
Abstract
It has been shown that after ischemia-reperfusion, application of hyperbaric oxygen (HBO) reduces cardiac injury. In this study we tested the hypothesis that HBO preconditioning reduces injury to the ischemic myocardium. One hundred and eight adult male Sprague-Dawley rats (250–280 g) were randomly divided into four groups: normoxia + sham surgery (CS), normoxia + permanent occlusion of the left anterior descending (LAD) coronary artery (CMI), HBO preconditioning + sham surgery (HS), and HBO preconditioning + permanent LAD occlusion (HMI). Rats receiving HBO preconditioning were intermittently exposed to 100% O2 at 2.5 atmosphere absolute (ATA) for 60 min, twice daily for 2 days followed by 12 hrs of recovery in room air prior to the myocardial ischemic insult induced by LAD ligation. Rats in the normoxia group were time-matched with the HBO group and maintained under normoxic conditions prior to LAD occlusion. At 3 and 7 days after LAD occlusion, heart function parameters were measured by inserting a catheter into the left ventricle, infarct size was calculated using the method of TTC staining, myocardial capillary density was determined by immunohistochemical staining with a monoclonal anti-CD31/PECAM-1 antibody, and VEGF protein level was determined by Western blot analysis. At 3 days after LAD ligation, the infarct size of the HMI group was significantly smaller than that of the CMI group (26 ± 2.5% vs. 38 ± 3%, P < 0.05). The heart function parameters including left ventricular systolic pressure (LVSP), +dP/dtmax and −dP/dtmax were significantly improved in the HMI group compared to the CMI group at 3 and 7 days after LAD occlusion. Capillary density and VEGF protein levels were significantly increased in the ischemic myocardium pre-exposed to HBO. We conclude that HBO preconditioning alleviates myocardial ischemia in rat model.
Introduction
Hyperbaric oxygenation (HBO) therapy is a potent means to increase the oxygen content of blood by intermittently exposing the entire body to 100% O2 at a pressure greater than 1 atm (101.325 kPa). HBO is used as a primary therapy in patients with carbon monoxide poisoning, decompression sickness, arterial gas embolism, and as an adjunctive therapy for the treatment of various diseases accompanied by impaired oxygen delivery, including wound healing and ischemic injury (1–3). Although HBO can potentially introduce oxidative stress, it is considered to be safe when used according to established protocols, with oxygen pressure not exceeding 3.0 atm and a duration limited to a maximum of 2 hrs (4).
Myocardial infarction is one of the leading causes of death in many countries throughout the world. Myocardial ischemia may occur as a result of increased myocardial metabolic demand and/or decreased delivery of oxygen and nutrients to the myocardium via the coronary circulation. Effective treatments for myocardial infarction are still lacking. Several laboratory studies have shown protective effects of post HBO treatment on myocardial ischemia-reperfusion (3–7). Several clinical studies also indicated cardiac benefits of HBO therapy, including preventing atrial fibrillation paroxysms, reducing anginal attacks, relieving dyspnea, and lowering cholesterol levels (7). The present study tested an HBO preconditioning protocol, which effectively reduced infarct size and improved heart function after myocardial infarction in a rat model.
Materials and Methods
Animals and Groups.
Adult male Sprague-Dawley rats weighing 250–280 g were used in all experiments. The rats were housed in individual cages in a temperature-controlled room with a 12 hr light/dark cycle and were given free access to food and distilled water. The total number of animals used for this study was 108, and they were randomly divided into four groups: normoxia + sham surgery (CS), normoxia + permanent occlusion of the left anterior descending (LAD) coronary artery (CMI), HBO pretreatment + sham surgery (HS), HBO pretreatment + permanent LAD occlusion (HMI). Each group has 27 rats. The animal numbers used for experiments are described in the figures.
All procedures were approved by the Second Military Medical University in Shanghai, China and were in accordance with the Guide for Care and Use of Laboratory Animals published by the US NIH (publication No. 96-01).
HBO Preconditioning.
Rats were exposed to 100% O2 at 2.5 ATA for 1 hr, twice daily for two consecutive days, the interval of HBO exposure was 12 hrs. Compression and decompression of HBO were carried out at the rate of 0.2 atm/min. The gas in the chamber was continuously ventilated to prevent the retention of CO2, and the temperature in the chamber was maintained within the range of 22°C–25°C. After the exposure to HBO, the rats were maintained in a normoxic environment for 12 hrs until the operation of myocardial infarction or the sham operation. Rats under normobaric room air served as control.
Production of Acute Myocardial Infarction.
Rats were intraperitoneally anesthetized with chloral hydrate (350 mg/kg). The rats were intubated and ventilated with a small-animal ventilator. The left chest was opened through the fourth intercostal space. The pericardium was opened, and a 5.0 prolene suture was tightened around the proximal left anterior descending (LAD) coronary artery (before the first branch of diagonal artery). Positive end-expiratory pressure was applied to fully inflate the lungs. The muscle layer and the skin were closed separately and the animals were allowed to recover.
Hemodynamic Measurement.
Three and seven days after the operative intervention, the rats were anesthetized. A small incision was made to the right of the midline in the neck. The right carotid artery was identified and a PE 50 catheter was introduced into the artery. The proximal end of the catheter was connected to a low pressure transducer. The inserted tip of this catheter was advanced down until it reached the left ventricular lumen and the left ventricular pressure (LVP) signal was obtained. The pressure signals were monitored, analyzed and recorded in real time. Heart rate (HR), LV systolic pressure (LVSP), and ±dP/dtmax were all calculated from the continuously obtained LVP signal.
Infarct Size Determination.
Three days after myocardial infarction, infarct size and area at risk were measured. Two milliliters of 1% Evan’s blue dye was infused into the heart through the apex to mark the risk zone as unstained (not blue) tissue. Frozen hearts were then cut into 2 mm thick slices parallel to the atrioventricular groove. Sections were thawed and incubated in a 1% tetrazolium chloride (TTC; Sigma) phosphate buffered solution (pH 7.4) at 37°C for 15 min and fixed in 10% formalin to increase the contrast of the Evan’s blue and TTC staining. Tissue sections were compressed to a uniform 2 mm thickness by placing them between two glass plates separated by 2 mm space. The viable tissue was stained red with TTC, while the dead tissue (infarcted tissue) was unstained. The volumes of the infarct area and the risk area in each of the sections were calculated by an image analysis system Image J, a public domain image analysis program developed by the National Institutes of Health, USA. The infarct size was calculated as a percentage volume of the infarct area (white area) versus the risk area (non-blue area).
Histological and Immunohistochemical Examination.
Rats were sacrificed after 3 and 7 days of LAD occlusion. The hearts were fixed with formalin and embedded in paraffin. Four-micrometer transections were cut from the paraffin blocks. The standard deparaffinization protocol was used. To evaluate capillary density in the border zone of the left ventricles, the immunohistochemical staining was performed by the avidin-biotin complex method using a monoclonal anti-CD31/PECAM-1 antibody (Santa Cruz Biotechnological Co., Santa Cruz, CA), as described previously (8). The antibody binding was visualized using an ABC Kit (Vector Laboratories). Five fields per section were randomly selected and analyzed at a magnification of ×400. The number of capillaries was counted from photomicrographs and the density per mm2 was calculated.
Western Blot Analysis for VEGF.
Total cell lysate for VEGF analysis was obtained from the border zone of the left ventricles, using a nuclear extraction kit (Active Motif) and following the manufacturer protocol. Equal amounts of the samples containing 40 μg proteins were loaded per lane, separated on 12% dodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE) and transferred electrophoretically to nitrocellulose membranes. Membranes were blocked with 2% BSA in Tris-buffered saline containing 0.1% Tween20 (TBST) at room temperature for 1 hr and then incubated overnight at 4°C with anti-VEGF antibody (Santa Cruz Biotechnology), and β-actin antibody (Sigma) diluted 1:1000 in 2% BSA in TBST. Horseradish peroxidase-conjugated anti-rabbit IgG (Santa Cruz Biotechnology) was used as the secondary antibody (1:2000 dilution in 2% BSA in TBST, 1 hr incubation) and the antigen antibody complexes were visualized using an enhanced chemiluminescence reagent (Pierce Biotechnology, Inc., IL, USA). The amount of VEGF was quantitated by densitometry scanning using a densitometer (GS-700; Bio-Rad Laboratories, Inc., CA, USA), analyzed with Quantity One 4.5.2 software (Bio-Rad Laboratories, Inc., CA, USA) and normalized to β-actin, an internal standard.
Statistical Analysis.
All results were expressed as means ± SEM. Differences between groups were determined with a one-way ANOVA followed by a Student-Newman-Keuls test. A value of P < 0.05 was considered to denote statistical significance.
Results
Hemodynamic Measurement.
The heart function parameters including LVSP, +dP/dtmax and −dP/dtmax were comparable between the CS and the HS groups. However, significant reduction of LVSP, +dP/dtmax and −dP/dtmax was observed after CMI after 3 and 7 days of LAD-occlusion (Fig. 1). HBO preconditioning prevented the reduction of the LVSP, +dP/dtmax and −dP/dtmax in the HMI group, though they were significantly lower than those in the CS/ HS group. No statistical difference was found for heart rate between all the groups after 3 and 7 days of LAD occlusion (data not shown).
Infarct Size.
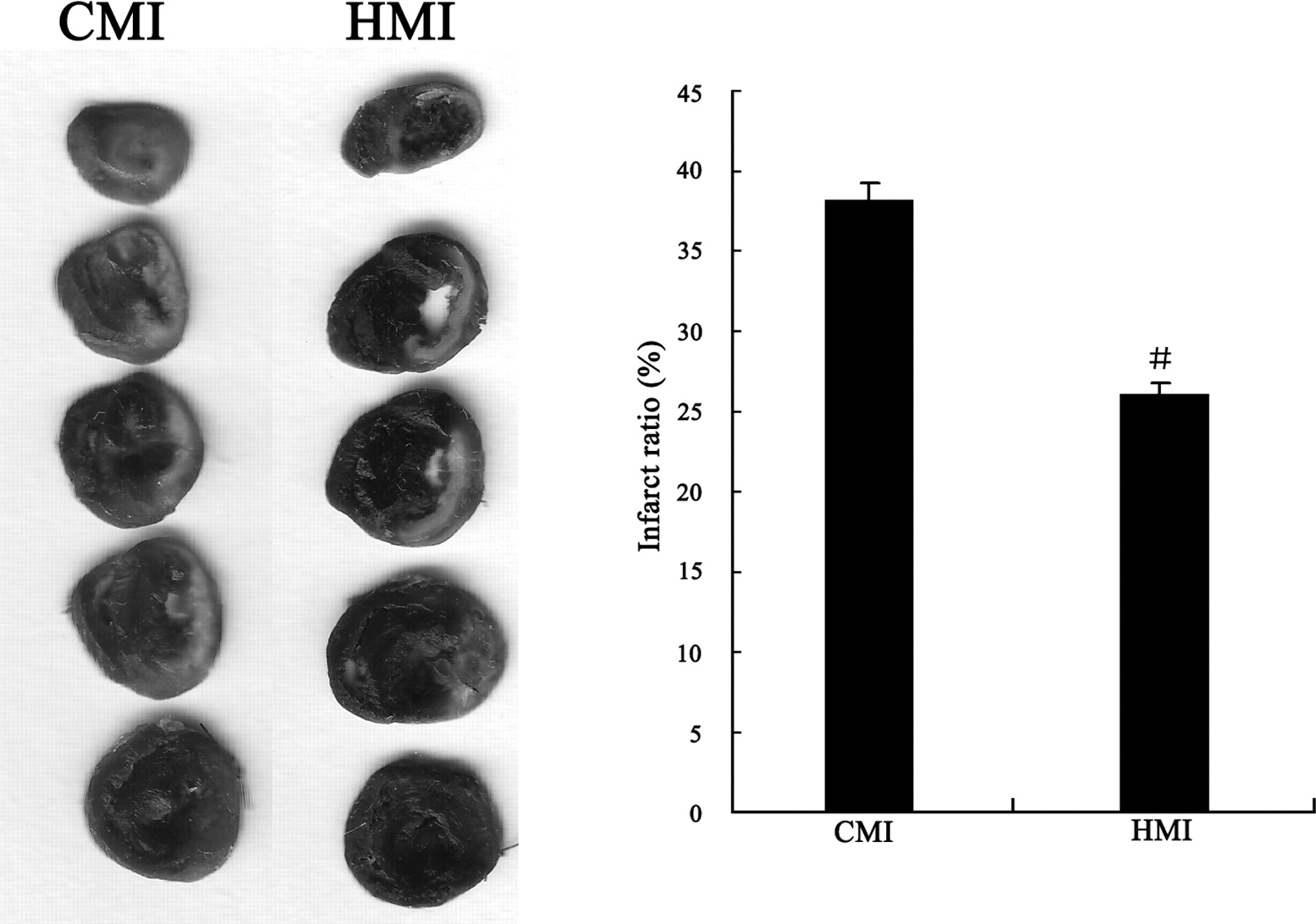
The infarct size was measured in 9 CMI hearts and 9 HMI hearts after 3 days of LAD occlusion. The infarct size of the HMI group was significantly smaller than that of the CMI group (26 ± 2.5% vs. 38 ± 3%, P < 0.05), as shown in Figure 2.
Capillary Density.
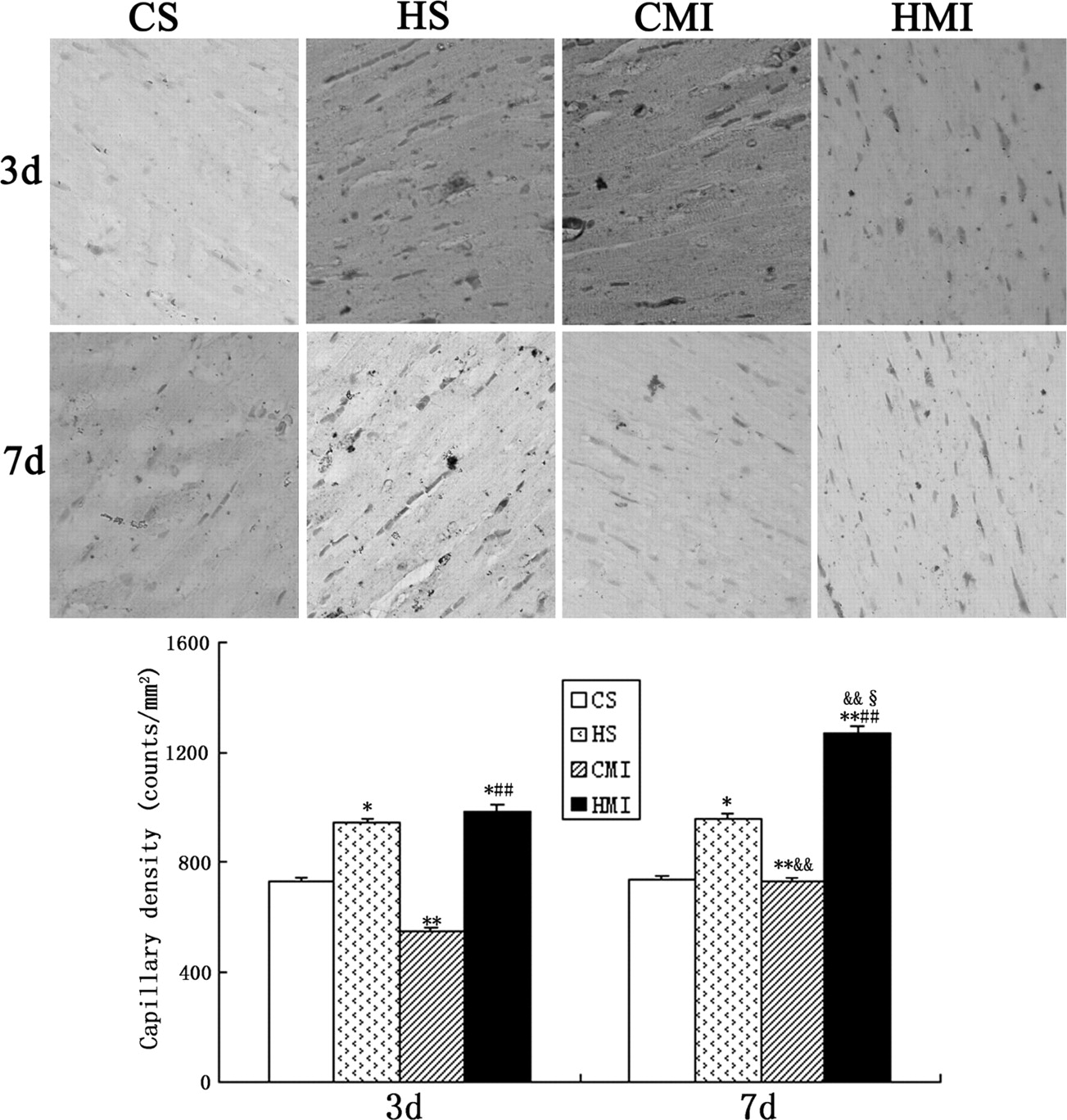
Compared to the CS group, the capillary density in the HS group increased by 24% 3 days after the operation (946 ± 25 vs. 720 ± 20 counts/mm2, P < 0.05), which maintained this high density by 7 days (952 ± 20 counts/mm2 vs.736 ± 14 counts/mm2, P < 0.05). In the CMI group, the capillary density was significantly lower than that of the CS group on day 3 after the operation (542 ± 18 counts/mm2 vs.720 ± 20 counts/mm2, P < 0.01), but it returned to the level of CS group after 7 days. The HMI density on day 3 was significantly higher than those of the CS and CMI groups, but capillary densities of the HMI and the HS groups were not different. It further increased to a level significantly higher than all the other 3 groups on day 7 (Fig. 3).
Protein Levels for VEGF.
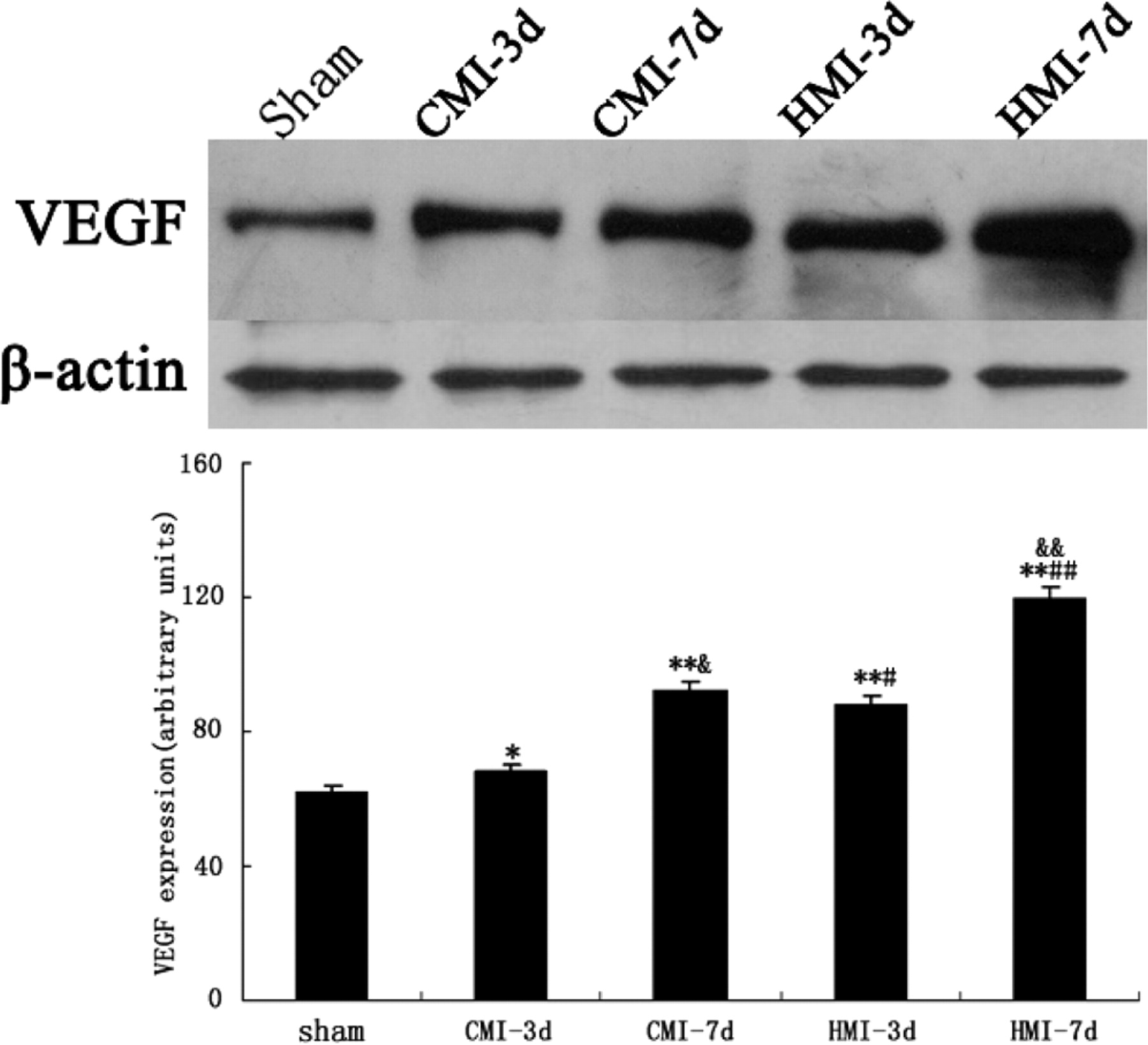
In the CMI group, the protein level of VEGF increased moderately (9%) after 3 days of LAD occlusion, compared to the CS and HS sham groups. It increased to a greater extent (29%) after 7 days. In the HMI group, the protein level of VEGF was elevated by 30% and 47% after 3 and 7 days of LAD occlusion, respectively, significantly higher than those of the CS and HS sham groups and the CMI group. The level at 7 days post-LAD ligation was also significantly higher than that at 3 days in the HMI group (Fig. 4).
Discussion
In clinical practice, HBO has been indicated to be beneficial to the myocardial ischemia induced by carbon monoxide poisoning (9) and the function in areas of ischemic myocardium at hibernation (10). Besides the effect of post HBO treatment to reduce cardiac injuries (11–12), HBO preconditioning also offers tissue protection. HBO preconditioning has been demonstrated to attenuate ischemia-reperfusion injury in various organs including the heart (4, 5, 13), brain (14, 15), liver (16), and spinal cord (17, 18). The present study observed that HBO preconditioning significantly reduced infarct size and improved heart function in a rat model of chronic myocardial infarction. This observation may have clinical potentials for cardiac thoracic surgery such as coronary bypass or heart transplant that HBO preconditioning may reduce ischemic injury to myocardium.
Previous studies suggest that HBO-induced cytoprotection is associated with enhanced expression of antioxidant enzymes (5, 17), suppressed apoptosis due to improved balance between anti- and pro-apoptosis proteins (4, 14, 19), activation of transcription factors such as NF-κB (4, 6), and intermediary metabolic enzymes, or cytoprotective heat shock proteins (11–12). However, the exact mechanism for HBO-induced myocardial protection especially in the situation when HBO is applied as a preconditioning modality has yet to be understood. VEGF is but one of several proteins mentioned above that may be induced by intermittent bouts of hyperbaric oxygen in normal and ischemic myocardium. Similar effects of HBO on the stimulation of neovascularization have been reported in flaps, wounds, irradiated tissues, and grafts (3). We are not aware of a similar study showing neovascularization by HBO in ischemic myocardium.
We demonstrated in this study that HBO preconditioning increased myocardial capillary density and the level of VEGF expression. Especially the increased capillary density occurred in HS group without ischemia and reperfusion (Fig. 3), indicating that HBO preconditioning may enhance angiogenesis in the normal myocardium. Apparently cardiac ischemia and reperfusion potentiated angiogenesis mechanisms that higher VEGF protein levels are observed (Fig. 4). This endogenous angiogenesis of myocardium after ischemia and reperfusion insult is further enhanced by HBO preconditioning in HMI animals.
The mechanisms for the enhanced capillary density may be related to the levels of VEGF, a potent angiogenic factor specific for neovascularization (6, 7), in myocardium. Consistent with the observation on the capillary density, we found that the LAD-ligated hearts expressed more VEGF in a time-dependent fashion. This endogenous VEGF expression after ischemia and reperfusion injury is further potentiated by HBO preconditioning (Fig. 4). These observations are also consistent with a report by others that delayed angiogenic compensation occurs after the ischemic insult (20). Furthermore, HBO induced VEGF expression has been observed in liver (21) and in wounds (22). The underlying mechanisms for VEGF induction by HBO could be associated with the activation of c-Jun/AP-1, ERK and JNK pathways (23).
In conclusion, the present study demonstrated that HBO preconditioning reduced infarct size and improved heart function in a rat model of myocardial infarction. The protection of HBO against myocardial infarction may be associated with accelerated angiogenesis, as evidenced by increased capillary density and VEGF protein level in ischemic hearts pre-exposed to HBO. It is suggested that HBO might be a potential therapeutic strategy for myocardial infarction.
The changes of LVSP (A), +dP/dtmax (B) and −dP/dtmax (C) after 3 and 7 days of LAD occlusion. Results are expressed as means ± SEM. Each group contains nine rats. * P < 0.05, ** P < 0.01 vs. CS/HS; #
P < 0.05, ##
P < 0.01 vs. CMI. Infarct size, expressed as a percentage volume of the infarct area versus the risk area, in rat hearts subjected to permanent LAD occlusion for 3 days. Left panel: representative photographs of serial heart sections stained with Evan’s blue and TTC. Right panel: quantitative analysis of infarct size. Results are expressed as means ± SEM (n = 9 for each group). #
P < 0.05 vs. CMI. Determination of capillary density in the myocardium of rats subjected to HBO and LAD occlusion. Upper panel: representative photographs of tissue sections immuno-stained with a monoclonal anti-CD31/PECAM-1 antibody (×400). Lower panel: calculations and comparisons of capillary density. Results are expressed as means ± SEM (n =9 for each group). * P < 0.05, ** P < 0.01 vs. CS; ##
P < 0.01 vs. CMI; &&
P < 0.01 vs. the same treatment at 3 days. §
P < 0.05 vs. HS. Protein levels of VEGF in the hearts of sham, CMI, and HMI rats. Upper panel: representative Western blot image for VEGF and β-actin. Lower panel: densitometry analyses of VEGF levels. Values are means ± SEM (n =9 for each group). * P < 0.05, ** P < 0.01 vs. sham; #
P < 0.05, ##
P < 0.01 vs. CMI at the same timepoint; &
P < 0.05, &&
P < 0.01 vs. the same treatment at 3 days.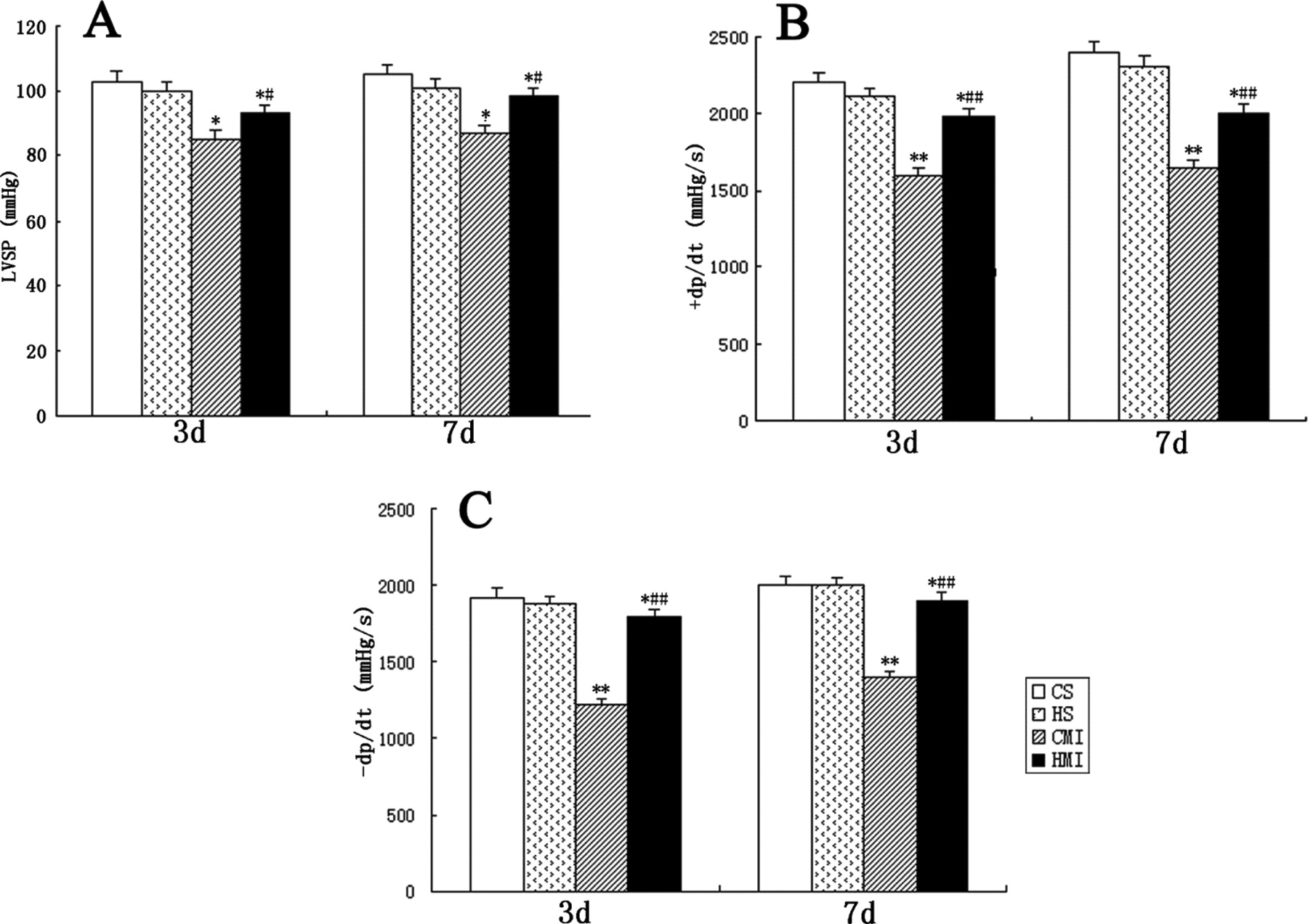
Footnotes
This study was supported by grant from the National Natural Science Foundation of China (No. 30500579).
1
Cuihong Han and Li Lin contributed equally to this work.
Acknowledgements
We thank Wenwu Liu and Yun Liu for their contributions to this work.