
Abstract
Ambient Assisted Living (AAL) solutions have been conquering an important place among strategies to promote ageing in place and address the societal challenges of population ageing. Related available smart solutions and their pervasiveness raise security challenges requiring more flexible and better adapted characteristics. However, such solutions are frequently described in the literature without any reference to access control and the few existing works in the AAL field focus mostly on authentication or physical access control. This paper describes the SoTRAACE (Socio-Technical Risk-Adaptable Access Control) model, designed to better adapt users’ access control needs to each AAL security context. SoTRAACE takes into account contextual, technological and user’s interaction profiling functionalities and performs a quantitative and qualitative risk assessment analysis to support a smart decision-making on the most secure, private and usable way to access and display information. SoTRAACE’s unique advantages for improved availability and privacy are discussed in contrast with existing access control models and within two AAL for mental health use case scenarios. SoTRAACE’s versatility adapts to different situations and user’s goals, whether these are patient or caregiver oriented, constituting an innovative and complete proposal for enhanced trust and security in AAL or similar smart environments.
Introduction
The economic and social challenges resulting from the contemporary phenomenon of population ageing have been increasingly approached by policies designed to promote healthy and independent ageing in place. Institutional arrangements for care provision to older adults (e.g., nursing homes) have been considered unsustainable to address the problems that the demographic shift is giving rise to, thus guiding to the emergence of alternative strategies, as the use of Information and Communication Technology (ICT) to support ageing at home [18].
A milestone regarding ICT-based solutions for ageing well was the creation of the Ambient Assisted Living Joint Programme in 2008, when the Ambient Assisted living (AAL) field progressed to a greater level of maturity [3]. The AAL concept corresponds to a new paradigm, which builds on the potentials of ubiquitous ICT-devices and new forms of interaction to improve quality of life, autonomy, security, health and social integration of older adults and individuals experiencing a variety of physical or mental health conditions [2]. Expected benefits of AAL solutions are threefold: individual, by increasing safety and wellbeing; economic, by allowing an effective management of limited resources; and societal, through the promotion of better life standards [30].
However, the pervasiveness of IoT brings key security challenges, with the increased amount of personal data existing in the cloud and interchanged with a larger number of devices always connected. Indeed, the IoT environment, which can tackle the AAL domain, comprises hardware, software and middleware components, thus augmenting the complexity of the system in terms of management and security [25]. Unexpectedly, IoT devices and services are frequently described in the literature without reference to any privacy and security issues they may integrate.
Moreover, users’ interaction with the systems is also suffering a noteworthy transition with these novel technologies, to more direct and seamless interactions. This issue is especially relevant in the scope of ICT for ageing well, as older adults’ specific requirements and attitudes towards technology need to be taken into account to promote solution’s uptake. It was suggested that the age cohort of the so-called digital immigrants (the Baby Boomers) seem to prioritize security of their personal data over any other aspects of the interaction with a system [21]. Indeed, even if older adults are quite a heterogeneous group and this applies also to attitudes towards ICT, there is evidence showing that privacy and security concerns are real barriers for older adults’ adoption of ICT-mediated solutions [22,32]. This was suggested to contrast with younger adults’ attitudes, who have shown to rely on ICT, even when having privacy and security concerns, a phenomena named of ‘privacy paradox’ [11].
Hence, the new interaction paradigm in view, which includes a plethora of devices and services, together with heterogeneous groups of AAL users and stakeholders (e.g., informal and formal caregivers, health professionals, products and service providers) stresses the need for more, flexible, adaptable, lean and seamless security and access control solutions [5,10,14,31]. Access control is one of the first interactions between the users and a system and one of the most important since it carries the potential for preventing and detecting security problems at first hand and before more serious harm takes place. Also, it can help providing more adapted and adequate access to the environment and individuals with special requirements in terms of system use. Therefore, in the scope of AAL environments and user requirements, traditional access control models are not sufficient and adequate anymore. Still, research focusing on alternative access control models seems to remain scarce, apart from solutions on authentication or physical access control [10,13,27].
This paper first presents the conclusions from a narrative literature review aiming to collect and characterize access control models applied to AAL environments. Second, collected access control models were compared to an enhanced access control model named SoTRAACE (Socio-Technical Risk-Adaptable Access Control Model), presented in this article, which can be used to better adapt users and stakeholders’ access control needs to each AAL security reality and context [19]. SoTRAACE can take into account contextual (e.g., physical location as work, home, public places), technological (e.g., type of device, network connection, secure protocols) and user’s interaction profiling (e.g., user’s history of accesses to specific data) within a quantitative and qualitative risk assessment analysis to decide, for each user’s request, what is the most secure and private way to access and display patient information.
An Adaptable Visualization Module (AVM), a new improvement introduced in this paper, will take into account the decisions of SoTRAACE and display users’ requests in the most secure, usable and useful way possible. All this is performed intelligently, without requiring extra effort from the user, unless the user wants to be an active participant in the process. Hence, the SoTRAACE model is embedded in a user-centric approach also typically adopted for guiding technologies applied to AAL or smart environments, i.e., it is oriented towards user’s and contextual needs, as well as requirements and capabilities.
Background
Privacy and security applied to AAL
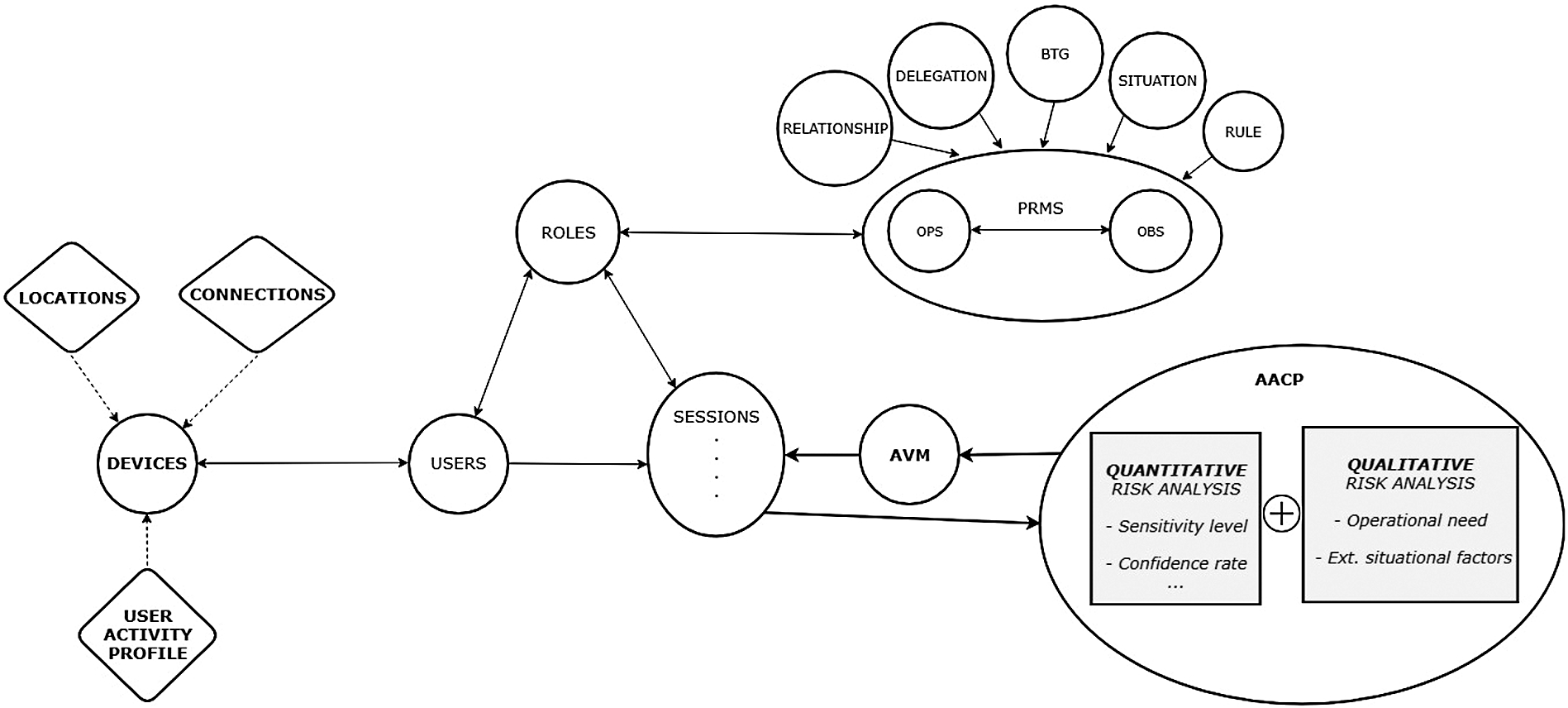
Architecture of the socio-technical risk-adaptable access control model (SoTRAACE) [19]. AVM is a new component.
Despite the potentials of AAL solutions for older adult’s empowerment, constraints to its implementation in the market as well as to its uptake by end users have been described. Indeed, despite of the hasty growing of AAL solutions, some essential aspects of AAL systems seem to have been disregarded, with meaningful gaps on interoperability and integration properties, usability, reliability, security and privacy [1,6,16,23]. In what concerns security, Minoli et al. [17] stress that infrastructure is not available, nor standards or best practices, to properly protect AAL users’ data. Indeed, each device is unique, with different security requirements and when interconnected with other devices or services such as cloud computing, security challenges multiply and are more complex to define and address. In addition, AAL solutions typically involve multi-organizational interactions, i.e., data is provided, stored and managed by different organizations [16]. Moreover, the data at stake are usually health-related and therefore sensitive, also frequently involving different components as medical sensors, records and applications [16]. Privacy threats arise as well from the use of generated data, for example, to create a user profile with personal data aggregation and sophisticated data mining techniques [24]. Privacy and security challenges for AAL, as described by Massacci and colleagues [14], also present a paradox: by one hand, dependability challenges stress that if an external entity (e.g., service provider) is unable to access the right data in the proper time, the older adult’s health and wellbeing can be jeopardized; on the other hand, privacy challenges put in evidence the issue of transference and storage of personal and sensitive data in different systems. Therefore, a conciliating option is needed, i.e., AAL privacy and security-preserving solutions, with transparency to older adults with regards to data flow [9].
To address security and privacy concerns, recent debates have been stressing the need to shift the choices and domain over data usage from developers and service providers to users, entitling those users to take control over their data, to enjoy their right to informational self-determination [24,26]. This perspective is of utmost importance to empower the users in the identification of their sensitive data and recognition of risks associated with its transmission and storage [24]. Communication aspects are of importance in this equation: the user interface must allow a proper understanding and manipulation of personal information being processed, i.e., must provide the user with information about the accessible data and offer means to control the access rights to the private information [26]. Moreover, all this must be displayed in an accessible and usable way for older adults or, if we prefer, ‘for all’. Indeed, while earlier solutions applied to health and care have been focusing more on monitoring the users (assuming the role of patients), contemporary systems seem to be progressively more compliant with the principles of citizen’s empowerment via increased user-system interaction and awareness [4]. Even if progresses are noteworthy, AAL systems still lack in user-perception and ethical frameworks, reinforcing the topics of security and privacy as main challenges in this field [4].
The SoTRAACE model (Fig. 1) integrates the basic Role Based Access Control (RBAC) entities [28] expressing the roles that users have as well as the permissions (what operations can be performed in what objects) associated to those roles (e.g., USERS-ROLES-PERMISSIONS-SESSIONS), to access available resources or objects (OBS).
Additional entities that can be further associated to PRMS (Permissions) from other RBAC extended models [7,8] and influence how these are going to be performed include:
BreakTheGlass (BTG) – for access in emergency or unanticipated situations;
SITUATION – for access restrictions regarding specific physical or logical locations;
RULE – other exceptions that need to be taken into account for specific permissions;
DELEGATION – for temporary accesses performed by a user that is usually not authorized but is referred by an authorized user (e.g., to request a second opinion on a patient’s report);
RELATIONSHIP – for accesses from users that have some relation (e.g., family relative, close friend, caregiver) to the authorized user and have been attributed (restricted/temporary) access to parts of his/her record.
New components (in Fig. 1 in bold) were integrated to increase the flexibility, user adaptation and risk assessment and awareness to the human interaction with the device. SoTRAACE architecture focuses on the use of portable devices (e.g., smartphones and tablets) and its new components include:
After having assessed the risk, AACP specifies a set of rules (the decision) that can be applied to PRMS. Decisions can vary according to the type of user, security and privacy requirements, type of device or data sensitivity. Some examples of SoTRAACE decisions can be: 1) simply block or allow the access (traditional access control); 2) enforce the fragmentation of the requested object and just allow access to some fragments (security visualization); 3) block or allow one or more operations to the object; or 4) trigger other hidden security protocols to better avoid the risk without compromising availability.
Finally, past decisions and respective parameters provided by the AACP are recorded and used to help decide each subsequent decision. This knowledge can improve algorithms that determine the risk, operational need and the rate of positive access control decisions, to build more accurate UAP and object logs and improve and monitor security measures in place.
Methods
Access control research in AAL
A narrative literature review on access control models applied to AAL was performed in order to collect and characterize those models. A comparison between encountered access control models is presented in this paper. This comparison includes the analysis of the features SoTRAACE can add to the existing research work, which were lacking.
SoTRAACE in AAL environments and use-cases
Every day, we generate great amounts of data from and to various devices, and blindly share it over different platforms, service providers and individual users, all over the globe. It is not possible today for an individual to be sure that what s/he has shared is exactly what s/he wants to be shared and to whom. On the other hand, individual’s personal Big Data (BiDa) can be a useful source to better understand what data are used for the most common interactions between the individual and the various systems and, when we know this, we can decide on the most adequate measures to protect that data.
SoTRAACE aims to automatically learn from an individual’s BiDa and from live data collected from every interaction a user makes comprising human, social and technical context at that moment (e.g., time, location, previous interactions, type of connection/device, etc.) and decides what is the most transparent, secure and usable way to both ask and retrieve the results of each request, to and from the application at hand. SoTRAACE performs a quantitative and qualitative risk assessment analysis to support that decision-making.
To demonstrate and discuss the application of SoTRAACE in AAL contexts, two use cases are described. Those build on two personas, i.e., realistic representations of the key audience under analysis, reflecting individual users with specific characteristics and requirements towards ICT. A persona representing an AAL primary end-user, i.e., an older adult who directly benefits from the solution (Use-case 1) and a persona representing a secondary end-user, i.e., an informal caregiver who benefits from the AAL solution both directly and indirectly when the needs of the primary end-user are addressed (Use-case 2). Both cases address mental health related scenarios. The two personas have different goals, needs and experiences and will require adaptable means to access and deal with information, while preserving their privacy. Both have a degree of ICT literacy which allows them to interact with mobile devices such as smartphones or tablets. More details can be found in the Results section.
Results
Access control research in AAL
To have a clearer idea on available research in this domain, two online databases (e.g., ACM and IEEE) were searched for related work published after 2008 (the last ten years). These two databases were chosen because they focus on more technical security as well as access control related themes. Search queries and terms included: (a) “Access control” AND “Ambient Assisted Living” (
SoTRAACE model vs. other available access control models for AAL applications
SoTRAACE model vs. other available access control models for AAL applications
Regarding their content, most currently available research on access control for Ambient Assisted Living solutions have been focusing on biometric authentication on IoT devices [10,12,13,27]. Only few works specifically address access control challenges in AAL. Table 1 provides a comparison between the entities/features present in the SoTRAACE model and those in previously developed access control models for AAL applications, encountered in the literature review. Massacci and colleagues [14] proposed an access control model and security architecture to provide secure and private AAL solutions in the smart-homes field. This model is goal oriented and restricts data access based on two main security principles: need to know and least privilege. However, AAL solutions typically involve diverse goals with sensors to detect and monitor human activity (e.g., dealing with a crisis situation as for instance a fall detection) and several users (e.g., older adult and informal caregiver). In this equation, it is of utmost relevance the provision of access in emergency or unanticipated situations as well as of a flexible mechanism to assess risk at interactional moments in order to adapt access needs according to the best balance between availability and confidentiality.
Satoh [29] proposed an access control model to bridge the gap between AAL and cloud computing focusing on context-aware access control including location, physical entities and relations between them. However, other factors such as users’ profiling interaction as well as technical and security contextual issues (e.g., type of network connection, security protocols in place) are not taken into account in the access control decision.
More recently, Salama and colleagues [27] propose the reuse of ABAC (Attribute-based access control) to perform access control, providing access control levels based on the attributes of people, data, and environments, therefore integrating contextual and location data. However, in resemblance to other models, this approach does not provide the required flexibility to include features such as users’ profiling interaction, emergency or unanticipated situations (which are common in healthcare environments) and adaptable risk assessment to improve overall security and availability of information.
The SoTRAACE model aims to fill identified gaps in what concerns security for AAL environments. The model integrates a BreaktheGlass (BTG) [7] solution for access provision in emergency or unanticipated situations, a quantitative and qualitative risk assessment, as well as a visualization adaptation module to better define risk assessment and adjust access needs according to the best balance between availability and privacy. Furthermore, it also integrates users’ profiling interaction in addition to technical and security contextual issues in the access control decision.
Various characteristics of SoTRAACE are applicable and necessary to AAL environments. The main RBAC entities described in the section ‘SoTRAACE model’ are the basis to create a stable standardized access control model that provides the main features to identify users, their roles and what permissions can they perform in what objects. Further, BTG or DELEGATION (and other exceptional/specific) situations can also occur in AAL contexts and the integration of these functionalities from other models in SoTRAACE is an added value.
The extended SoTRAACE components can further improve security and interaction with users in AAL solutions. The DEVICES entity is a crucial requirement for AAL since IoT devices are portable and with specific characteristics regarding data collection and usage. Similarly, to a smartphone, other devices such as smartwatches for vital signs measurement and transmission can store and transmit relevant data such as time and date as well as the location where that collection is taking place (e.g., component LOCATIONS) and the type of connection/communication that is used, even to other devices (e.g., component CONNECTIONS), including available security controls. This information can be stored through various SESSIONS or interactions to create an historical continuum of interactions and associated profiles to be used in future decisions (UAP).
Regarding the risk assessment feature, the AACP is the main component to assess users’ needs and adapt the system actions to their requirements at any moment in time. Performing and integrating both quantitative and qualitative risk allows a richer span of possible decisions that may better adapt to what the user is requesting at one time and under certain conditions. Object logs and user’s interaction history data can complement that assessment and future decisions. SoTRAACE evaluates if a user’s request is customary under specific conditions according to interaction history, therefore facilitating upcoming accesses.
For instance, in a context of continued uses (e.g., frequent vital signs monitoring), SoTRAACE can provide a seamless authentication/interaction, as previously well identified and tested devices/locations/contextual situations will not require additional identification features. Further, under the circumstance of users who face sight or even cognitive problems, SoTRAACE visualization features (e.g., AVM) can adapt device display to the best balance between availability and privacy – according to the user’s context [12].
Next, two use-cases are presented to conceptually evaluate the SoTRAACE model and verify its applicability into real world situations for further testing and analysis.
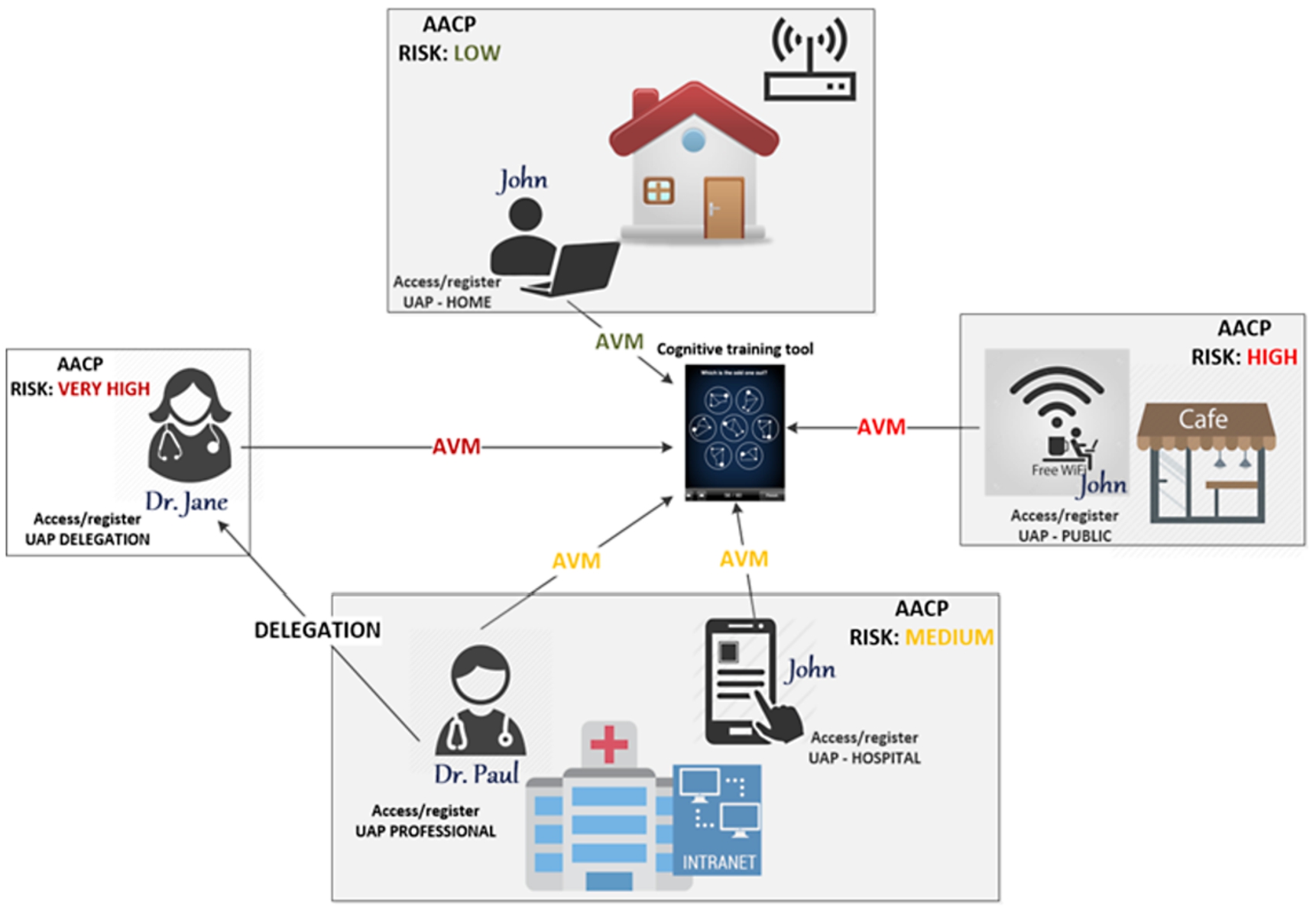
SoTRAACE model applied to the online cognitive training scenario (use-case 1).
John is 68 years old and diagnosed with Mild Cognitive Impairment (MCI). He presents a slight but noticeable decline in cognitive abilities, including memory and thinking and is interested in adopting coping strategies that may be helpful in slowing the cognitive decline. John is ICT savvy and does a frequent use of smartphone and laptop. John is followed in the department of neurology at the local hospital, where the neurologist recommended, as a complementary intervention measure, the use of an online cognitive training tool developed by the local hospital. This tool allows the prescription of individualized training programs that can be followed by the patient at any place with internet connection (e.g., home, coffee shop). The patient’s performance and program compliance can be remotely monitored by a designated health professional (here, the neuropsychologist Dr. Paul). Figure 2 illustrates the security challenges posed in this scenario and how those can be addressed by the different components of the SoTRAACE model, in particular:
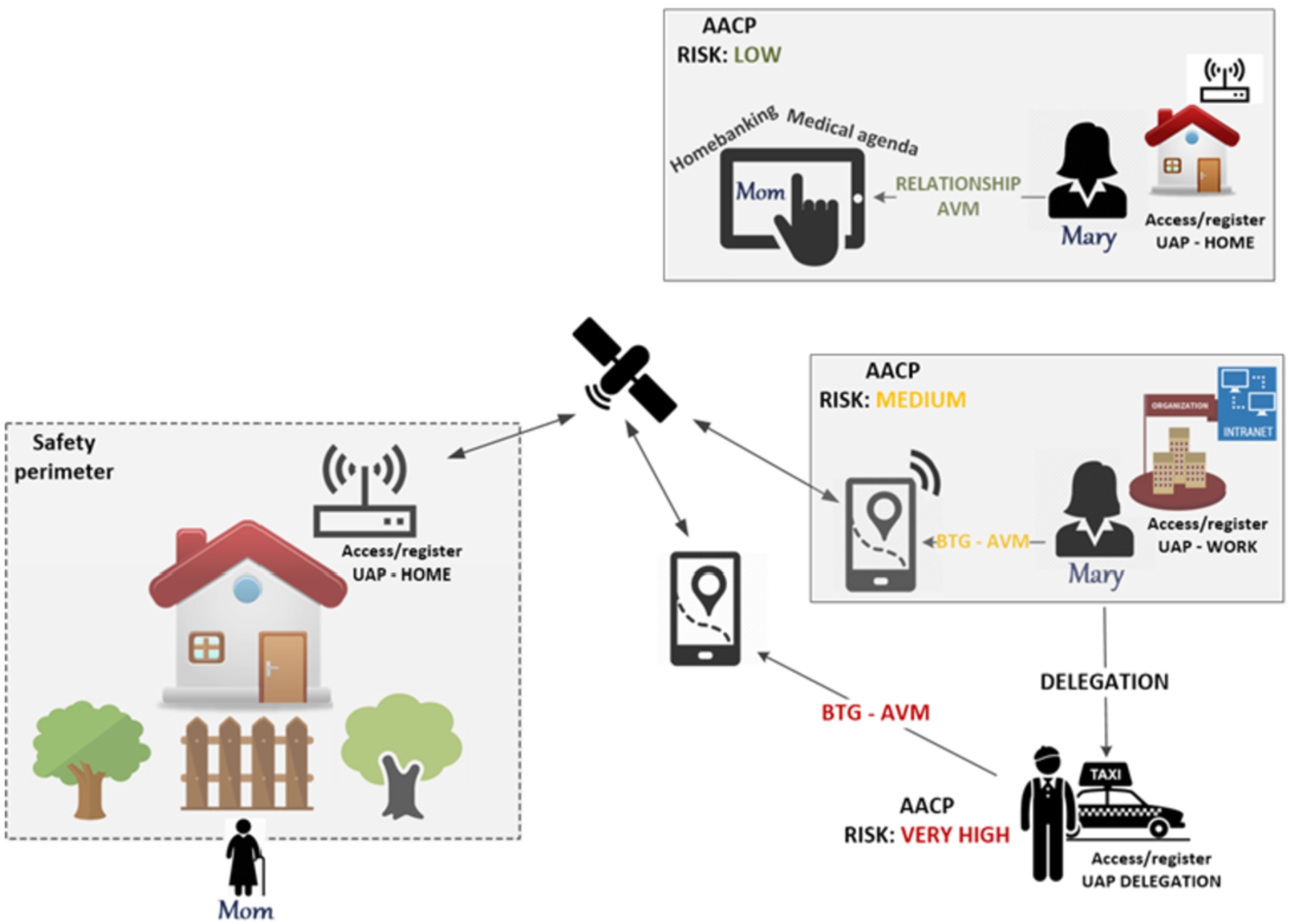
SoTRAACE model applied to the scenario of navigational aid applied to dementia (use-case 2).
Mary is 47 years old and her mom suffers from Alzheimer’s Disease (middle-stage). Mary works 40 km away from her mother’s house and she is always concerned that in case of emergency she would not be able to provide a quick answer. She would like to take care of her mother without losing her own independency and work. Mary’s mom has a housekeeper who accumulates regular home maintenance tasks (e.g., cleaning, buying groceries) with caregiving activities while Mary is at work. Recently, Mary’s mom started wandering away from her house and in one situation the housekeeper was only able to notice her absence after a couple of hours, and Mary had to leave work to search for her mom. Mary is ICT savvy and does a frequent use of smartphone and tablet/laptop, so in order to limit wandering and preventing her mom from becoming lost, Mary decided to purchase a monitoring navigational aid application for her mom’s smartphone (who wears it all the time in a cell phone pouch with a neck strap). This application allows Mary to monitor her mother’s geolocation and launching an alert when a predefined safety perimeter is crossed. When this happens the application informs and updates the exact place where her mother’s phone is located. Figure 3 illustrates the security challenges posed in this scenario and how those can be addressed by the different components of the SoTRAACE model, in particular:
Discussion
Ambient Assisted Living solutions will probably conquer an important place in an ageing society in need for sustainable and life enhancing solutions. These type of solutions have exponentially grown in the last decade to promote independent living in older adults’ preferred environments, i.e., in their own home and community. However, privacy and security measures have not developed as quickly as they should to be seamlessly integrated in such processes. This work shows that for one of the most important aspects on human–computer interactions influencing security – access control – an optimal solution was not yet developed to address new usage challenges previously described in this paper. In fact, as expressed by the presented use cases, security measures need to become another crucial feature of AAL devices, so that they can easily adapt to the environment and context of use, including user’s own interactional behaviour and characteristics. The access control model presented in this article – SoTRAACE – aims to contribute to bridge this gap.
SoTRAACE is a model that can be used to acquire various environmental and technical conditions at the moment of usage of a specific application and decides on the best balance regarding availability and security of that request. This analysis will influence the way information is displayed to the user, therefore adapting to each unique situation, regardless of who the user is (in this case the user/patient or an informal caregiver in mental health related scenarios). Different situations represent different risk levels, as assessed by the SoTRAACE model and culminating in adapted visualizations from the applications in use.
In use-case 1 (Fig. 2), John, an older adult with Mild Cognitive Impairment makes use of an online cognitive training tool as a therapeutic measure to cope with his condition. With most existing access control models, privacy of visualized information would be the same independently of the situation, technical measures or user’s interaction profile. With SoTRAACE, interactional experience is always unique. When accessing the cognitive training tool at home, the associated risk level is low due to the private protected Wi-Fi network and the highly improbable presence of unknown people around to perform shoulder surfing. In this low risky scenario, the AVM component would show all data associated with the tool, including John’s personal data, diagnosis, therapeutic measures, performance history, among others. When John is at the hospital, usually a more crowded place, privacy restrictions may be applied. There is no need to display personal data such as date of birth, complete name or address, while in situations with even higher risk (e.g., in public places with unsecure connections) only strictly fundamental data regarding the current training session is available.
This is also true when it comes to third parties accessing data, for instance the professionals monitoring John’s evolution. SoTRAACE integrates modules for delegation where unauthorized professionals can temporarily access John’s evolution to help assessing his progress. In this situation, SoTRAACE applies even more restrictions as this professional does not need to know any personal information regarding the trainee but only the strictly fundamental information to provide a recommendation (e.g., John’s training history). Once accomplished the purpose of this specific access authorization, access is revoked.
Although use-case 2 (Fig. 3) builds on the persona of an informal caregiver (Mary) of a person living with dementia i.e., a secondary end-user, there are similarities in the way SoTRAACE processes access control decisions in terms of UAPs, how ACCP calculates risk and how delegation is performed. This case also illustrates the BTG component where access is granted only in emergency situations rather than in a regular basis. Moreover, this scenario also demonstrates how SoTRAACE can be useful to adapt to both urgent and more ordinary situations (e.g., access to bank or medical data).
Furthermore, for both use-cases, there are various UAPs which are registered in all different situations. This information is used to calculate risk assessment which will mostly influence the qualitative risk analysis. The qualitative component supports the definition of access according to user’s needs and behaviours rather than relying only in technical/security aspects. It is also noteworthy that SoTRAACE adaptations are not only a matter of visual privacy issues. In riskier places there is no need for sensitive data to be transmitted over unsecure channels, unless requested by the user. Nevertheless, whomever owns the data of the application in use is in control and has always the option to access the entire spectrum of authorized information, any time (e.g., accessing personal data in a Coffee Shop that was first hidden by AVM).
Limitations: The lack of relevant research work to contrast with the SoTRAACE model, especially in what concerns access control in AAL, is a noteworthy limitation to the performance of a deeper discussion in this paper. However, this work also aims to stimulate more interest and research in this field, to bridge existing gaps. Since SoTRAACE is currently at a prototype stage, functionalities were not yet tested with users neither subjected to a user experience evaluation in terms of availability and privacy in a real setting. Forthcoming work includes refining the SoTRAACE prototype as well as design and implementation of security usability protocols to field test, in the AAL domain, the balance that SoTRAACE can bring in terms of availability and privacy features.
Conclusions
Currently, the SoTRAACE model is a complete proposal for secure and adaptable access control in AAL or similar smart environments, addressing many of the security gaps identified in the state of the art. The model allies the integration of already existing features, valuable for their adaptability and flexibility, with new components that bring richer profiling data useful to deliver decisions adapted to user’s needs and goals. This allows to seamlessly providing for the best balance between data availability and privacy, both important requirements when dealing with personal and sensitive health data.
Footnotes
Acknowledgements
The research leading to this paper has received national funding from FCT - Fundação para a Ciência e Tecnologia, I. P. in the scope of the three projects: TagUBig - Taming your Big Data (IF/00693/2015); ActiveAdvice - Decision Support Solutions for Independent Living using an Intelligent AAL Product and Service Cloud (AAL-2015-2-058, FCT Ref. AAL/0007/2015) and PD/BD/135496/2018.