
Abstract
Paclitaxel is a chemotherapeutic agent used for the treatment of metastatic breast cancer. 2,5,7,8-Tetramethyl-2R-(4R, 8R-12-trimethyltridecyl) chroman-6-yloxyacetic acid (α-TEA) is an analog of vitamin E that inhibits primary tumor growth and the incidence of lymphatic and pulmonary metastases in preclinical animal models. Here, the efficacy of sequential treatment with paclitaxel and α-TEA was tested in the BALB/c syngeneic 66cl-4-GFP mammary cancer model. Both agents were formulated into liposomes and delivered by inhalation in an effort to increase anti-tumor efficacy and minimize paclitaxel toxicity. Combination treatment consisting of twelve days of every-other-day treatment with aerosolized paclitaxel (approximately 0.46 μg/mouse/treatment) followed by a daily regimen of aerosolized α-TEA (36 μg/mouse/treatment) significantly decreased primary tumor burden when compared to untreated or liposome control groups and was significantly better than individual treatments (P < 0.05). Importantly, combination treatment was significantly better at reducing lung and lymph node micrometastatic foci when compared to control and individual treatment groups (P < 0.05). Immunohistochemical analyses of tumor sections showed combination treatment when compared to liposome control or individual treatments to significantly decrease total number of cells staining positive for the endothelial cell marker CD31 or for the Ki67 marker of cellular proliferation and increase the number of apoptotic (TUNEL positive) tumor cells (P < 0.001). Studies addressing the toxicity of α-TEA demonstrated that α-TEA formulated in liposomes and delivered by aerosol (72 μg/mouse/day) or gavage (5 mg/mouse/day) for 25 days did not cause blood, liver, or kidney toxicity. In conclusion, sequential inhalation delivery of liposomal-formulated paclitaxel and α-TEA produces significantly better anti-tumor outcomes than single treatments.
Introduction
Paclitaxel is used for the treatment of several types of cancer including metastatic breast, advanced ovarian, and non–small-cell lung cancers (1). Paclitaxel is an anti-mitotic agent that binds to the β-tubulin subunits of microtubules, inhibiting microtubule breakdown leading to mitotic arrest, disruption of cell cycle progression, and induction of apoptosis (2). Since paclitaxel is not soluble in water, different formulations have been tried. One formulation, which is sold under the trade name Taxol®, is paclitaxel dissolved in Cremophor EL, a polyoxyethylated castor oil, but this formulation can cause severe allergic reactions in some patients. Newer formulations include paclitaxel bound to albumin (sold under the trade name Abraxane) and paclitaxel formulated into liposomes (3, 4).
2,5,7,8-Tetramethyl-2R-(4R, 8R-12-trimethyltridecyl) chroman-6-yloxyacetic acid (abbreviated α-TEA for alpha-tocopherol ether–linked acetic acid analog) is an analog of vitamin E (RRR-α-tocopherol). Alone and in combination with other anticancer agents, it has been shown by our lab and others to significantly reduce tumor burden and metastases in xenograft and syngeneic animal models of breast, ovarian, and prostate cancer (5–8). α-TEA mediates its anticancer actions by inhibiting DNA synthesis, blocking cell cycle progression, inducing apoptosis, and down-regulating inhibitors of apoptosis (reviewed in Ref. 9).
Based on the need to develop more effective and less toxic chemotherapeutic regimens for breast cancer, the studies presented here address the anti-tumor outcomes of using liposomal-formulated paclitaxel delivered every other day by inhalation for twelve days, followed by daily aerosol treatments of liposomal-formulated α-TEA for ten days, in comparison to untreated and liposome control groups as well as single treatments of α-TEA and paclitaxel formulated in liposomes and administered by inhalation in the same sequence.
Materials and Methods
Animals.
Female BALB/c mice at 6 weeks of age (20–25 gm body weight) were purchased from Jackson Labs (Bar Harbor, ME). The mice were housed 5/cage at the Animal Resource Center at the University of Texas at Austin at 74 ± 2°F with 30–70% humidity and a 12-h alternating light-dark cycle. Animals were given water and standard lab chow (Harlan Teklad #2018 Global 18% Protein Rodent Diet; Madison WI) ad libitum. Guidelines for the humane treatment of animals were followed as approved by the University of Texas Institutional Animal Care and Use Committee.
Tumor Cell Inoculation and Experimental Design.
Source of 66cl-4 cells originating from a spontaneous mouse mammary tumor, stable transfection with an expression vector for enhanced green fluorescence protein (GFP), and cell line maintenance have been described previously (10). Mice were injected with 100 μl of 2 × 106 66cl-4-GFP cells/ml in the inguinal area at a point equal distance between the 4th and 5th nipples on the right side, using a 23-gauge needle. Sixty mice (10 mice/group) were assigned to 6 groups: (i) no treatment throughout, (ii) liposomes only for both treatment periods, (iii) first liposome followed by α-TEA, (iv) first paclitaxel followed by α-TEA, (v) first paclitaxel followed by liposomes, and (vi) first paclitaxel followed by no treatment. Paclitaxel treatments were initiated 7 days following tumor cell inoculation and continued every other day for a total of 6 treatments (see Fig. 1A). α-TEA treatments began following termination of paclitaxel treatments (on day 18 post tumor cell inoculation) and continued daily until the end of the study. Tumors were measured using calipers every other day, and volumes were calculated using the formula: volume (mm3) = [width (mm)2 × length (mm)]/2 (11). Body weights were determined on a weekly basis to monitor the possibility of drug toxicity.
Preparation of α-TEA and Paclitaxel Liposomes for Delivery by Aerosol.
α-TEA (FW = 488.8) was prepared at high purity (99% pure) as previously described (5). Paclitaxel (FW = 853.9) was purchased from Sigma Chemical Co. (St. Louis, MO). α-TEA/liposome ratio of 1:3 (w/w) was prepared as described previously (5). Paclitaxel was prepared as previously described (12). Briefly, the lipid [1,2-dilauroyl-sn-glycero-3-phosphocholine (DLPC); Avanti Polar-Lipids, Inc., Alabaster, AL] was dissolved in tertiary-butanol (Fisher Scientific, Houston, TX) at a concentration of 180 mg/ml, then sonicated in a water bath to obtain a clear solution. Paclitaxel at 18 mg/ml was dissolved in tertiary-butanol and vortexed until all solids were dissolved. The two solutions were combined in equal amounts (vol:vol) to achieve the desired ratio of 1:10 paclitaxel/liposome. All treatments were frozen at −80°C and lyophilized overnight to dryness. The formulations were stored at −20°C until used.
Aerosol Delivery.
Aerosol was administered to mice as previously described (3, 4). Briefly, an air compressor (Easy Air 15 Air Compressor; Precision Medical, Northampton, PA) producing a 10 L/min airflow was used with an AeroTech II nebulizer (CIS-US, Inc., Bedford, MA) to generate aerosol. Prior to nebulization, vials of α-TEA/lipid powder (75 mg/vial) and paclitaxel/lipid powder (1 mg/vial) were brought to room temperature, then reconstituted by adding 3.75 ml and 4 ml distilled water, respectively, to achieve the final desired concentration of 20 mg α-TEA/ml and 250 μg paclitaxel/ml. The mixtures were allowed to swell at room temperature for 30 min, with periodic inversion and vortexing, and then added to the nebulizer. Mice were placed in plastic cages (7 × 11 × 5 in.) with a sealed top in a safety hood. Aerosol entered the cage via a 1-inch accordion tube at one end and discharged at the opposite end through the top of the treatment chamber. A one-way pressure release valve was used to equalize the pressure in the treatment chamber. The total amount of α-TEA used was 75 mg/cage/treatment and paclitaxel was 1 mg/cage/treatment. Animals were exposed to aerosol until all of the treatment was aerosolized (approximately 15 min). Estimates of final drug delivery to the respiratory tract of each mouse per treatment are: approximately 36 μg of α-TEA/mouse and 0.46 μg of paclitaxel/mouse (13). Aerosolized liposomal drug delivery also includes oral ingestion because of swallowing of nasal and lung mucus secretions, and in mice, there is the added oral ingestion factor created by their inborn grooming behavior, which rapidly facilitates the translocation of any drug deposited onto the fur into the digestive tract (14).
Lung and Lymph Node Metastases.
Visible tumor foci were counted in all five lung lobes at time of sacrifice. Fluorescent micrometastatic foci were counted using a Nikon fluorescence microscope (TE-200; ×200 magnification), as previously described (5). For micrometastatic foci analyses, the left lung lobe was flattened and the top and bottom surfaces were scored for three size groupings of fluorescent tumor cell foci: <20 μm, 20–50 μm, and >50 μm. Based on a typical 66cl-4-GFP tumor cell diameter of 10–20 μm, the <20 μm grouping is thought to represent solitary cells, the 20–50 μm grouping to represent two to five cells, and the >50 μm grouping to represent microscopic metastases of more than five cells.
Immunohistochemistry.
Deparaffinized sections (5 μm) of tumor tissue (n =10 separate tumors per group) were used to assess apoptosis, cell proliferation, and blood vessel density. Apoptosis was assessed using reagents supplied in the ApopTag In Situ Apoptosis Detection kit (Intergen, Purchase, NY), according to the manufacturer’s instructions. Nuclei that stained brown were scored as positive for apoptosis and those that stained blue were scored as negative. At least sixteen ×400 microscopic fields were scored per tumor. Cellular proliferation was assessed using antibody to the Ki-67 antigen, which is a nuclear antigen expressed in proliferating cells and which serves as an indicator of a cell undergoing active cell division, using previously published procedures (5). Ki-67–positive stained (brown) cells were counted in five separate fields per sample. Entire tumor sections were scored for CD31 stained blood vessels (brown) and adjusted for tumor size by dividing number of CD31-positive staining vessels by length × width of tumor tissue mounted on slide, as previously described (15).
α-TEA Toxicity Assessment.
In a separate study conducted prior to the combination paclitaxel study, six-week-old normal (i.e., non–tumor-bearing) female BALB/c mice were treated with liposome-formulated α-TEA, administered by aerosol or gavage. There were 5 groups of 5 mice/group: untreated control, aerosol vehicle (liposome) control, gavage vehicle (liposome) control, α-TEA delivered by aerosol, and α-TEA delivered by gavage. Mice were treated twice daily with α-TEA delivered by aerosol, depositing approximately 72 μg of α-TEA into the respiratory tract/mouse/day for 25 days. Empty liposome was administered twice daily to control mice, delivering the same amount of liposome as in α-TEA aerosol–treated group. α-TEA was delivered by gavage once daily at 5 mg/day/mouse for 25 days. Empty liposome was delivered by gavage once daily to control mice, delivering the same amount of liposome as in α-TEA gavage–treated group. At the completion of the 25 days of treatment, mice were transported to the University of Texas M.D. Anderson Cancer Center, Michael E. Keeling Center for Comparative Medicine and Research, Department of Veterinary Sciences, Bastrop, Texas, where they were euthanized and complete blood counts and serum chemistry tests were run to detect any signs of toxicity in the blood, liver, or kidneys.
Statistical Analyses.
Tumor growth was evaluated by transforming volumes using a logarithmic transform (base 10) and analyzed using a nested two-factor analysis of variance using SPSS (SPSS, Inc., Chicago, IL). Means and SEM of toxicology data, numbers of visible and micrometastatic foci, and immunohistochemical assay results were calculated for each treatment using Prism software version 4.0 (Graphpad, San Diego, CA), and results were subjected to the two-tailed Mann-Whitney rank test using Prism 4.0 to determine if there were significant differences in the treatments as compared to the appropriate control. A level of P < 0.05 was regarded as statistically significant.
Results
Tumor Volume.
Comparison of average tumor volumes throughout the course of treatment showed that paclitaxel + liposome, paclitaxel + no treatment, and paclitaxel + α-TEA treatment groups were all significantly reduced when compared to either the liposome or untreated control groups (P < 0.001; Fig. 1A). The paclitaxel + α-TEA combination treatment group showed mean tumor volumes throughout the course of the experiment that were significantly lower than either the α-TEA or paclitaxel groups (P < 0.001). Although a marked decrease in tumor volume was noted following initiation of α-TEA treatments at 19 days post–tumor cell inoculation, average tumor volumes during the prior liposome treatment phase resulted in this treatment group showing a significant difference from liposome but not untreated controls. Comparison of the average tumor volumes throughout the course of treatment between the untreated group and the liposome control group showed no statistically significant difference (P < 0.05). Although the difference was not statistically significant, one reason the untreated group tumor burden tracked below the liposome group may be attributable to two mice in the untreated group whose tumors grew very slowly in comparison to the others in this group.
Animal Weights.
Animal weights were measured the first day of every treatment week over the course of the study (four measurements in total). Over the duration of the study, mean animal weights for control and each treatment group showed no significant overall difference, based on assessment by the Mann-Whitney rank test (Fig. 1B). The use of aerosol-delivered and liposomal-formulated paclitaxel produced no obvious toxicity, in contrast to severe weight loss observed in a previous study using IP-injected paclitaxel administered every other day at 20 mg paclitaxel/kg body weight (data not shown).
Visible Lung Metastases.
Upon completion of the study, animals were euthanized and all five lung lobes from each mouse were examined for visible tumor cell foci (Table 1). In comparison to either control, all treatments produced a significant decrease in total number of animals/group exhibiting visible lung tumor foci and in total number of visible lung tumor foci observed (P < 0.05; Table 1), with the exception of the number of animals per group having visible lung metastatic foci in the paclitaxel + liposome treatment group in comparison with the liposome control group.
Micrometastatic Lung and Lymph Node Foci.
Since the 66cl-4 mammary cancer cells used in this study are tagged with green fluorescent protein, this permitted the scoring of micrometastatic foci and their classification into three size categories: <20 μm, 20–50 μm, and >50 μm (Fig. 2). Based on a typical 66cl-4-GFP tumor cell diameter of 10–20 μm, the <20 μm grouping is thought to represent solitary cells, the 20–50 μm grouping to represent two to five cells, and the >50 μm grouping to represent microscopic metastases of more than five cells. Since the biological potential for different sized micrometastatic lesions is unknown but may differ, we have presented the different size groupings for completeness. Data showed a significant decrease in total number of micrometastatic lung foci in all treatment groups (liposome +α-TEA, paclitaxel + α-TEA, paclitaxel + liposome, paclitaxel alone) in comparison to either of the two control groups (P < 0.001; Fig. 2A). There were 95% fewer total micrometastatic lung foci in the combination treatment group compared to either untreated or liposome-only controls. The liposome + α-TEA, paclitaxel + liposome, and paclitaxel alone treatment groups had 67%, 76%, and 78% fewer micrometastatic foci than controls, respectively. Additionally, the total number of micrometastatic foci for all three size categories of the combination treatment group was significantly different from individual treatment groups (P < 0.0001; Fig. 2A).
Green fluorescent micrometastatic foci in the axillary and brachial lymph nodes from each treatment group were counted (Fig. 2B). All treatment groups exhibited a significant reduction in total micrometastatic foci when compared to the control groups (P < 0.0001). The combination treatment group had 92% fewer total micrometastatic lymph node foci in comparison to either untreated or liposome-only control groups (P < 0.0001; Fig. 2B). Also, as observed in the lung, all three size categories, in addition to total number of lymph node micrometastatic foci in the combination treatment group, were significantly reduced when compared to either α-TEA or paclitaxel individual treatment groups (P < 0.0001). The individual treatment groups showed 35% (liposome + α-TEA), 53% (paclitaxel + liposome), and 48% (paclitaxel alone) fewer micrometastatic lymph foci in comparison to control (P < 0.0001).
Cell Proliferation and Apoptosis.
All treatment groups except liposome +α-TEA showed a significant (P < 0.05) decrease in tumor cell proliferation and increase in apoptotic cells in comparison to controls (Fig. 3A and B). Importantly, the combination treatment produced both a decrease in tumor cell proliferation and an increase in tumor cell apoptosis that was not only significantly different from the control groups, but also significantly different from the individual treatments (Fig. 3A and B).
Blood Vessel Density.
All treatment groups significantly reduced the total number of CD31 (PECAM-1)-positive staining endothelial cells in comparison to either control (P < 0.0001; Fig. 3C). The combination treatment produced significantly fewer blood vessels in comparison to individual treatments.
α-TEA Does Not Exhibit Toxicity.
Six-week old female BALB/c mice treated with liposome-formulated α-TEA delivered by aerosol (72 μg/mouse/day) or gavage (5 mg/mouse/day) daily for 25 days did not exhibit any hematological or clinical biochemical measures of blood, liver, or kidney toxicity (Table 2). The only parameter that was judged to be significantly different from empty liposomes administered by inhalation was an increase in total lymphocytes in the animals receiving α-TEA by aerosol (P = 0.03). Additionally, no significant differences in body weights were observed (data not shown).
Discussion
This study demonstrated that sequential treatments of paclitaxel and α-TEA, in which both agents were formulated in liposomes and administered by inhalation, markedly inhibited growth of 66cl-4-GFP mammary tumor cells in BALB/c mice and was well tolerated. The combination treatment was equally good as or significantly better than single-agent treatments for all anti-tumor parameters examined, including reduction of tumor burden (significantly better), reduction in number of animals/group exhibiting visible lung metastatic foci, reduction in total number of visible lung metastatic foci, and reductions in total numbers of lung and lymph node micrometastatic foci (significantly better). Studies addressing mechanisms of anticancer actions showed the combination treatment to be significantly better than either single-agent treatment in reduction of tumor cell proliferation, enhanced tumor cell apoptosis, and reduction in total number of tumor-associated blood vessels.
Toxicological studies of α-TEA formulated in liposomes and delivered either orally by gavage or by inhalation to normal (non-tumor bearing) female BALB/c mice showed no significant variation from controls except for a higher total lymphocyte count in animals receiving α-TEA by aerosol (Note: this variation was not observed in animals receiving α-TEA by gavage). Neither the biological reason for this increase nor the impact of this increase is understood at this time.
Due to the poor prognosis of metastatic breast cancer, there is a clear therapeutic need for new active agents and/or combination treatments to improve longer progression-free survival times (16). Studies reported here addressed the hypothesis that a new (clinically untried) vitamin E analog, α-TEA, in combination with paclitaxel, a clinically effective agent sometimes limited by bioavailability and/or formulation toxicity, if formulated in liposomes and delivered by inhalation will increase treatment efficacy and be well tolerated. The findings presented here provide justification for further studies of this drug combination regimen.
Ongoing research seeks newer formulations of paclitaxel to increase solubility and reduce toxicity as well as studies to evaluate the effects of paclitaxel in combination with other chemotherapeutic and biologic-based antitumor agents (17, 18). Recently, nanoparticle albumin-bound paclitaxel (named nab-paclitaxel or Abraxane; Abraxis BioScience, Inc., Los Angeles, CA) showed several advantages including high tumor retention, improved antitumor efficacy and reduced toxicity over the conventional Cremophor solvent–based paclitaxel (Taxol®; Bristol-Myers Squibb Co., Princeton, NJ; 19). Research into combinations of paclitaxel and anti-vascular endothelial growth factor A (VEGF-A) antibody bevacizumab (Avastin®; Genentech Inc., South San Francisco, CA) and the humanized monoclonal antibody to the HER2/neu member of the epidermal growth factor receptor family trastuzumab (Herceptin®; Genentech Inc., South San Francisco, CA) suggest improved outcomes (17, 18). One potential advantage of the combination therapy used here is the use of lower paclitaxel dosage. It is noteworthy that the dose of paclitaxel used in these studies (namely, 0.1 mg/m2/day) is markedly lower than the usual recommended dose of 175 mg/m2 (administered by three-hour intravenous infusion every three weeks; 20). Thus, results reported here support the previously reported therapeutic effectiveness of paclitaxel formulated into liposomes and delivered by inhalation as a single agent to inhibit pulmonary metastases in a renal carcinoma model (12) and demonstrate that paclitaxel given prior to α-TEA is a highly effective combination treatment.
Vitamin E analogs are being investigated as a new class of pro-apoptotic compounds that exhibit selective anticancer actions (6, 9, 21–23). Studies reported here add support to previous studies showing the ability of α-TEA to exhibit significant therapeutic efficacy in preclinical animal models of breast, prostate, and ovarian cancer with no overt toxicity (6–9). Previous studies by our lab using the syngeneic 66cl-4-mouse mammary cancer model used α-TEA as a monotherapy with initiation of treatment starting 9 days after tumor cell inoculation, with daily treatment administered until sacrifice (13–21 days following treatment initiation). In these studies (5, 10), α-TEA–treated mice showed significantly decreased tumor burden and metastases in lungs and lymph nodes and analyses of tumor sections showed that α-TEA significantly reduced tumor cell proliferation as measured by Ki67 and increased apoptosis as measured by TUNEL. In contrast, in this study the α-TEA treatment was a control for the sequential treatment of paclitaxel followed by α-TEA; thus, the liposome + α-TEA treatment consisted of every-other-day liposome treatment instead of paclitaxel followed by every-day administration of α-TEA starting at day 18 after initial inoculation of tumor cells. Based on the marked drop in tumor volume (Fig. 1A) 48 hours after the first administration of α-TEA, it is surprising that at the time of sacrifice 9 days later we did not observe a significant decrease in tumor cell proliferation (Ki67) or increase in apoptosis in comparison to either the untreated or liposome-only controls. Whether or not the significant reduction in CD31 (PECAM-1) staining endothelial cells in these tumors can totally account for the marked reduction in tumor volume is not known.
Studies addressing toxicity of α-TEA demonstrated that α-TEA formulated in liposomes and delivered by aerosol (72 μg/mouse/day) or gavage (5 mg/mouse/day) for 25 days did not cause blood, liver, or kidney toxicity, with the exception of elevated lymphocytes in the aerosol group only. Previous studies demonstrated no genotoxicity of α-TEA when tested by: (i) bacterial mutagenesis in the Salmonella E. coli assay, (ii) chromosome aberrations in Chinese Hamster Ovary cells, and (iii) micronucleus induction in mouse bone marrow (24).
α-TEA has multiple anticancer mechanisms of action including: DNA synthesis arrest, induction of apoptosis, and blockage of survival factors, suggesting that it may have added value when used in combination treatments (9). Preliminary data from cell culture analyses show murine mammary cancer cells treated with the paclitaxel + α-TEA combination to undergo apoptosis via extrinsic (Fas/CD95, caspase 8) and intrinsic (caspase 9) death signaling. Additionally, the combination treatment markedly decreased protein levels of pro-survival factors, survivin and c-FLIP (25). Indeed, preclinical animal studies confirm that α-TEA in combination with 9-nitro-camptothecin or celecoxib significantly reduce mammary tumor volume in comparison to either treatment alone, and significantly reduce lung and lymph node metastases (15, 26). Results reported here showed that sequential use of paclitaxel and α-TEA led to increased tumor cell death, reductions in tumor cell proliferation, and reductions in formation of new tumor-associated blood vessels as the biological basis, at least in part, for the significant reductions seen in tumor volume in this preclinical model. Future studies need to address if continued rounds of sequential treatments would significantly extend life and address the anti-tumor outcomes of administering both drugs at the same time.
In conclusion, the ability of sequential paclitaxel and α-TEA treatment to significantly decrease primary tumor volume and to substantially decrease the incidence of lymphatic and pulmonary metastases in an aggressive and metastatic preclinical animal model of mammary cancer suggests a promising treatment plan for metastatic breast cancer.
Visible Lung Metastatic Foci
Evaluation of Liposomal-Formulated α-TEA Delivered by Inhalation or Gavage for Blood, Liver, and Kidney Toxicity in Comparison to Corresponding Liposome Control a
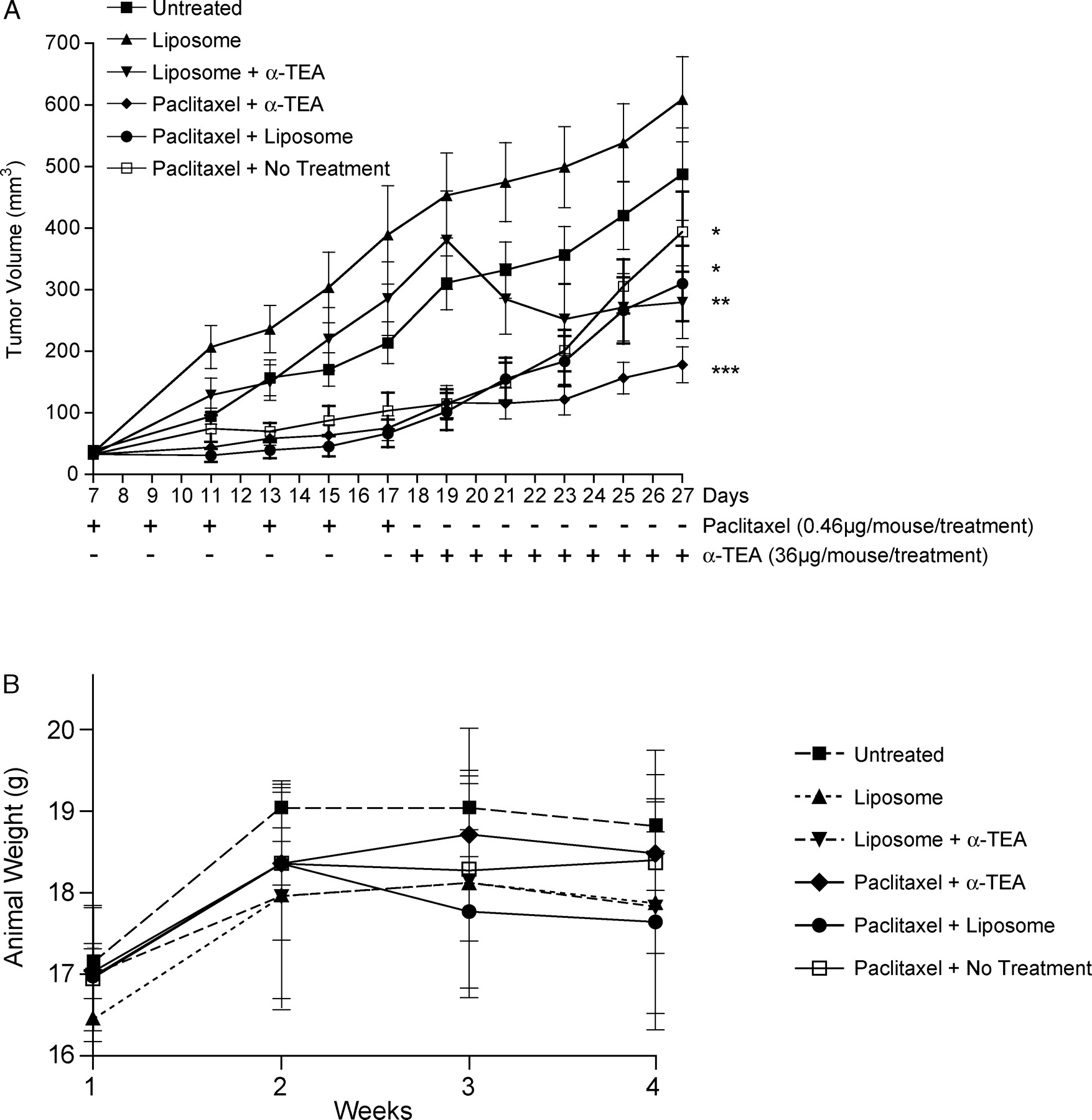
Effects of sequential aerosol delivery of liposomal formulated paclitaxel and α-TEA in combination or as single treatments on tumor volume (A) and body weights (B) over treatment time of murine 66cl-4-GFP mammary tumor cells in BALB/c mice. Paclitaxel treatments (1 mg/cage/treatment, which is calculated to be equal to approximately 0.46 μg/mouse/treatment) started 7 days after subcutaneous injection of 2 × 105 66cl-4-GFP cells/mouse and continued every other day for 6 treatments. α-TEA (75 mg/cage/treatment, which is calculated to be equal to approximately 36 μg/mouse/treatment) treatment started on day 18 and continued daily for 10 days. Tumor volume was measured by calipers in each individual animal every other day throughout the experiment. Animal weights were measured the first day of every treatment week over the course of the study (four measurements in total). Asterisks represent statistical significance over the whole period of the study, as determined using a nested two-factor analysis of variance using (SPSS). * = significantly different from untreated and liposome control groups; P < 0.05; ** = significantly different from liposome control group; P < 0.05; *** = significantly different from untreated, liposome, and individual treatment groups; P < 0.05.
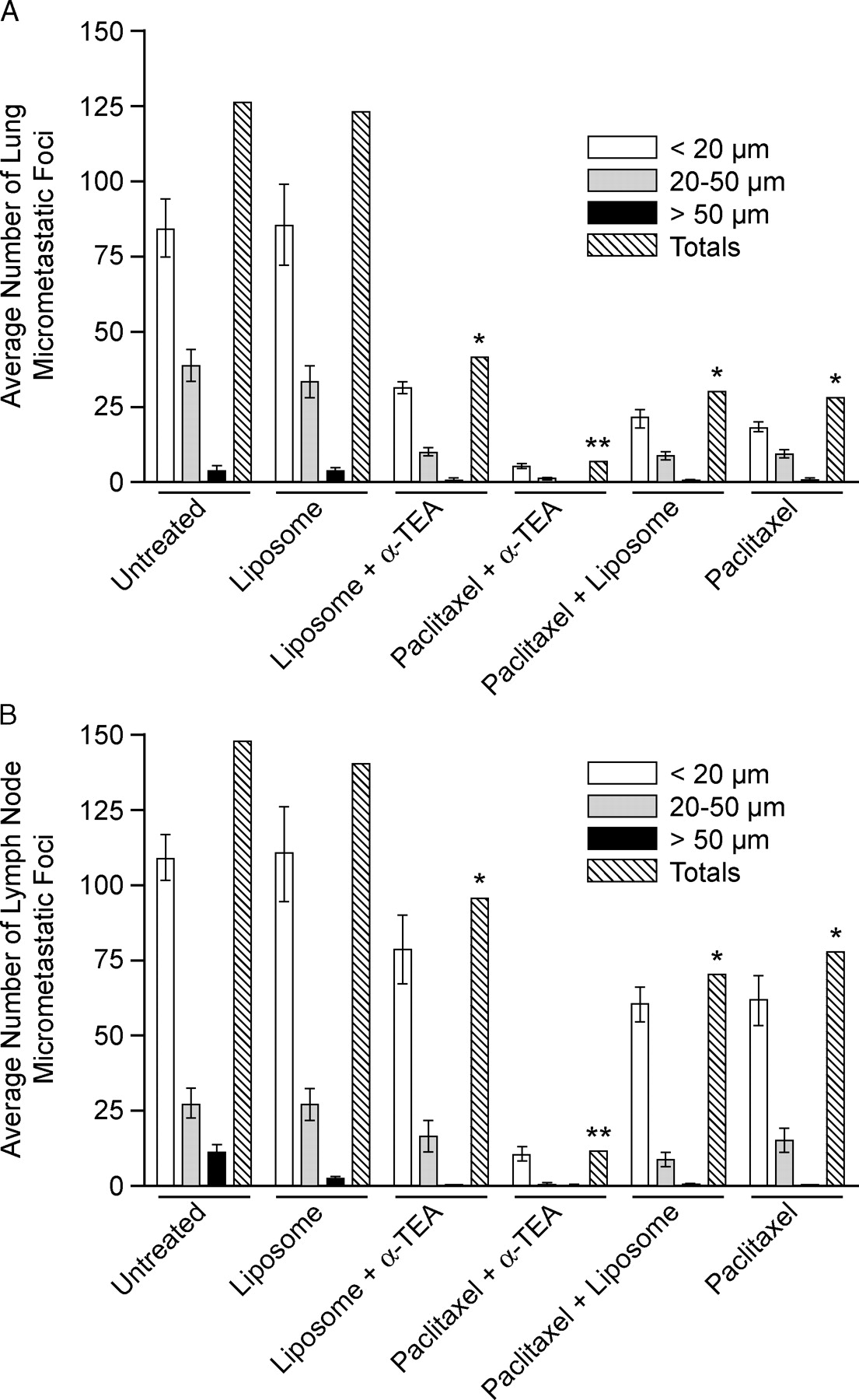
Effects of treatments on number of lung (A) and lymph node (B) micrometastatic foci. The number of fluorescent microscopic foci (<20, 20–50, and >50 μm) on the surface (top and bottom) of flattened left lung lobes from control and treatment groups were counted using a fluorescent microscope. * =significantly different from control groups; P < 0.05; ** =significantly different from control and individual treatment groups; P < 0.05.
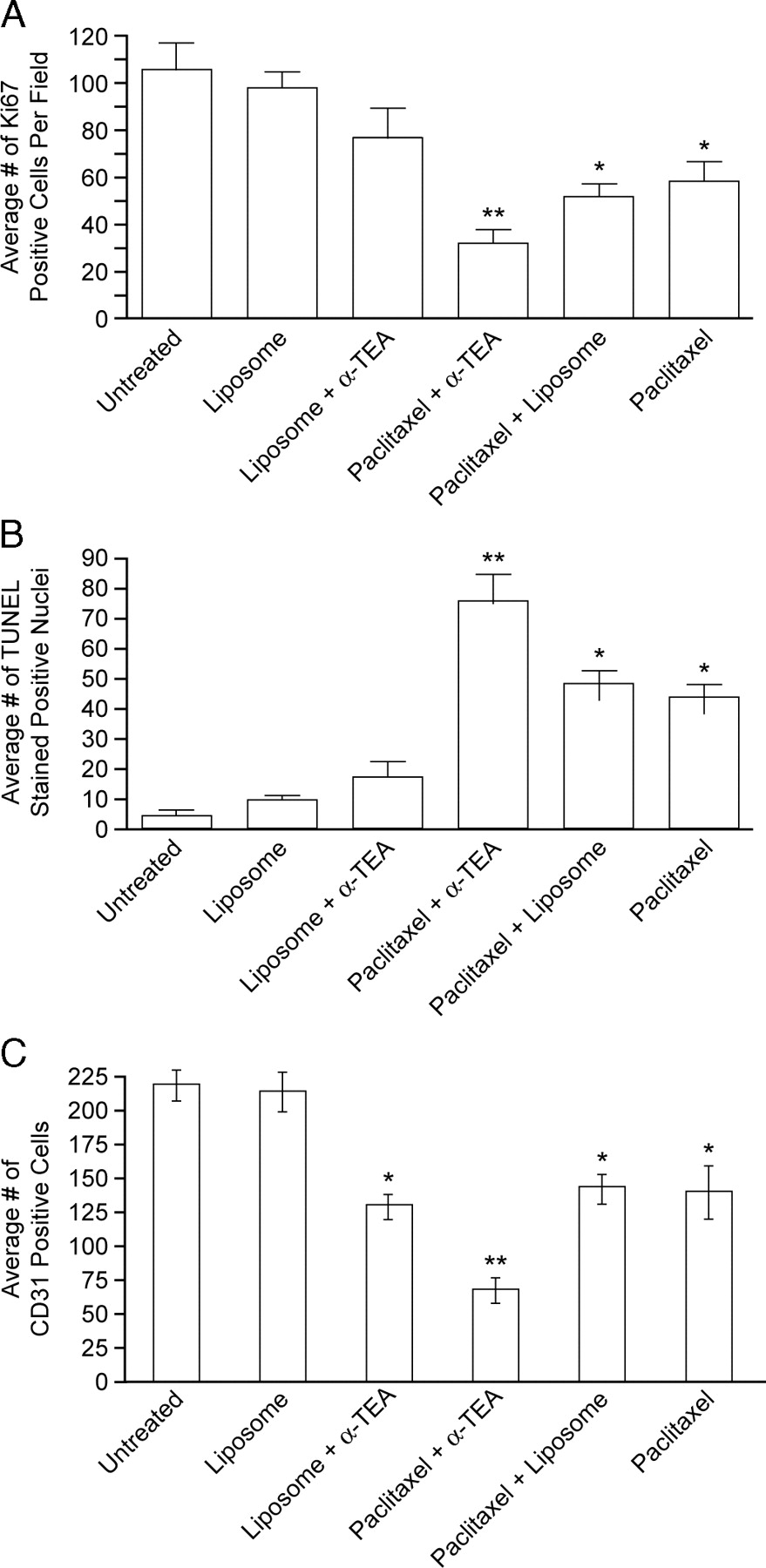
Immunohistochemical analyses of 5-μm tumor sections for proliferation, apoptosis, and number of blood vessels. (A) Proliferating tumor cells were identified using Ki-67 antibody. Five separate fields of each slide were scored for Ki-67–positive cells. (B) The terminal deoxynucleotidyltransferase-mediated dUTP-biotin nick end labeling (TUNEL) assay was used to identify tumor cells undergoing apoptosis. TUNEL-positive nuclei were counted in 16 separate fields on each slide. (C) Blood vessels were identified using antibodies to the endothelial cell surface marker CD31. Entire tumor sections were scored for CD31-stained blood vessels (brown) and adjusted for tumor size by dividing number of CD31-positive staining vessels by length × width of tumor tissue mounted on slide. Data are averages ± SEM of all tumors in each group. * = significantly different from either control group; P < 0.05; ** =significantly different from controls and individual treatment groups; P < 0.05.
Footnotes
This work was supported by grants from Public Health Service (Grant CA59739), the National Institute of Environmental Health Sciences Core Center Grant (ES007784), and the Clayton Foundation for Research. Rachel M. Snyder received a fellowship from the National Institutes of Environmental Health Sciences Training Grant (T32ES07247).
Acknowledgements
We thank the Histology Core Facility at the University of Texas M. D. Anderson Cancer Center–Science Park Research Division for preparation of H & E and immunohistochemically stained tissues, and Dr. Mark J. McArthur, Department of Veterinary Medicine, University of Texas M.D. Anderson Cancer Center–Veterinary Division, Bastrop, TX, for toxicology analyses.