
Abstract
Hyperbilirubinemia or jaundice occurs in 60% of healthy babies and 80% of preterm infants because of an increase in unconjugated bilirubin in red blood cells. It is subjective to determine the severity of jaundice by visual assessment of the skin color of a newborn, and clinical judgement is dependent on the doctor’s knowledge. The paper explains the development of a non-invasive bilirubin detection technique called CliNicS, to check the bilirubin level of premature babies and report premature births and deaths to the health organization via an IOT network. CliNicS provides a noninvasive, transcutaneous bilirubin monitoring system using LED having a wavelength of 410 nm to 460 nm, and it also provides the treatment automatically by using LCT (LED Controlled Therapy) method. The level of bilirubin will be detected by using the photo detector, and the bilirubin measurement will be displayed on the LCD display. The bilirubin levels will be transmitted to doctors and health organizations via the IOT network. The proposed method helps to detect neonatal jaundice earlier, which reduces the risk of hyperbilirubinemia in newborns and makes it easier to measure total serum bilirubin levels than ever before.
Introduction
Hyperbilirubinemia (jaundice) is one of the most prevalent diseases in the first few weeks of life, that affects 60% of normal and 80% of premature babies [2]. Blood bilirubin levels exceeding 2.0 to 2.5 mg/dl may indicate jaundice. Bilirubin is a yellowish pigment present in the blood that is excreted by the liver through an enzyme-mediated glucuronidation mechanism [17]. A high level of toxic bilirubin can result in kernicterus, a rare but fatal disease with chronic neurological effects like athetoid spasticity and sensorineural hearing loss that can also result in death.
Severe hyperbilirubinemia can result in unconjugated bilirubin passing through the blood–brain barrier, possibly causing neurotoxicity [4,25]. Therefore, early bilirubin monitoring is necessary to detect severe jaundice quickly after birth, especially in preterm newborns who may die or become disabled due to jaundice [16,20]. The management of neonatal jaundice depends on several different factors, including the baby’s age, weeks of gestation, and serial bilirubin levels.
Jaundice evaluations in hospitals can be classified as invasive or non-invasive [14,18]. Jaundice is most easily diagnosed through an invasive blood test that is taken from the feet of the baby. The problem with this approach is that it can cause stress to both parents and infants, and also there may be a chance of infection if the equipment isn’t sanitized before use [21,26]. A non-invasive approach based on Kramer’s Rule assesses skin yellowness visually. Only trained medical personnel are capable of determining whether a newborn has jaundice or not, so this procedure is subject to human error [22,31].
An alternate non-invasive approach is done by employing a bilirubinometer or jaundice meter placed on the baby’s forehead or sternum [19,28]. This device directs light into the skin of the infants and calculates the intensity of the wavelengths returned. This equipment has an extremely high cost, so it is only available in general hospitals, making it unaffordable for infant centers and researchers [9,27]. Numerous low-cost phototherapy devices have recently been created for use in low-resource settings, but there are no low-cost diagnostic tools to screen newborns for bilirubin levels and monitor their response to therapy [5,29,30].
Color card approaches [3] which uses optical methods and linear regression analysis to find the bilirubin levels and medication requirements and also it displays the result on a graphical user interface that can only be accessed by authorized personnel. This method is cost effective and detects jaundice with better accuracy. To analyze and monitor the jaundice in low-cost resource, BilliSpec [15] was proposed which detects bilirubin level from several drops of blood at the point of care. Skin optics technique [23] which comprises of an LED, and a photodiode to create a non-invasive bilirubin detector. The artificial bilirubin standard solution (ABSS) was used to replicate blood bilirubin in the tests of bilirubin degradation. A non-invasive bilirubin meter [24] that would rely on a smartphone to take colour images that would be filtered and evaluated to determine if the infant is jaundiced, which uses an artificial neural network. Another non-invasive method [7] for identifying jaundice involves projecting blue light (450–500 nm) onto the skin of the new born in a dark environment. With this approach, newborns and adults can be diagnosed for jaundice without experiencing any discomfort. A photon diffusion theory-based technique, which is valid in the 450–600 nm wavelength region aiming to offer reliable neonatal bilirubin concentration determination and increases the accuracy [6]. Neonatal bilirubin level can be measured with non-invasive methods based on spectrometry rather than the total serum bilirubin (TSB) test [10]. A noninvasive method developed independently can measure bilirubin levels accurately and precisely in infants under a variety of physiological conditions. A transcutaneous bilirubinometer [13] which simultaneously detects the bilirubin level, SpO2, and HR of newborns. Their system was able to accurately measure bilirubin during phototherapy. Deep learning strategies [1] were also used to detect jaundice which is based on skin, eye, and merged pictures, that increases accuracy in detecting bilirubin levels. Skin color analysis method [11] has been used to detect jaundice which uses a color-based digital camera as an analytical tool since it is inexpensive, objective, common, and less uncomfortable for newborns. Digital camera-based method [12] using the real-time collected photos, this approach detects jaundice and finds if the infant needs medication. Mobile Computer-Assisted Diagnosis (mCADx) tool [8], which can use sophisticated image processing and data mining techniques to diagnose neonatal jaundice.
However, the above techniques show better results in finding hyperbilirubinemia, but they were not helpful in the treatment of this disease in serious conditions, and some of the techniques may be high-cost. Therefore, further research needs to be conducted. This research attempts to suggest a hardware-based system called the (CliNicS) care living instrument for neonatal infant connectivity solution to quantify jaundice level and provide treatment in certain conditions. The development of a low-cost, precise, and non-intrusive hardware-based system is the main goal of this study. The major contributions of the proposed CliNicS method are as follows:
To monitor premature babies and to report premature births according to gestational age on a national and international scale (data are currently reported by birthweight).
It provides a noninvasive, transcutaneous bilirubin monitoring system using LED and provides the treatment using the LCT (LED Controlled Therapy) method with minimal cost.
It eliminates the risk of hyperbilirubinemia in newborns and permits the system to assess total serum bilirubin (TSB) levels easier.
The proposed method uses IOT technology that will help to contact the doctor for treatment in the earlier stage which will save the lives of the neonates.
The remainder of the paper is presented in the following way. In Section 2, the proposed CliniCs method has been described. In Section 3, the experimental results have been evaluated. In Section 4 a brief discussion has been performed and Section 5, encloses with conclusion.
Care living instrument for neonatal infant connectivity solution (CliNicS)
Jaundice is one of the most common disorders among newborns. According to the journal of perinatology-neonatology, each year approximately 40% of the 4 million preterm infants in the United States die, and it has been predicted that every year there will be an increase of almost 10% worldwide. In order to reduce the death rate of neonates, it is necessary to monitor premature babies. So, for monitoring the neonates and for reporting the National and international premature births and deaths, the CliNicS method has been developed in this paper.
In the proposed method, the bilirubin level was predicted using a LED and a photodetector and treated by using LED controlled therapy (LCT). The level of bilirubin in the blood is checked by passing the LED (410 nm to 460 nm) source on the child skin, and the actual level of bilirubin is detected by using the Photo Detector that catches the light of the LED reflected from the skin of the premature baby. Then, if necessary, the child is treated by using a slightly higher wavelength LED (475 nm to 490 nm) to reduce the level of bilirubin.
The Arduino board will receive the value from the photodetector and the voltage value will be converted and the digital value of the bilirubin should be obtained. The digital value should be compared with the predefined value and if the obtained value exceeds the predefined value, treatment process should be turned on to decrease the level of bilirubin value in blood, and two channel LCD array used to display the level of Bilirubin. This connectivity solution gives the status to doctors using IOT technology and is used to report the infants’ birth and death reports to World Health Organization (WHO), based on gestational age instead of weight of infants. The overall IOT enabled framework of CliNicS is represented in Figs 1 and 2.
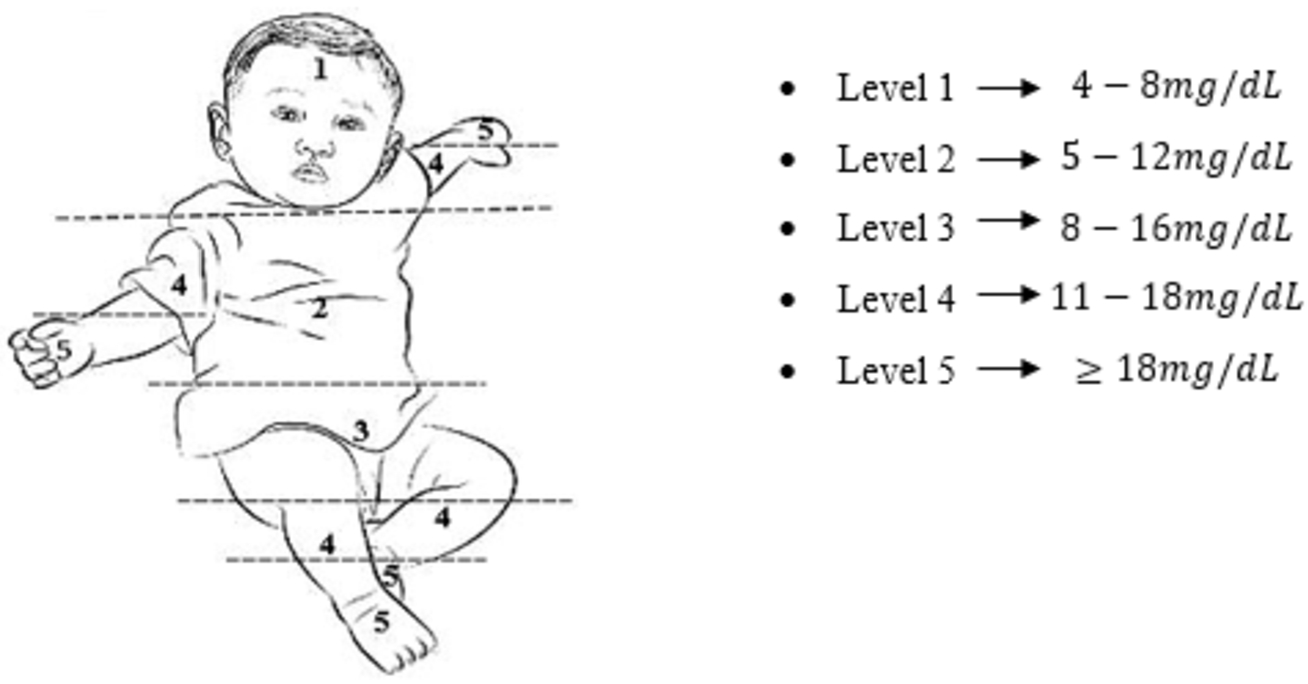
Bilirubin levels classification using Kramer’s rule.
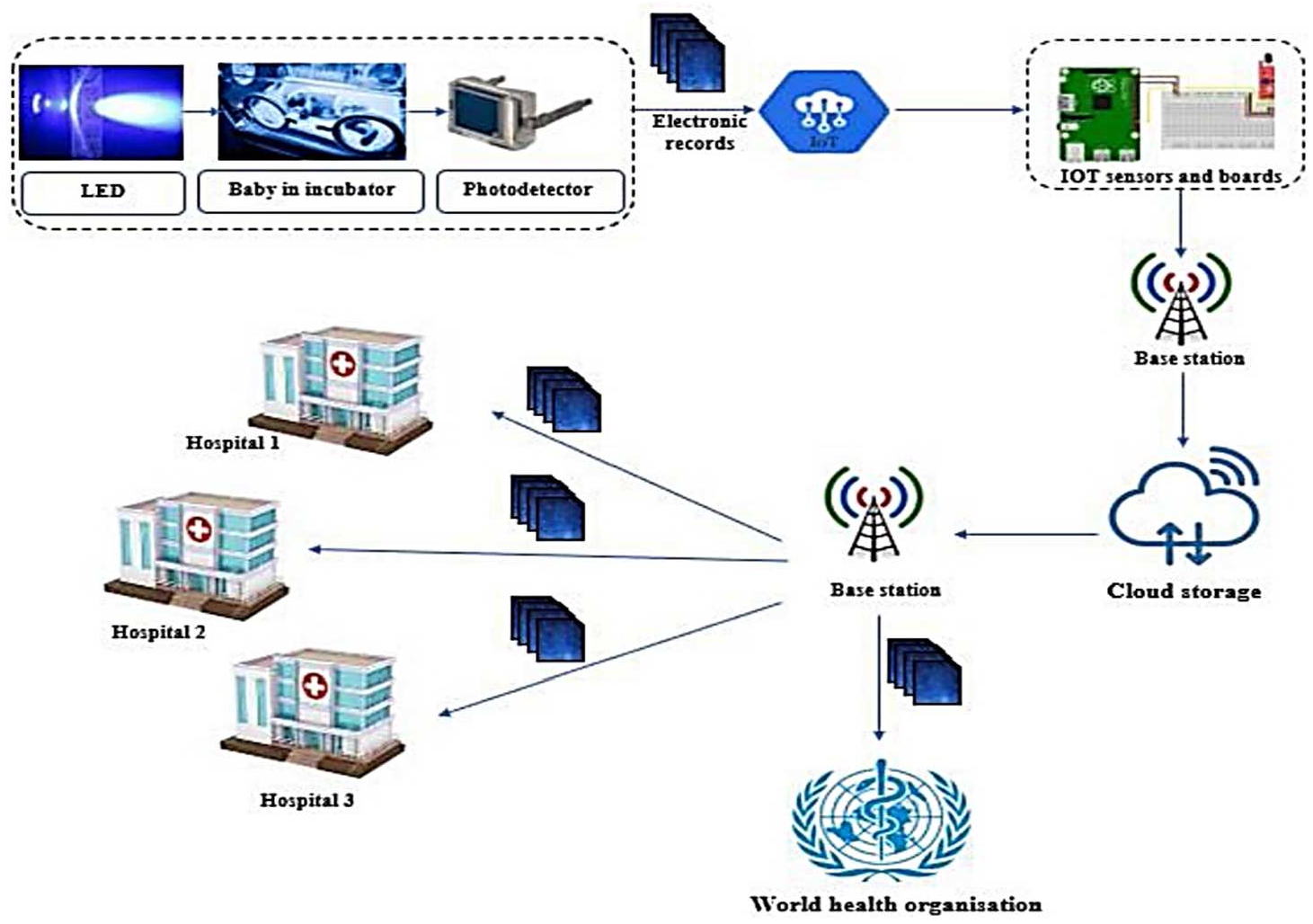
Overall structure of CliNicS.
CliNicS setup has a Length 30inch (707 mm), Breadth 17inch (444 mm) and Height 51 inch (1285 mm). In this study, CliNicS starts by emitting blue light directly onto the newborn’s skin through an LED. Based on the light that is reflected from the skin, the photodetector monitors voltage. After the voltage value was provided, the Arduino Uno analyzed it to determine the bilirubin content. Following that, the Arduino Uno sends a digital signal to the microcontroller. The digital signal at this point is being processed to display the bilirubin level in the LCD display, and the data will be sent to physicians in hospitals and health care organizations through the IOT network.
LED
A LED is chosen for the proposed method because it can last for a long time and consume little power, and its light spectrum is concentrated in the blue region, it produces less heat and is able to be placed near the baby. Traditional phototherapy light treatments may cause skin damage when utilized with conventional UV radiation. With LEDs, the chances of skin damage are reduced as well. Bilirubin absorption occurs between wavelengths 427 and 473 nm, based on spectral light absorption. Melanin and hemoglobin, the other components of the circulation, absorb light between 527 nm and 532 nm, and 620 nm to 720 nm, respectively. Therefore, the bilirubin concentration was determined using blue light with a wavelength range of 410 nm to 460 nm. The irradiance for LED is calculated by using the following equations.
In the above relationship, the computed radiation is greater than the American Academy of Pediatrics’ recommendation (AAP). According to APP1, the optimal quantity of radiation delivered by phototherapy gadgets is above 30 W/cm/nm 2, and the lights utilized in the study fall within this range.
Photodetector
A PIN photodetector with fast speed and high radiant sensitivity, the BPW34 is used for detecting the light. When placed opposite the LED source, the photodetector detects light passed through the infants and however, in a reflectance manner, the photodetector detects light backscattered or reflected from bone, blood vessels, or tissue. LED and photodetector position influence signal quality and strength to motion disturbances during design. In order to improve sensor performance, it is therefore necessary to identify suitable measurement sites. The characteristics of photodetector is represented in Table 1.
Features of photodetector
Features of photodetector
In order to construct the detection systems, it is used the analog-to-digital converter (ADC) of the ARDUINO UNO board. In the Arduino board, pins A0 through A5 have an ‘A’ in front of their designation to indicate that they can read analog voltages. An analog signal terminal was attached to pin A4 on the Arduino Uno microcontroller. Using the ADC Eq. (4), digital data can be converted from analog signals.:
The data will then be transmitted to calculate the bilirubin concentration using Eq. (4). A final transmission was made through the IF block to display the bilirubin value. In the following stage, the output value of a specific bilirubin value will be allocated as a digital value (High = 1). Next, find the value of the threshold. When it is higher than the typical value, LCT is initiated.
Determination of hyperbilirubinemia using clinics
The determination of hyperbilirubinemia and the application of LED controlled therapy is illustrated in Fig. 3.
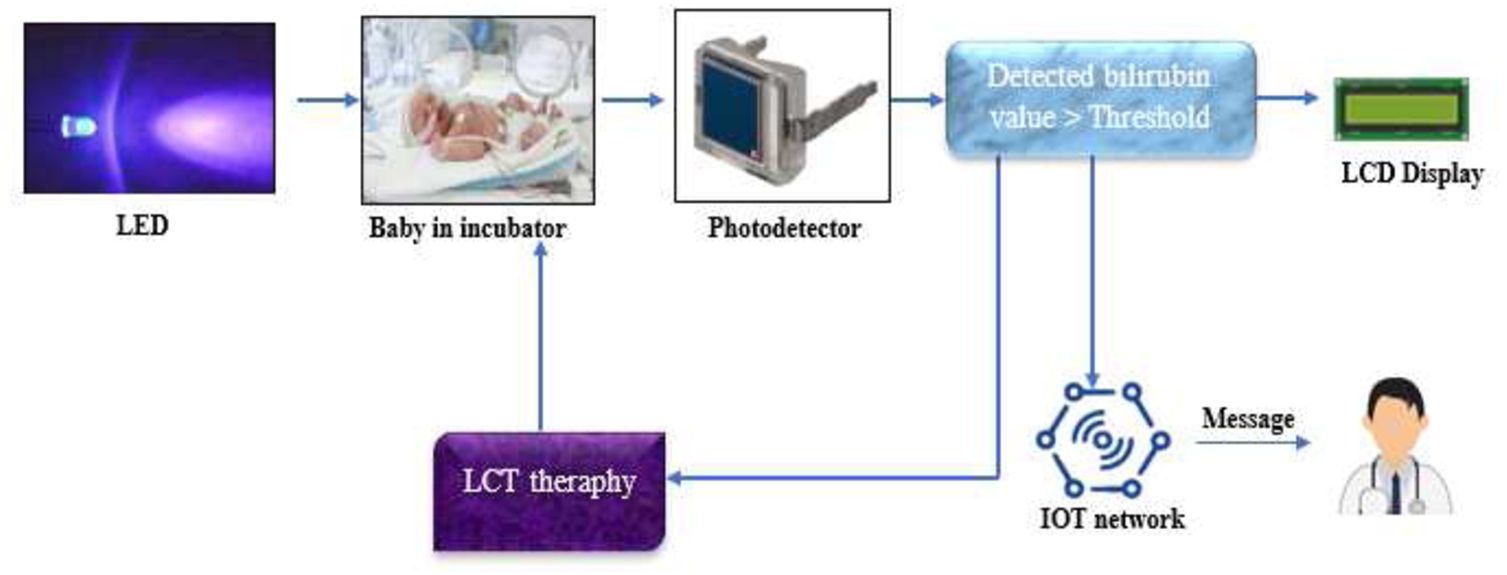
Hyperbilirubinemia detection and treatment process.
Clinicals offers a non-invasive bilirubin monitoring device as well as LCT treatment. In LCT therapy, blue LEDs whose wavelength ranges from 460 nm to 490 nm are used. CliNicS continuously monitors newborns and provides the most accurate bilirubin levels. The proposed LCT algorithm computes the decision factor based on the newborn’s immediate bilirubin level, post-gestational age, and weight. This decision factor controls the (460 nm–490 nm) LED arrays and the amount of therapy. Health institutions are alerted about the state of infants using IoT technology, as well as births and deaths. There will be very little infrared light and no ultraviolet light from this device.
According to the new born baby’s postnatal age and the chance of bilirubin neurotoxicity, a range of total bilirubin levels is used to determine bilirubin neurotoxicity risk. It is expected that the clinical impact of LCT therapy will be observed within 1–2 hours with a decrease of serum bilirubin concentration of over 2 mg/dL (34*mol/L). The accuracy of LCT is measured by continuous bilirubin measurements; the accuracy of these measurements is critical due to the abrupt rise in bilirubin concentration (rebound) when LCT is stopped. The suggested LCT technology reduces the need for a doctor’s presence and enables more precise decision-making.
Remote monitoring
A modernized healthcare system has become essential in the current situation. The use of IoT in the medical industry will aid management in making more informed decisions and reducing costs. By using CliNicS approach, the remote monitoring can be done because it incorporates IOT technology. The Internet of Things architecture in this proposed method consists of five layers. The IOT boards, and sensors that collect data are found in the perception layer, which is one of the five layers. The second layer is the preprocessing layer, which contains the microcontroller and the third layer is the network layer which contains the wifi network protocol that connects the devices to the internet. The fourth layer has the storage layer which uses cloud storage. Furthermore, the information is handled by the application layer which is the fifth. As a result of the coupling of IoT with healthcare systems, clinicians can easily access sensor data from the cloud and remotely monitor the health of patients. Electronic health records may also be delivered to health organizations using IOT technology.
Results and discussion
In this study, 27 neonates were enrolled, and their statistical features are outlined in Table 2. Based on gestational age, birth weight, or postnatal age, there has been no substantial variation in categories. Total Serum Bilirubin (TSB) is a blood test that evaluates the quantity of bilirubin in the body. On the basis of a TSB value of 14 mg/dL, neonates are divided into two groups. When bilirubin levels reach 14 mg/dL, additional investigation and therapy are initiated. TSB values varied from 3.2 mg/dL to 19.9 mg/dL in all the neonates, with seven having TSB levels above 14 mg/dL.
Characteristics of selected neonates
Characteristics of selected neonates
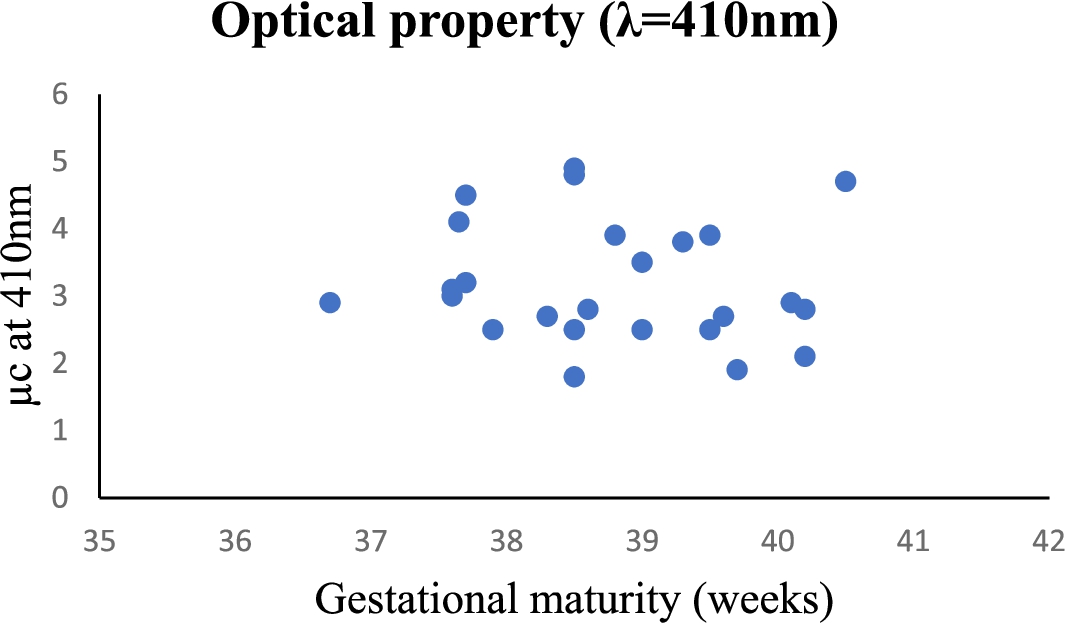
The thickness of a neonate’s skin is related to gestational maturity. According to research, the relationship between TcB (Transcutaneous Bilirubin) and TSB is altered by skin maturity. To evaluate the level of bilirubin in a child’s blood without using a needle, transcutaneous bilirubin (TcB) measurement is an option. Figure 4 shows the dependence between μb at 410 nm on gestational maturity of 27 neonates. This may be due to identical skin structure among infants studied as s’ at 460 nm shows little association with gestational maturity. The adsorption and decreased dispersal factors of infants selected in this research were found to be larger and lower, respectively.
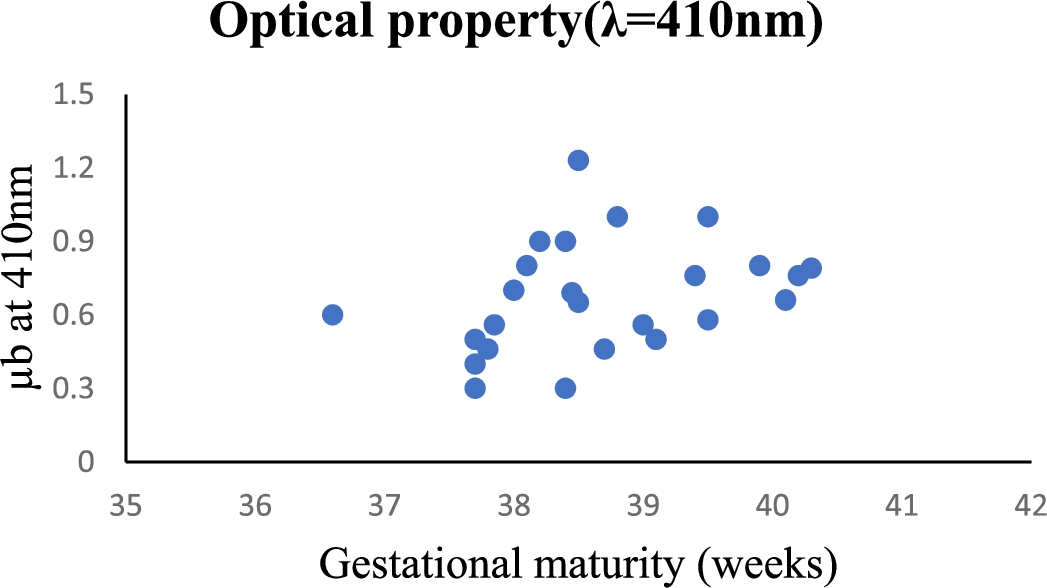
Optical properties μb vs gestational maturity at
Optical properties μc vs gestational maturity at
Figure 5 shows the dependence between
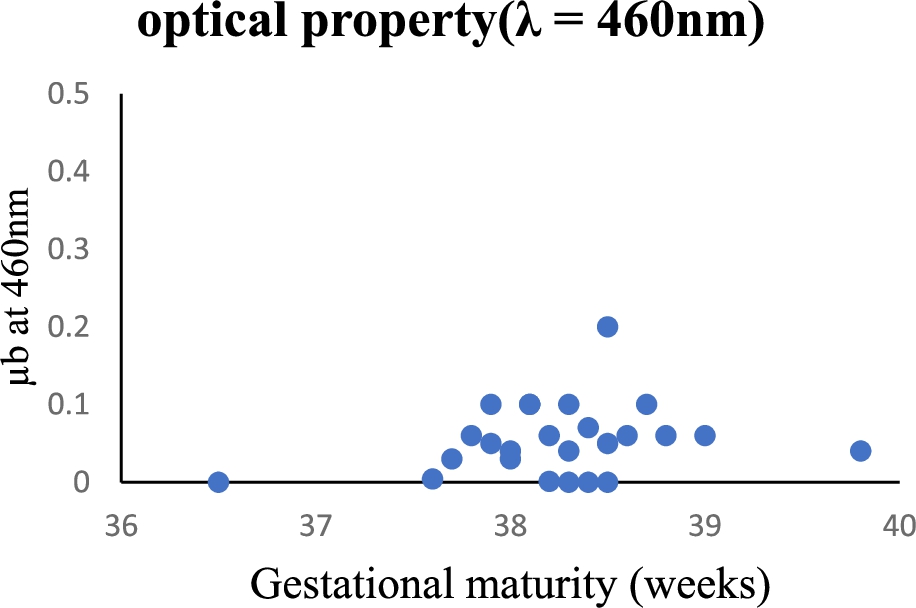
Optical properties μb vs gestational maturity at
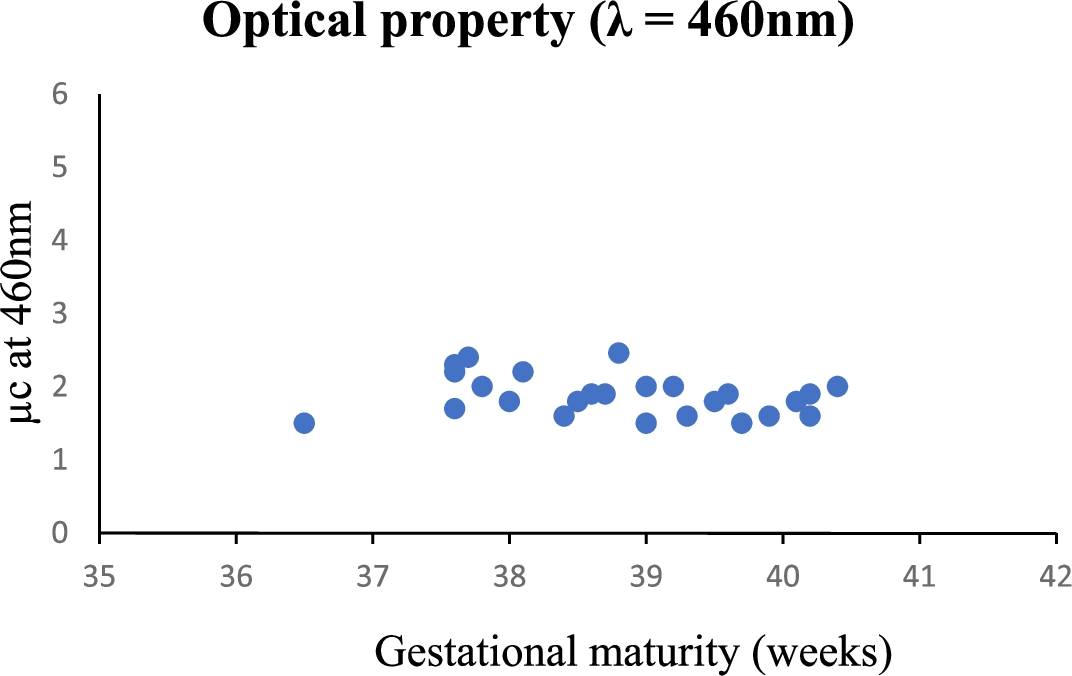
Optical properties μc vs gestational maturity at
Figure 7 shows the dependence between μc and at 460 on gestational maturity of 27 newborns. The total blood bilirubin level dispersion according to gestational maturity. Various factors, including the intensity of light, the distance from the patient of phototherapy, the exposure area, the treatment time, and the quantity of bilirubin in the subject’s body, must be considered to determine the device’s efficiency and effectiveness.
Concentration of bilirubin vs voltage reflection absorbance.
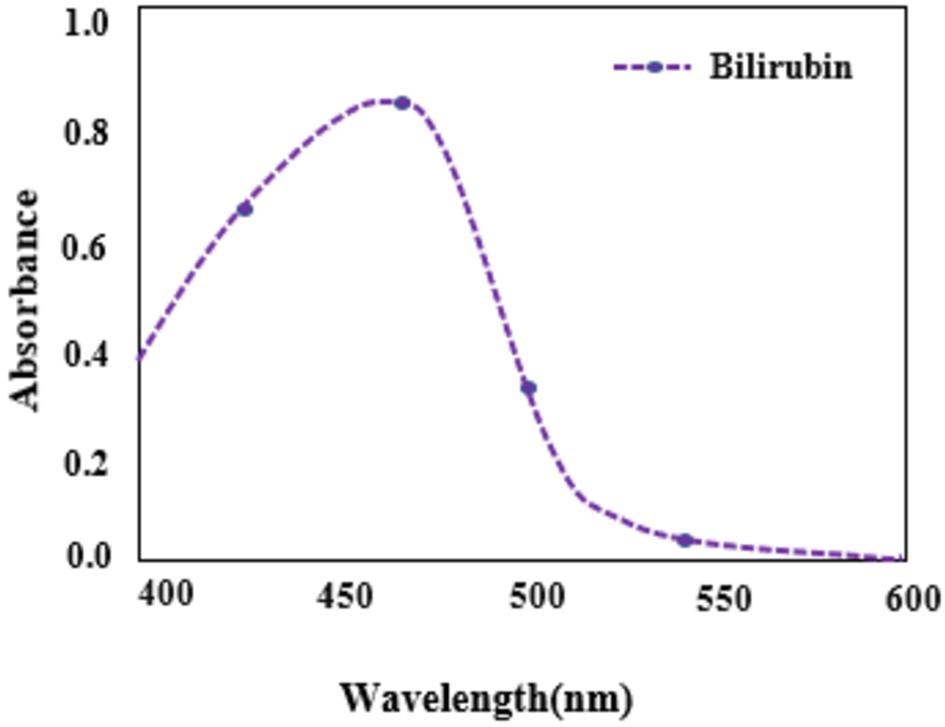
This differential method is justified by the fact that bilirubin concentration is correlated with absorption at 455 nm and is represented in Fig. 8. The majority of babies with hyperbilirubinemia had bilirubin levels greater than 14 mg/dL: 25% of hyperbilirubinemia patients had peak TSB levels greater than 24.9 mg/dL, and 50% had peak TSB levels greater than 29.9 mg/dL (Fig. 9). Birth weight and bilirubin levels did not correlate in this group.
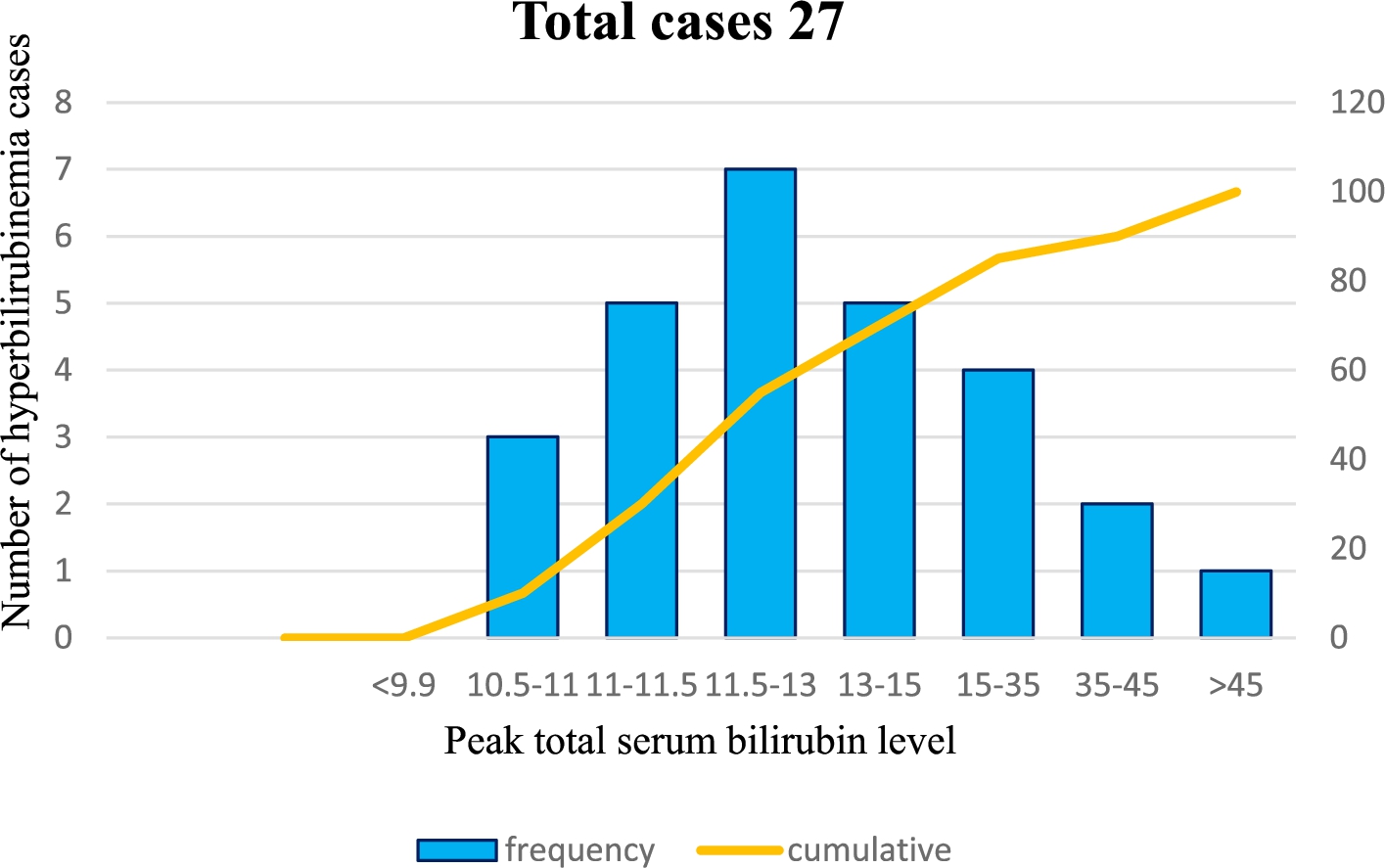
Peak TSB levels in term and pre-term neonates with neonatal jaundice.
Youden’s J statistic yields the maximum which can be used to determine an ideal cutoff threshold (xcut*) that is expressed in the following equation.
The ideal value is
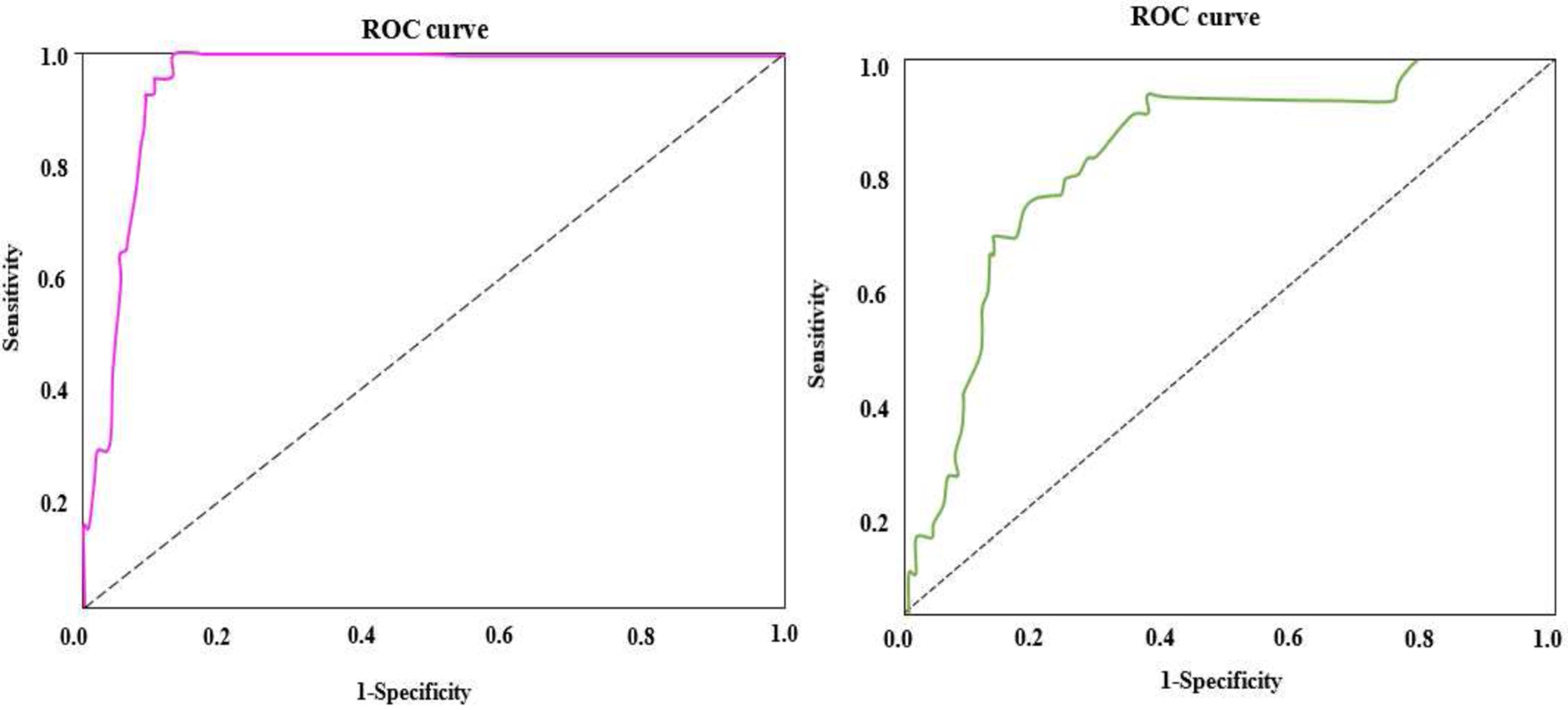
Comparison of ROC curve for total bilirubin and total albumin.
The ROC graph for the total serum bilirubin the total albumin of the neonates is shown in Fig. 10. From the graph, it is understood that it has high accuracy for the bilirubin detection. Table 3 represents the comparison of ROC (Receiver Operating Characteristics) curves for the total bilirubin level and the total albumin level which influence hyperbilirubinemia in infants. Based on this research, the B/A ratio of cord serum predicted the occurrence of severe newborn hyperbilirubinemia. Babies with a total bilirubin level of 1.84 mg/dl in their cord serum were at risk of developing substantial indirect neonatal hyperbilirubinemia. This is the threshold value for predicting hyperbilirubinemia.
Comparison between ROC curves of bilirubin and albumin (in percent)
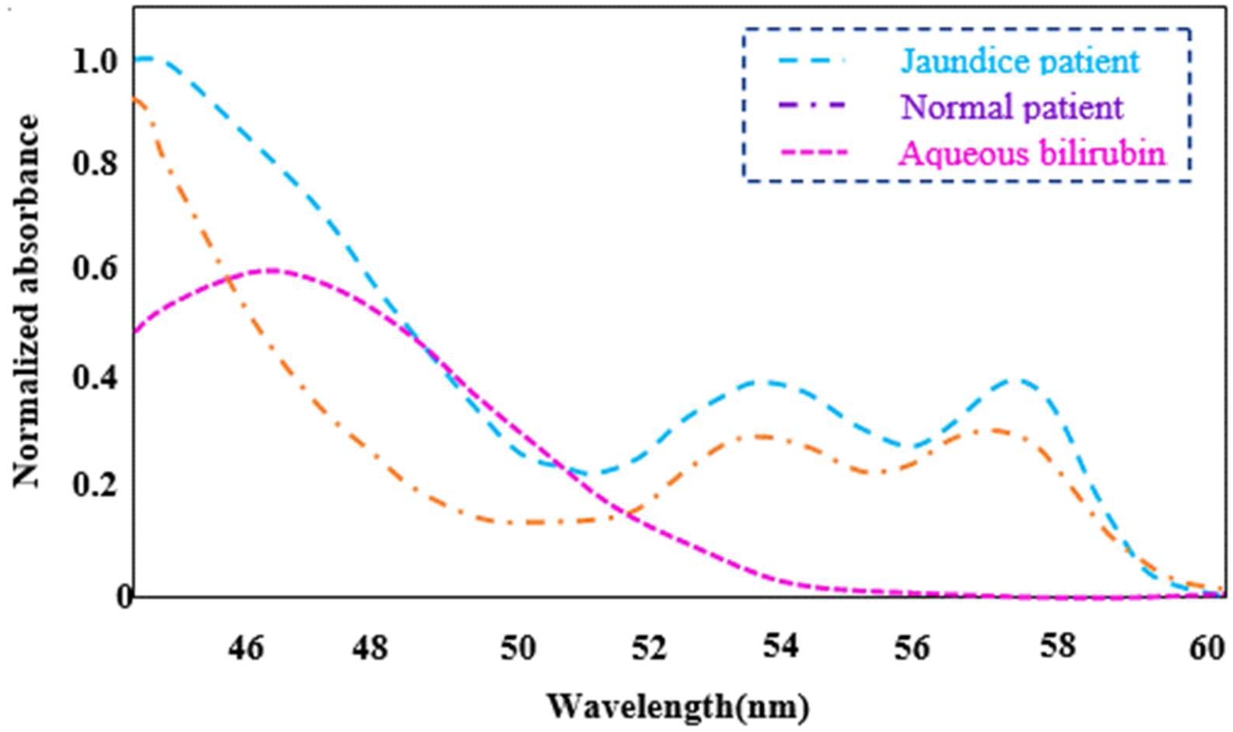
Comparison of a spectral response between a normal and jaundice patient.
A spectral response comparison between a normal and jaundice patient was performed using an LED with a wavelength range of 410–460 nm and is shown in Fig. 11. Patients with jaundice have a greater contribution of yellow pigment to their conjunctiva, which results in a significant variation in spectral appearance. The figure also includes an absorption spectrum of aqueous bilirubin solution.
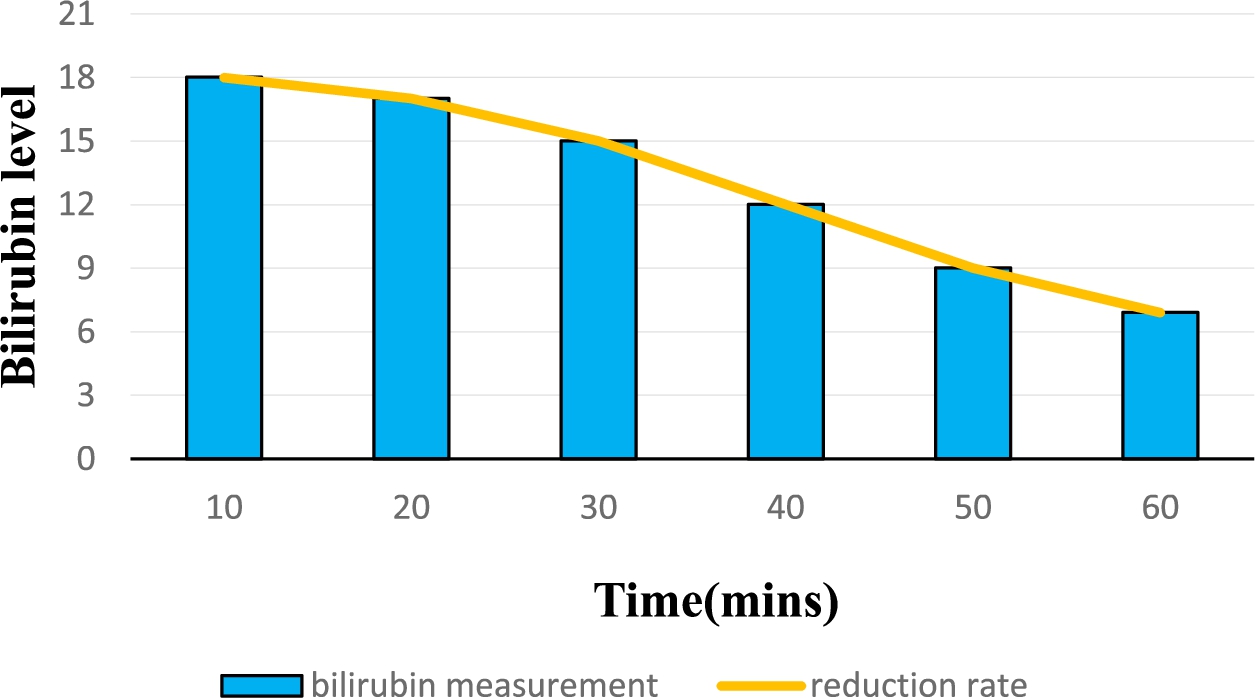
Accuracy of LCT treatment in reducing bilirubin level.
Figure 12 represents the accuracy of the LCT technique which reduces the bilirubin level when the light is passed for 60 mins. From the graph, it is understood that the LCT technique reduces the hyperbilirubinemia of new born effectively.
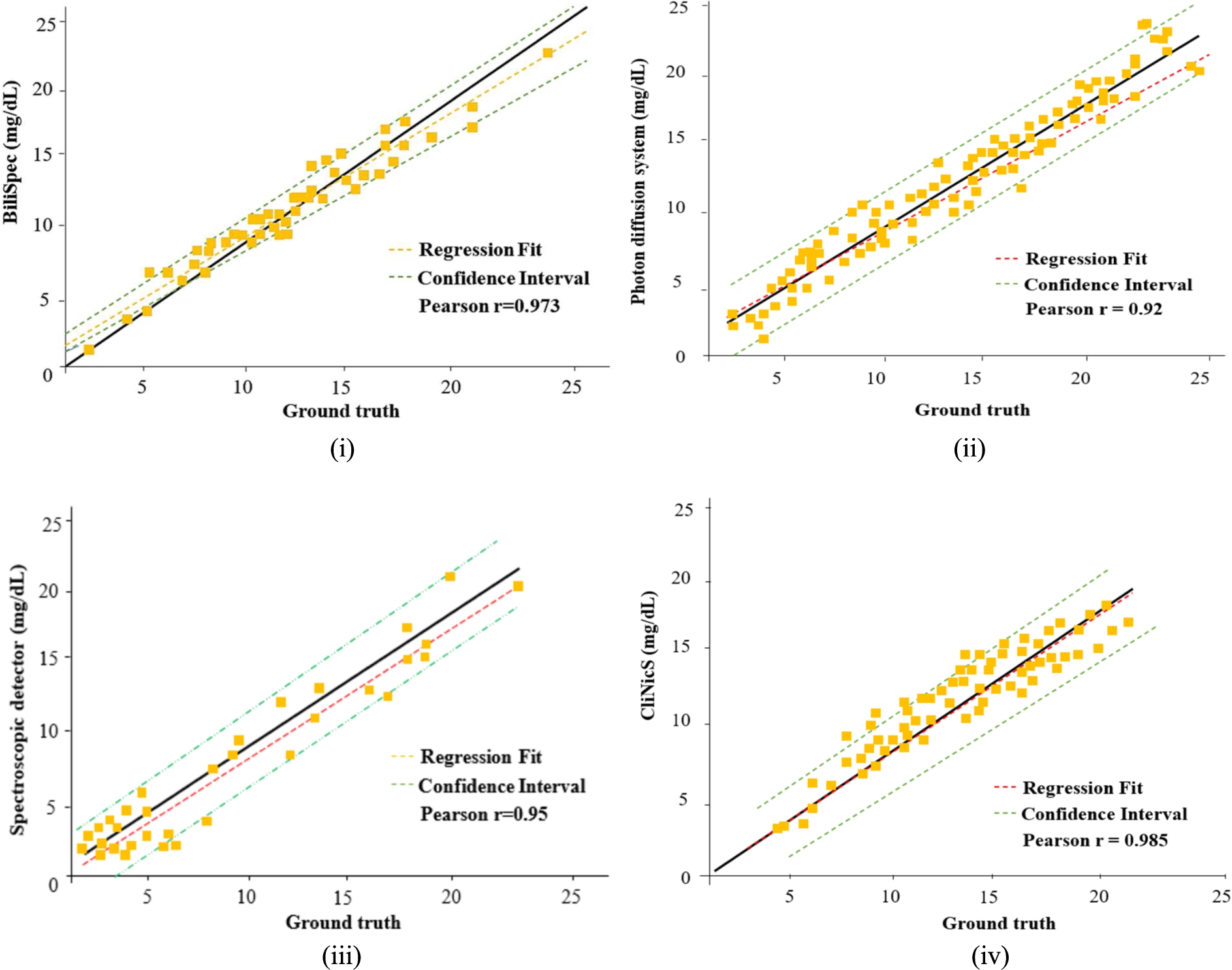
Comparison of correlation between existing and proposed CliniCs.
Figure 13 represents the comparison of correlation between the existing methods such as BiliSpec, Photon diffusion system, spectroscopic detector and the proposed CliNicS technique. Figure 13(i) represents the correlation between TSB levels measured in the test set using BiliSpec and a ground reference. The instrument index values maintain a linear relationship with the TSB values obtained from BiliSpec measurements. Both correlation coefficients were the same in the presence or absence of measurements. There was a strong correlation between TcB levels and TsB levels across the entire cohort. Figure 13(ii) represents the correlation between TSB levels measured in the test set using Photon diffusion system and a ground reference. The instrument index values maintain a linear relationship with the TSB values obtained from Photon diffusion system measurements. Figure 13(iii) represents the correlation between TSB levels measured in the test set using Spectroscopic detector and a ground reference. When compared to TsB, the mean SD shows that TcB overestimates bilirubin levels. Figure 13(iv) represents the correlation between TSB levels measured in the test set using proposed CliNicS and a ground reference. According to the results, the whole blood bilirubin measurements made using the photon diffusion system and the CliNicS method demonstrated a strong correlation with a mean bias of 1.0 mol/L. A mean bias of −4.4 mol/L and a 95% confidence interval of −29.90 to 21.10 mol/L indicated that the spectroscopic detector had been statistically underestimated. The correlation regression for the proposed CliNicS system is 0.985, and the existing system such as BiliSpec, Photon diffusion system, spectroscopic detector is 0.973, 0.92 and 0.95. From the figure, it is understood that the proposed CliNicS system achieves strong regression.
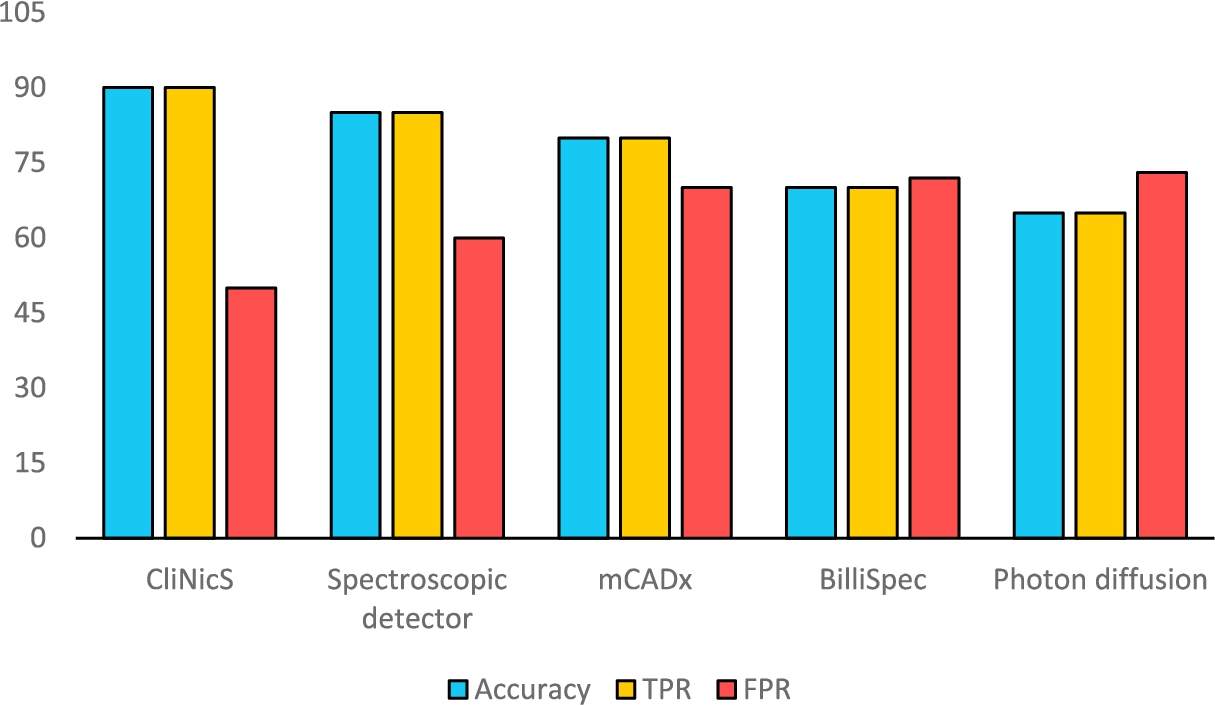
Comparison of proposed CliNicS approach with existing methods.
Figure 14 represents the comparison for the proposed CliNicS approach with the existing mCADx and BiliSpec method for accuracy, True predictive rate and False predictive rate. From the figure, it is understood that the proposed CliNicS approach provides better accuracy and True positive rate than other existing techniques and reduced false positive rate than existing techniques. As a result, we can conclude that, the CliNicS approach can detect hyperbilirubinemia faster than other methods and can give treatment automatically. With the help of IOT technology, CliNicS approach will send the details to doctors and health organizations with that this method will save the lives of the children.
In this study, the goal was to develop a noninvasive device that could help detect and control neonatal hyperbilirubinemia in its early stages and also support doctors in diagnosing it. In general, the results produced were compared to the standard blood test results for 27 healthy newborns. As a result of the sensitivity of newborn neonates and the courtesy of vessels, our proposed CliNicS technique could be used to detect jaundice non-invasively and at a rapid rate. Based on an evaluation of the system’s processes, jaundice was correctly detected and treated in a short time for 7 jaundiced newborns.
The device was tested on randomly selected 27 neonatal subjects (Table 2), which categorizes neonates into two groups based on the bilirubin level. Additional testing and therapy are started when bilirubin levels reach 14 mg/dL. The TSB levels of newborns ranged from 3.2 mg/dL to 19.9 mg/dL, with seven exceeding 14 mg/dL. Figures 4–7 depict the optical property dependencies on gestational maturity. The effect of b at 410 nm on the gestational maturity of 27 babies is seen in Fig. 4. This could be because all of the infants investigated have the same skin structure, as s’ at 460 nm has minimal correlation with gestational maturity. The differential method is justified by the fact that bilirubin concentration is correlated with absorption at 455 nm and is represented in Fig. 8. Figure 9 shows the peak total serum bilirubin level and it demonstrates that the majority of neonates affected by jaundice have bilirubin levels greater than 29.9 mg/dL. From the ROC graph in Fig. 10, it is understood that the proposed technique has high accuracy in detecting bilirubin. Table 3 represents the comparison of ROC (Receiver Operating Characteristics) curves for the total bilirubin level and the total albumin level, which influence hyperbilirubinemia in infants. The statistical test results are shown in Fig. 12. The statistical test as well as the ROC curve and analysis showed the effectiveness of this system in detecting neonatal hyperbilirubinemia. Then, the proposed system was compared to other methods that included jaundice detection in various ways. As a result, the proposed CliNicS technique has been found to be unique, with better quality and rapid processing time.
Conclusion
In newborns, both invasive and non-invasive procedures can be used to detect bilirubin in the blood. This invasive procedure requires the collection of blood samples from newborns, which is extremely distressing and time-consuming to detect. In order to resolve these problems, a non-invasive procedure was implemented, which is painless and produces results faster than invasive procedures. In this paper, a noninvasive technique called CliNicS has been proposed to identify and treat hyperbilirubinemia in neonates. By using an LED of wavelength 410 to 460 nm and a photodetector, CliNicS effectively determines if the baby has hyperbilirubinemia or not. If hyperbilirubinemia is identified, CliNicS initiates the LCT treatment by turning a blue LED light on with a slightly higher wavelength. IOT technology is enabled for remote monitoring of preterm infants and sending the health records to the doctor and health organizations. In comparison with other existing systems in the literature, the proposed system has several advantages, such as its ability to detect hyperbilirubinemia at TSB levels above 14 mg/dL and its low cost, which makes it ideal to be employed in clinics and health centers without laboratory facilities or trained medical professionals. Newborn jaundice was identified successfully in the initial experiments. Results may be improved by working with more participants in various lighting scenarios and with participants with a diverse range of skin tones in the future.
Conflict of interest
None to report.