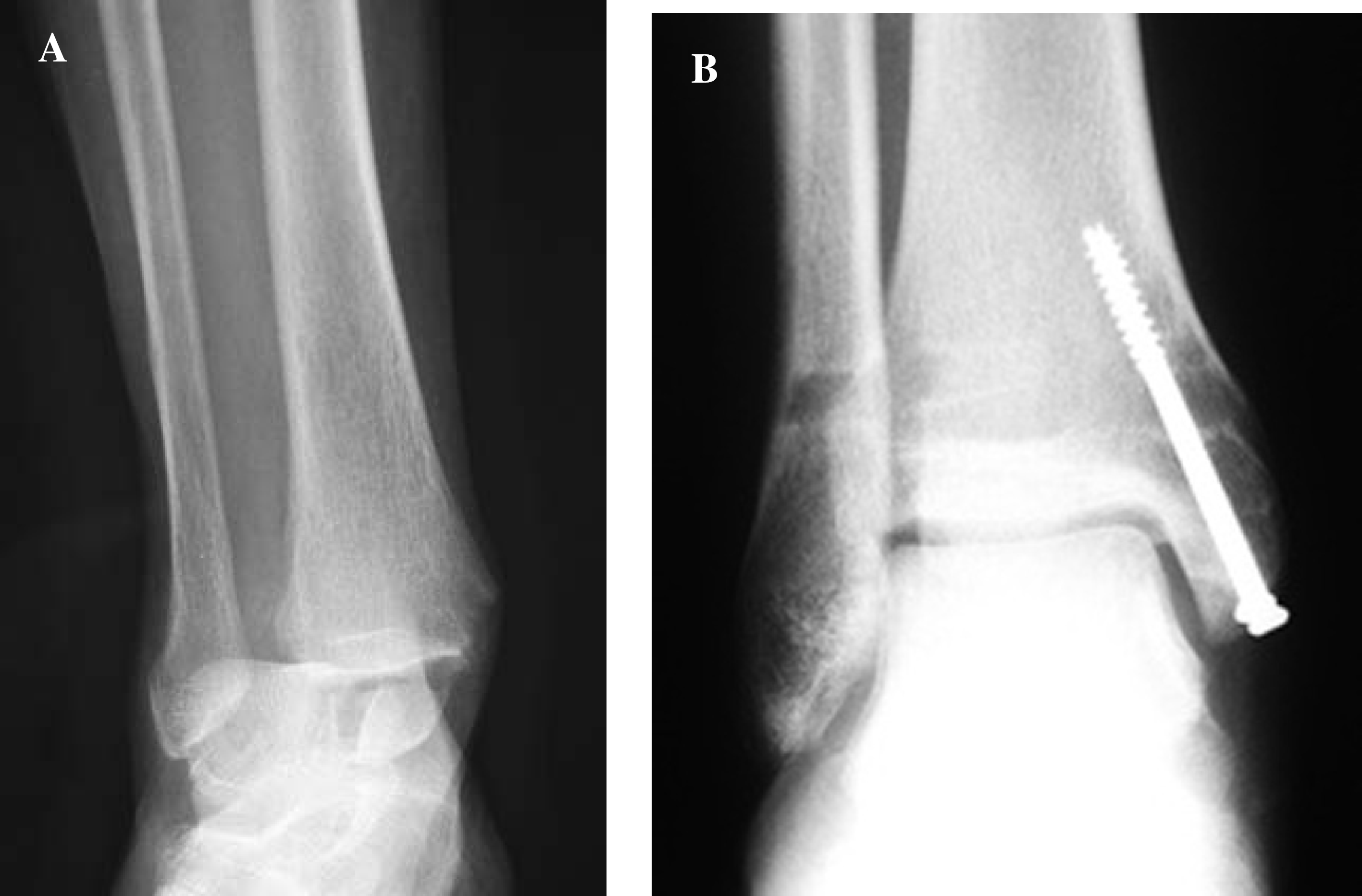
Preoperative (A) and final postoperative (B) radiographs at 42 months of a study patient with a Maisonneuve injury. Following medial malleolar fixation, this patient still had intraoperative syndesmotic instability which necessitated fixation. Note that while the tract for the bioabsorbable syndesmotic screw remains visible, the patient's medial and tibiofibular clear space is reduced.
Our study, while retrospective and non-comparative, details results in patients with a variety of unstable ankle injuries with syndesmotic instability. We demonstrated that using bioabsorbable PLA screws to achieve syndesmotic fixation was predictable in providing ankle and syndesmotic function and stability. None of our patients displayed clinical or radiographic syndesmotic instability. Furthermore, all radiographs of our patients showed neither loss of mortise congruency nor post-traumatic arthritis in the sigmoid notch area at final followup. This is identical to the results in earlier mentioned studies with smaller patient populations and shorter patient followup. 14,15,31,34
In contrast to prior studies regarding bioabsorbable syndesmotic screw fixation, we used AOFAS and VAS scores to assess patient outcomes. An earlier study used the Olerud-Molander (OMA) scoring system to assess patients at final followup. 24 Both the OMA and AOFAS scoring system include points for pain, activities of daily life, and motion. However, the remaining points in the OMA system are accounted for by swelling, use of supports, ability to climb stairs, run, jump, and squat. The other points in the AOFAS Ankle-Hindfoot scoring system involve walking distance, walking surfaces, gait abnormalities, stability, and alignment. There are no studies to date that compare the OMA and AOFAS scoring systems as outcomes measures. The mean postoperative AOFAS and VAS scores in our study population are 90 and 1.8, respectively. These values are consistent with the improved pain, function, and stability seen among our patients.
In contrast to earlier studies, the size of our study population allowed for some comparisons between patients with different fracture patterns. When AOFAS and VAS scores were assessed based on the type of injury, we found that those with bimalleolar fracture, Maisonneuve, and ankle dislocations had comparable averages. However, those with trimalleolar ankle fractures displayed significantly lower mean AOFAS and VAS scores with p values of 0.002 and 0.007, respectively, when compared to the rest of the study population. As none of the patients displayed postoperative syndesmotic instability or loss of mortise congruency, this discrepancy seems to arise from the difference in fracture pattern rather than the syndesmotic injury. It has been widely published that many trimalleolar ankle fractures are higher-energy injuries with a greater potential for chondral damage than other types of rotational ankle fractures. 36 This would explain the difference in AOFAS and VAS scores between our study patients with trimalleolar fractures and those with other injuries.
Our study does have some inherent limitations due to its length of followup and population size. As the range of followup is from 12 to 74 months, final AOFAS and VAS scores for some patients may change in the longer term. While our entire study population was larger than in other studies, its size was divided into four types of fracture patterns. Comparing patients to each other based on the type of injury was restricted as the population of each subset was limited and unequal. While it takes time to achieve a larger study population with larger and more equal distributions of population subsets, this may be of benefit for future research.
Conclusion
This study demonstrated that the use of bioabsorbable screws for syndesmotic fixation was associated with satisfactory restoration of ankle function and syndesmotic stability. PLA screws were advantageous in this setting as they were absorbable. Initially, they provided enough distal tibiofibular stability to allow for syndesmotic healing. As the ligaments healed, the screw resorbed without need for surgical removal.