
Abstract
Impaired glucose metabolism is implicated in cardiac failure during ischemia-reperfusion. This study examined cardiac glucose uptake and expression of glucose transport-4 (GLUT-4) in dogs undergoing ischemia-reperfusion. Cardiac ischemia was induced by cardiopulmonary bypass for 30 min or 120 min in dogs. Plasma insulin and glucose concentrations were measured at pre-bypass (control), and aortic cross-clamp off (ischemia-reperfusion) at 15, 45, and 75 min. At the same time, the left ventricle biopsies were taken for GLUT-4 immunohistochemistry and glycogen content analysis. In dogs receiving 120-min ischemia, coronary arterial and venous glucose concentrations were increased, but the net glucose uptake in ischemia-reperfusion heart were significantly decreased from 25% (control) to zero at 15 and 45 min of reperfusion, and recovered to only 7% after 75 min reperfusion. Myocardium glycogen contents were decreased by 65%. Plasma insulin levels and Insulin Resistant Index were markedly increased in dogs undergoing 120-min ischemia and reperfusion. These changes were relatively mild and reversible in dogs receiving only 30-min ischemia followed by reperfusion. Expression of total GLUT-4 in myocardium was decreased 40% and translocation of GLUT-4 from cytoplasm to surface membrane was decreased 90% in dogs receiving 120-min ischemia followed by 15-min reperfusion. Suppressed translocation of GLUT-4 was also evident in dogs receiving 30-min ischemia, but to a lesser extent. Reduced myocardium glucose uptake, utilization, and glycogen content are clearly associated with ischemia-reperfusion heart injury. This appears to be due, at least in part, to suppressed expression and translocation of myocardium GLUT-4.
Introduction
Cardiopulmonary bypass has been used over 50 years for heart surgery, and has undergone considerable improvement since its application (1–3). Despite many years of clinical and experimental research, the contribution of cardiopulmonary bypass and cardioplegic arrest to mortality after cardiac surgery remains unclear (4–5). Myocardial ischemia-reperfusion injury, secondary to aortic cross-clamping, is an undesired outcome influenced by many risk factors and various molecular mechanisms (5). The molecular mechanisms for ischemia-reperfusion heart injury include the generation of free radicals, increase in intracellular calcium, dysregulation of nitric oxide pathways, inability of energy production, dysregulation of ATP-sensitive potassium channels and aberrant signal transduction. These mechanisms could act together to produce myocardial infarction, cardiac arrhythmias, and contractile dysfunction (4–6). Among many cardiovascular risk factors, diabetes and insulin resistance are definitely contributing factors for myocardial ischemia-reperfusion injury (5–6).
The decline of aerobic glucose metabolism on reperfusion of ischemic myocardium is one of the main causes contributing to cardiac dysfunction (7). Myocardial glucose utilization dysfunction directly leads to cardiac energy production impairment, cardiac dysfunction, and even cardiac failure (5–8). Emerging evidence indicates that changes in cardiac energy metabolism may contribute to the development of contractile dysfunction. Myocardial mitochondrial dysfunction during metabolic syndrome could lead to oxidative stress, calcium overload, and activation of uncoupling proteins (5, 9).
Insulin resistance is an important factor to trigger the metabolic syndrome leading to the impairment of glucose uptake and utilization (6, 8, 10). Insulin resistance is associated with the severity of chronic cardiac failure (5–6), but may also contribute to decline in glucose utilization after cardiopulmonary bypass or cardiac ischemia-reperfusion (11), and to the abnormal energy metabolism. Impaired cardiac glucose metabolism can contribute to increased ischemia-reperfusion heart damage in chronically infracted rat heart (12). Glucose transport-4 (GLUT-4), an insulin-regulated glucose transport in the heart (13), translocates to myocyte membranes to increase glucose transport in response to various stimuli (14–15). During cardiac ischemia-reperfusion, impaired translocation of GLUT-4 is associated with decreased glucose uptake in animals (15–16). Recent studies suggest that impaired insulin-signaling in ischemic hearts contributes to inability of GLUT-4 translocation to myocyte membranes (17), leading to abnormalities in myocardium glucose uptake and utilization in response to ischemia.
The aim of the present study is therefore to examine the involvement of insulin resistance and the expression of GLUT-4 during ischemia-reperfusion injury in dogs undergoing cardiopulmonary bypass. The results clearly demonstrate that prolonged cardiac ischemia-reperfusion decreased myocardium glucose uptake and utilization, and these effects are possibly related to insulin resistance with decreased GLUT-4 expression and translocation to myocyte surface membranes.
Materials and Methods
Experimental Animals.
Healthy mongrel dogs, weighing 12.8 ± 2.26 kg, were randomly assigned to two groups irrespective of gender. Group 1 (n = 6) received aortic cross-clamping for 30 mins and Group 2 (n = 6) received aortic cross-clamping for 120 mins. Animals were provided from Experimental Animal Surgery Department of Zunyi Medical College. All research was conducted in compliance with the Animal Welfare Act and the Guide for the Care and Use of Laboratory Animals. Surgery was performed in designated veterinary surgical suites using sterile instruments and procedures.
Experimental Procedures.
The animals were fasted overnight and anesthetized with an intraperitoneal injection of sodium pentobarbital (25 mg/kg), and underwent endotracheal intubation to maintain mechanical ventilation (VT 12–15 ml/kg, 15 times/min) throughout the experiment. Electrocardiogram (ECG) was continuously monitored during operation. Mean arterial pressure (MAP) was monitored through a left femoral artery catheter and a transfusion tube was established through the left femoral vein. Blood gases and pH were also measured to ensure preparation stability. Immediately after opening the thorax through a central incision, heparin (3 mg/kg) was injected into the right atrium catheter and cardiopulmonary bypass was established. St. Thomas cardioplegic solution at 4°C was infused for 1 time (10 ml/kg) in Group 1 and 4 times in 30 min intervals in Group 2. Artificial plasma containing Hydroxyethy Starch and isotonic sodium chloride was prefilled into the Cardiopulmonary Bypass Unit for maintaining MAP at a constant 60–80 mmHg (80 ml/kg/min). By using “U-type” mattress suture, the blood flow of coronary sinus was determined at pre-bypass, aortic cross-clamp off at 15, 45, and 75 mins, respectively. Blood samples (6 ml) were taken simultaneously from coronary artery and coronary sinus for glucose and insulin analysis, and the biopsy samples from the apex of the left ventricle (about 8 mm3 size) were taken for GLUT-4 and glycogen analysis.
Biochemical Assays.
Plasma glucose levels were determined immediately with OLYMPUS AU-2700 Biochemistry Analysis Automatics. In order to exclude the influence from blood dilution, blood glucose values were normalized with hematocrit (Hct) with the formula: pre-bypass Hct/sample Hct (18).
For plasma insulin determination, plasma was stored at −20°C prior to determination with Radio-Immunity Assay (RIA) using the RIA Kits from Beijing North Institute of Biological Technology (Tian-Jin, China) in gamma scintillation counter (USTC Co. Ltd, Zonkia, China). Insulin resistance was calculated as Insulin Sensitivity Index using the homeostasis model assessment (HOMA) formula: fasting plasma glucose (mmol/l) × fasting serum insulin (μU/ml)/22.5 (19).
A portion of biopsy heart sample was used for cardiac glycogen content determination, and expressed as mg/g dry heart weight.
Immunohistochemistry.
Heart biopsy samples were fixed in 10% buffered formalin, and embedded in paraffin blocks by standard histology procedures. Tissue blocks were de-paraffinized in xylene and hydrated in a series of graded alcohol solutions, and endogenous peroxidase was blocked with 5% hydrogen peroxide. The sections were then incubated with Polyclonal antibody against GLUT-4 (1:100 Santa Cruz Biotechnology, California, USA) at 4°C overnight, followed by incubation with goat anti-rabbit IgG conjugated with horseradish peroxidase (1:200). The signals were visualized by ABC Immunostain Systems (Santa Cruz Biotechnology, CA). Each sample was blindly examined in three slides with three visual fields in each slide with Olympus microscope (Japan). To quantify the immunostain intensity, visual images were analyzed with the Hyper HAD Mias-2000 Visual Analyzing Automatic System (Leica Ltd, Germany). The optical density (OD) value of the myocardial immunostain was corrected with the background OD value to obtain the corrected OD value (OCD) for comparison.
Statistics.
Data represent mean ± SEM. The PSS12.0 software was used for statistical analysis. For comparisons between two groups, Student’s t test was used. For comparisons among three or more groups, data were analyzed using a one-way analysis of variance, followed by Duncan’s multiple range tests. For cardiac immunostain, Games-Howell test was used. The level of significance was set at P < 0.05 in all cases.
Results
Decreased Glucose Uptake and Utilization in Ischemia/Reperfusion Heart.
Cardiopulmonary bypass followed by reperfusion resulted in marked increase in plasma glucose concentration in both coronary artery and venous blood (Fig. 1). Plasma glucose concentrations were increased 5.5-fold after 120-min aortic cross-clamp. The shorter time aortic cross-clamp (30-min) also results in elevations (2-fold) in glucose concentrations in coronary artery (arterial glucose), but to a much lesser extent (Fig. 1A). However, the glucose concentrations in venous blood (venous glucose) were also elevated to the levels similar to the concentrations detected from arterial blood (Fig 1B). If one calculates myocardium uptake and utilization based on the formula (% of glucose utilization = (arterial glucose – venous glucose)/venous glucose), the net glucose uptake/utilization in 120-min ischemia animals was decreased from 25% to zero at 15 and 45 mins after reperfusion, and only recovered to 7% at 75 mins of reperfusion (Fig. 1C). 30-min ischemia also reduced glucose utilization from 20% to zero at 15 mins after reperfusion, and slowly recovered to 11% at 75 mins of reperfusion. With sharp decline in glucose uptake and utilization, aerobic glucose metabolism via consumption of cardiac glycogen occurred, resulting in myocardium glycogen content decrease from 11 mg/g dry heart to less than 4 mg/g after 120-min aortic clamp (Fig. 1D).
Increased Plasma Insulin Levels and Insulin Resistant Index.
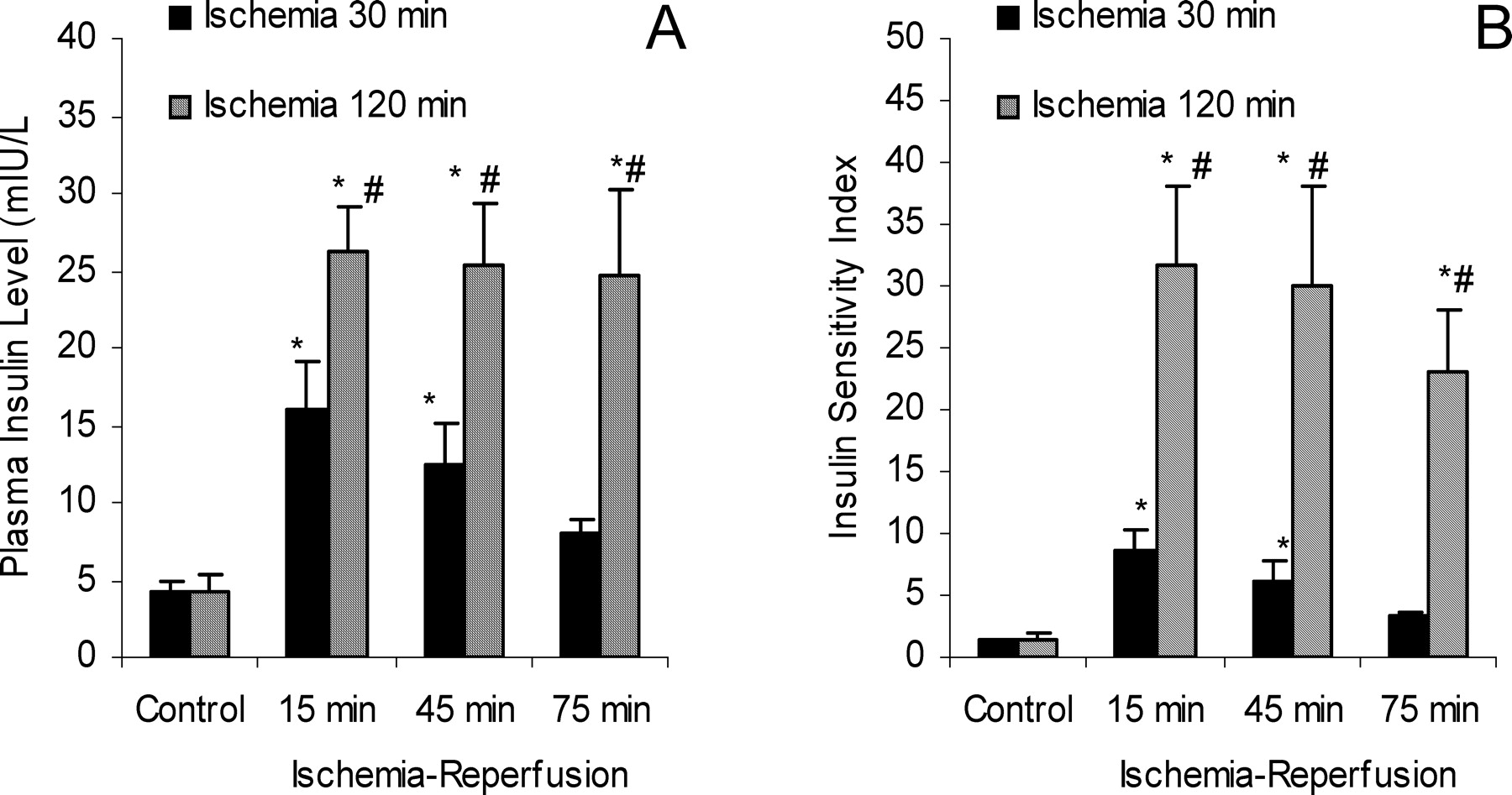
To compensate the decreased myocardium glucose uptake and utilization, plasma insulin levels were markedly increased over 5-fold after 120-min aortic cross-clamp, or 3-fold after 30-min aortic cross-clamp off at 15 mins reperfusion (Fig 2A). For the dogs that received a 120-min aortic cross-clamp, the plasma insulin levels remain elevated throughout the 75 mins reperfusion; while for dogs that received a shorter 30-min ischemia, the plasma insulin levels were slowly returned to control levels (Fig. 3A). Despite the elevations of plasma insulin levels, the glucose uptake and utilization in myocytes remained very low (Fig. 1C), and if the Insulin Sensitivity Index formula (19) is used for comparison, such differences are even greater, reaching to 25 folds in 120-min ischemia, and 7 folds in 30-min ischemia, respectively (Fig. 2B).
Suppressed Expression and Translocation of Glucose Transport-4.
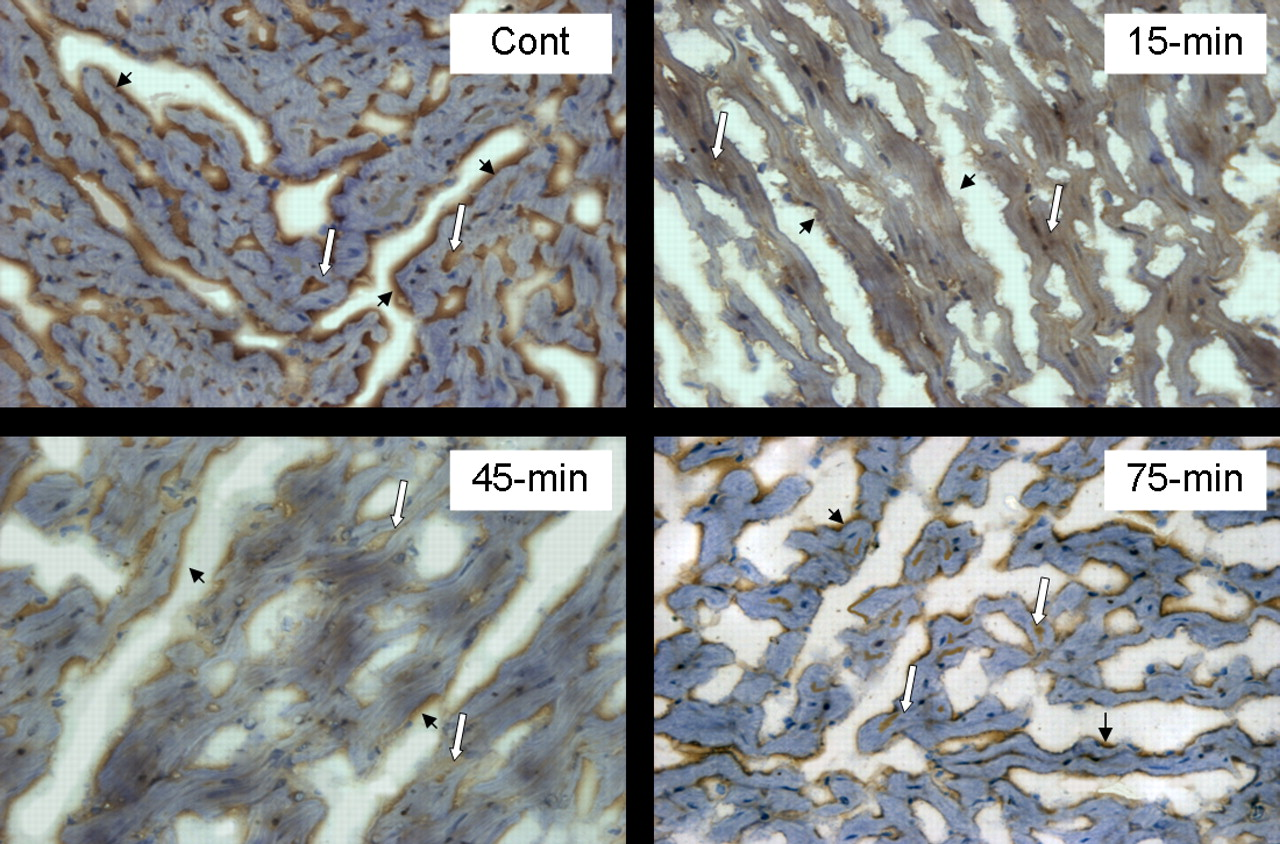
To further examine the molecular mechanisms for insulin resistance associated with ischemia-reperfusion cardiac injury, the expression of GLUT-4 in the heart was examined by immunohistology (Fig. 3) and the intensity of the immunostain was semi-quantified with Hyper HAD Mias-2000 Image Analysis System (Fig. 4). The positive stain for GLUT-4 appears to be yellow to dark brown depending on the extent of expression (Fig. 3). The GLUT-4 mainly located in cytoplasm (80–90%), with less than 20% located on myocyte surface membrane as compared to prior to ischemia-reperfusion (Cont). At 15 mins and 45 mins after aortic cross-clamp off, the percentage of GLUT-4 located in surface membrane was dramatically decreased, and the expression of GLUT-4 in cytoplasma was also decreased (15-min and 45-min). At 75-min reperfusion, the expression of GLUT-4 was slightly increased, but still much less than what was seen at control levels (75-min).
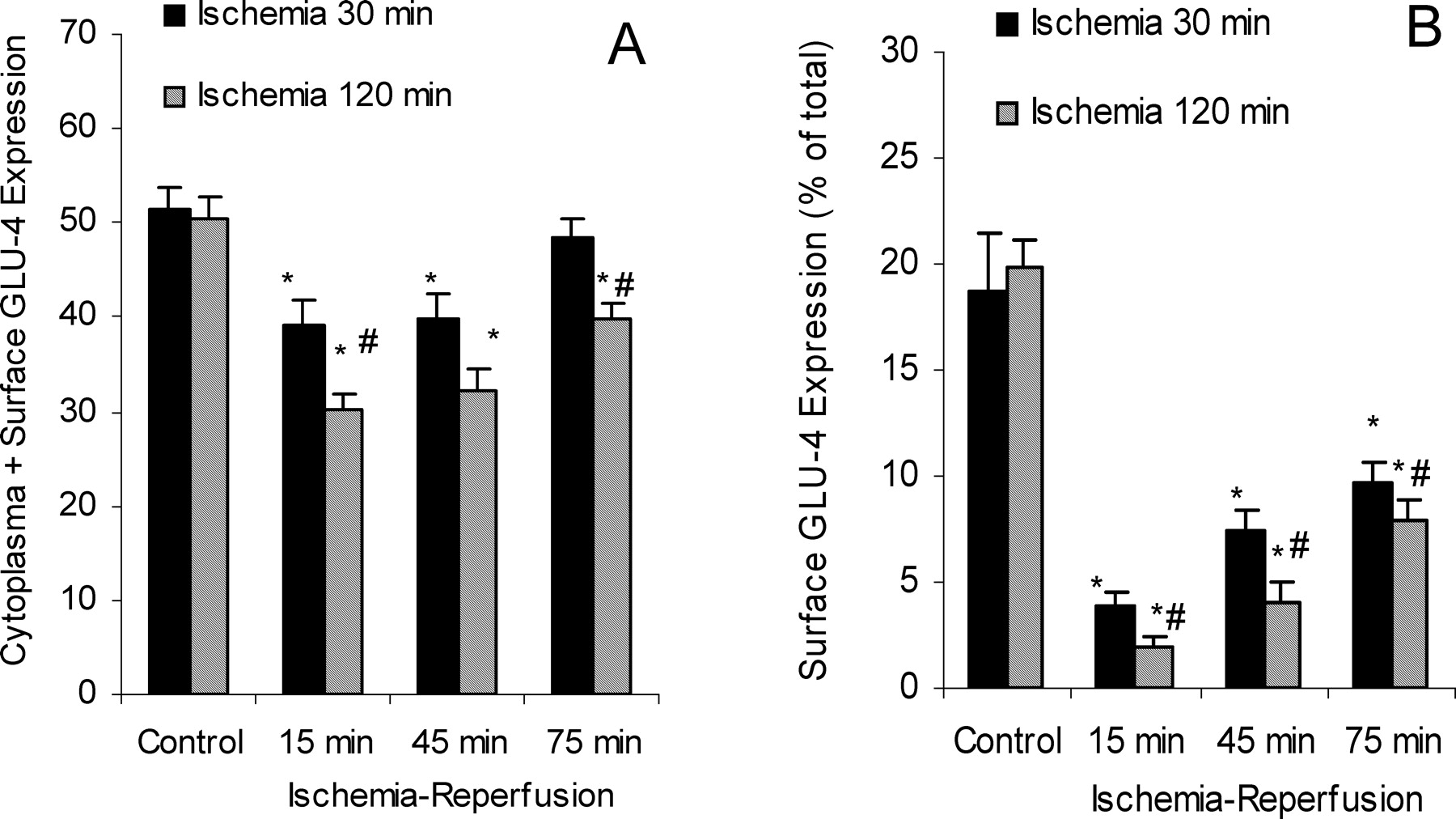
Myocardial GLUT-4 expression in myocyte cytoplasma surface membranes was semi-quantified and results are shown in Figure 4. The Total corrected optical density (COD) for GLUT-4 in cytoplasma and myocyte surface was around 50 in controls. After 120-min aortic cross-clamp off at 15 mins, it was about 30, a 40% decrease; and it remained low at 45- and at 75-min of reperfusion, it was still 20% lower than controls. In contrast, after 30-min aortic cross-clamp off, the COD was only 20% lower than control, and returned to normal at 75 mins of reperfusion (Fig 4A). When the percentage for GLUT-4 in myocyte surface membrane is considered, marked decreases were even more evident in an ischemic time-dependent fashion (Fig. 4B). The translocation of GLUT-4 from myocyte cytoplasma to surface membrane was dramatically decreased from 20% to 2% in 120-min ischemic animals, which was gradually recovered to 8% at 75 mins after reperfusion. Similar pattern for decreased GLUT-4 translocation was also evident in 30-min ischemic animals, but to a lesser extent, and at 75 mins of reperfusion, it was still half of the control value.
Discussion
The present study clearly demonstrates that glucose uptake and utilization are decreased after cardiopulmonary bypass and reperfusion in dogs, and the longer the ischemic period the more pronounced reduction in glucose uptake occurred. To compensate for decreased glucose uptake into ischemic heart, plasma insulin levels are increased in an attempt to increase the uptake of glucose, as heart energy production is dependent on aerobic glucose metabolism in ischemic heart (5–8). Impaired glucose uptake due to “insulin resistance” in ischemic heart leads to consumption of cardiac glycogen, and once glycogen is completely depleted, cardiac failure occurs. The present study also demonstrates the expression and translocation of GLUT-4, an insulin-regulated glucose transporter in the heart, were significantly suppressed following ischemia. These findings are novel in that the association of impaired glucose uptake with aberrant expression of GLUT-4 in dog undergoing cardiopulmonary bypass (ischemia) has been clearly demonstrated.
The decline in glucose uptake and utilization directly leads to impairment of cardiac energy production (7–8, 20). Insufficient energy production not only impairs cardiac contractile function, but also contributes to inability of myocardium to cope with ischemia/reperfusion stress (9, 21). The generation of oxygen free radicals and influx of calcium are well-known consequences of ischemia-reperfusion, which can be further exaggerated by insufficient energy production due to decline in glucose uptake and utilization (5, 9). Impaired glucose uptake and utilization could result in mitochondrial dysfunction and dysregulation of ATP-sensitive potassium channels with aberrant signal transduction in the heart, causing cardiac dysfunction (5, 7, 21), therapeutic strategies to improve glucose uptake and utilization may benefit the ischemic heart, and could have an additive benefit to existing therapeutic strategies (22).
To compensate the decline of myocyte uptake of glucose, insulin secretion is greatly enhanced. However, in the present study, increased plasma insulin failed to restore glucose uptake and utilization to the control levels. One explanation is the “insulin resistance phenomenon” occurring during ischemia-reperfusion cardiac injury (5, 6, 10). Insulin resistance, in turn, renders myocytes insensitive to insulin stimuli to increase glucose uptake. Insulin resistance can also abolish myocardial preconditioning against ischemia-reperfusion heart injury (5, 23), probably mediated through mitochondrial dysfunction and enhanced oxidative stress. Pioglitazone, a thiazolidinedione, can increase glucose uptake in the periphery tissues and can decrease the risk of certain cardiovascular diseases (24); whether such drugs can be used to increase myocardium sensitivity to insulin and to enhance glucose uptake during ischemia-reperfusion is worthy of further investigation.
Myocardial ischemia switches cardiac energy metabolism from oxidation of fatty acids and glucose to anaerobic glucose metabolism (5–8, 10), and thus cardiac glucose uptake is important (15–17, 24–27). Both GLUT-4 and GLUT-1 have been shown to play important roles in ischemia-mediated myocardial glucose uptake in canine or rat heart (25–26), and impaired insulin signaling in hypertrophied hearts restricts insulin-mediated GLUT-4 translocation during ischemia, contributing to ischemia cardiac injury (17). Indeed, suppressed GLUT-4 translocation to myocyte membranes during ischemia-reperfusion has been reported in rats (12, 15, 26), diabetic mice (16), rabbits (17) and dogs (26, 27). GLUT-4 translocation in ischemic dog can also be reduced by exogenous nitric oxide such as nitroglycerin and 8-Br-cGMP, but the nitric oxide synthesis inhibitor L-nitro-argininemethylester does not affect GLUT-4 translocation while stimulating glucose oxidation (27). Expression of GLUT-4 is tissue-specific and is regulated by hormones and many metabolic factors (13). To elucidate the regulation of GLUT-4 during ischemia-reperfusion cardiac injury may help solve the problem of its depressed expression and translocation and the resultant reduction of glucose utilization.
In summary, this present study in Mongrel dogs demonstrated that cardiac ischemia from cardiopulmonary bypass followed by reperfusion decreased uptake of glucose and produced the depletion of cardiac glycogen. The decreased glucose utilization appears to be due, at least in part, to decreased GLU-4 expression and translocation to myocyte surface membranes. Thus, the depressed GLUT-4 translocation during cardiac ischemia could trigger decreased glucose uptake, contributing to ischemic heart injury.
Decreased cardiac glucose uptake during ischemia-reperfusion. Mongrel dogs were anesthetized, and cardiac ischemia was produced by aortic cross-clamping for 30 mins or 120 mins, respectively, followed by reperfusion at 15, 45, and 75 mins. Plasma glucose concentrations from coronary artery blood (A) and from coronary venous blood (B) were determined. The net glucose uptake and utilization (C) was calculated based on arterial and venous blood glucose concentrations. Cardiac glycogen content was determined with biopsy samples from the left ventricle. Data are mean ± SEM (n = 6); *significantly different from corresponding controls, P < 0.05; #significantly different from 30-mins ischemia group, P < 0.05. Plasma insulin levels and Insulin Resistance Index during ischemia-reperfusion. Mongrel dogs were anesthetized, and cardiac ischemia was produced by aortic cross-clamping for 30 mins or 120 mins, respectively, followed by reperfusion at 15, 45, and 75 mins. Plasma insulin concentrations were determined by the RIA assay (A), and the Insulin Resistant Index (B) was calculated by the formula described in the Methods. Data are mean ± SEM (n = 6); *significantly different from corresponding controls, P < 0.05; #significantly different from 30-min ischemia group, P < 0.05. The representative photographs of GLUT-4 immunostain during ischemia-reperfusion in dogs. The biopsy samples were taken from the left ventricle before ischemia (Cont), and aortic cross-clamping off at 15, 45, and 75 mins. The GLUT-4 in myocardium was stained yellow to dark brown. White long arrows indicate the GLUT-4 location in the myocardium cytoplasma, and black short arrows indicated the GLUT-4 translocation to surface membrane of myocytes. Magnitude: ×400. A color version of this figure is available in the online journal. Semi-quantitation of GLUT-4 expression in the canine heart during ischemia-reperfusion. The biopsy samples from the left ventricle were taken before 120 min of ischemia and at 15, 45, and 75 mins after removing the aortic cross clamp. The immunostain was quantified with Mais 2000 Automatic Analyzer. Data are mean ± SEM (n = 6); *significantly different from corresponding controls, P < 0.05; #significantly different from 30-min ischemia group, P < 0.05.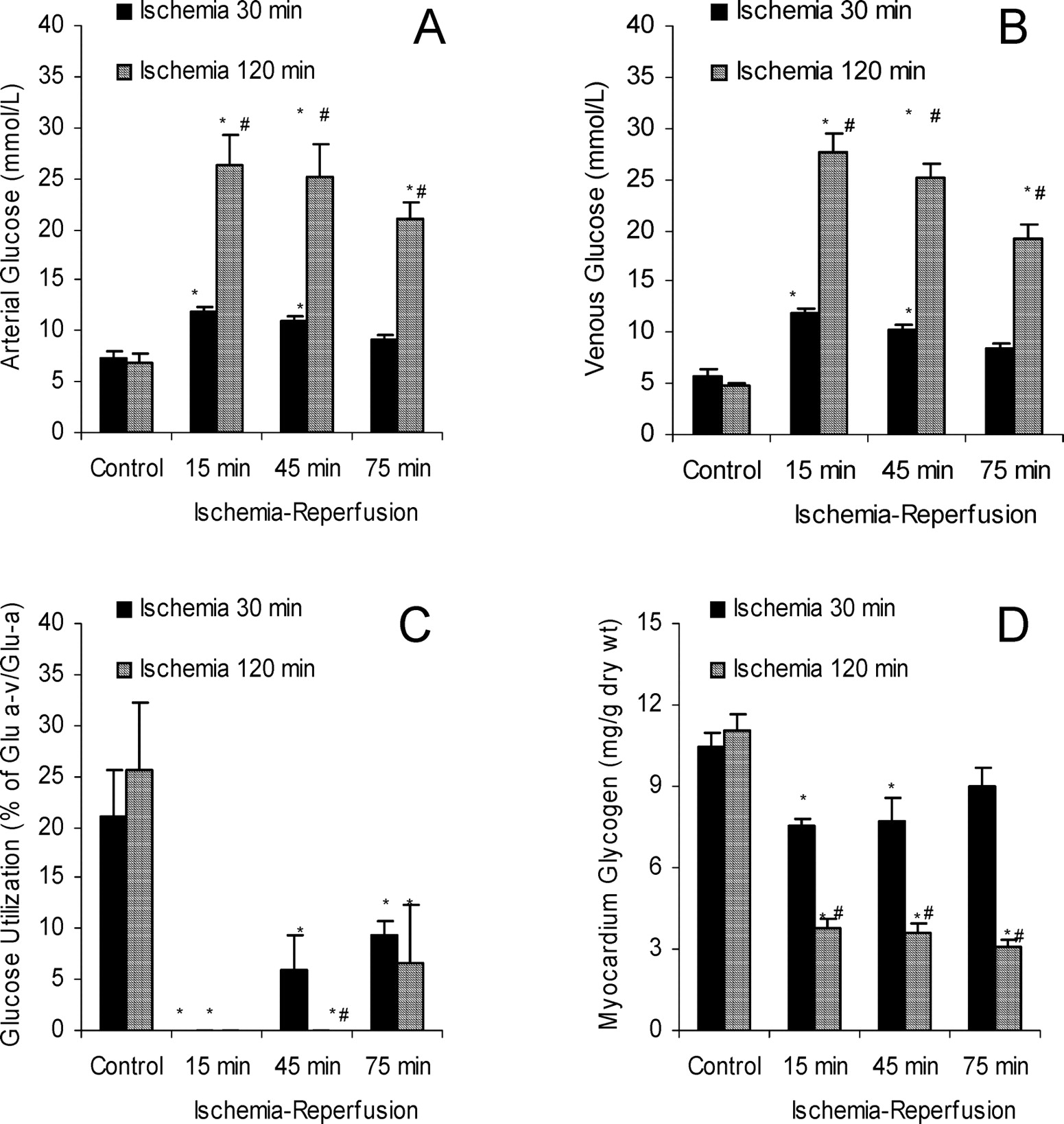
Footnotes
This work was supported by Guizhou Governor Funds #2003-04-02 and Guizhou Key Research Program Fund #2007–1032.