
Abstract
BACKGROUND:
Breakage of joint arthroplasty components are rare, yet during an implant retrieval program we found several cases.
OBJECTIVE:
In this study we examined the components to determine the causes and mechanisms of breakage of these implants.
METHODS:
From our collection of 849 retrievals we selected 682 cases with metal parts (503 hip, 79 knee arthroplasties) and identified fractured components: seven hip resurfacing implants, five total hip replacement stems, one monopolar femoral head, and one modular revision femoral stem from. Implants were examined using optical and scanning electron microscopy; metallographic sections were prepared and samples of periprosthetic tissues underwent microscopic examination.
RESULTS:
In the resurfacing components breakage occurred in small stems placed in the femoral neck due to necrosis of femoral heads, with no metal flaws detected. Fatigue breakage of femoral stems was caused by presence of material flaws in the CoCrMo alloy, and corrosion. The monopolar head failed in fatigue fracture mechanism, breakage was initiated in an undercut near the taper connection for femoral component. The modular stem from Ti alloy sustained fatigue fracture induced by corrosion caused by debris from previously revised stem; no material flaws were detected in this sample. In most cases periprosthetic tissues had a morphology typical for aseptic loosening.
CONCLUSIONS:
In our series failure was caused by material flaws, presence of stress raisers and localized corrosion. Our findings indicate that sharp edges and other features which can act as stress raisers should be avoided in newly designed implants. Corrosion induced fracture of the modular Ti stem indicates the need for a detailed debridement of periprosthetic tissues during revision arthroplasties.
Introduction
Fractures of metal implants used in joint arthroplasty are rare complications, since most designs undergo fatigue testing during pre-clinical evaluation [1]. Still, breakage has been reported for various types of components, such as early models of the Exeter femoral stem, which led to modification of implant geometry and change of material used for its manufacturing [2–4]. More recently concerns regarding corrosion induced fractures of modular femoral necks were raised, which ultimately resulted in withdrawal of most designs from clinical use [1,5–10]. It has been suggested that certain patient-related factors such as obesity or high activity level may be associated with implant breakage [1,6,11–13]. However the role of these factors is controversial, since there is a lack of evidence from studies involving large groups of patients.
So far most papers regarding component factures were case reports, which were focused on increasing awareness this complication and served as an early warning against the use of certain designs [4–6,10,14–18]. Many authors did not conduct any structural analysis of retrieved implants and the underlying failure mechanisms were not explored. Little is also known about reactions of periprosthetic tissues in these cases.
This study examined a series of fractured metal components of joint replacements, which were obtained as part of a retrieval program. Samples were inspected in order to determine if their breakage was associated with implant design features and properties of biomaterials used for their manufacturing. Furthermore, samples of periprosthetic tissues were examined for presence of inflammatory reactions.
Materials and methods
This study examined 14 metal components, obtained from 13 patients as part of a retrieval program approved by the local bioethical committee (162/2012). Implants were selected from a collection of 849 retrievals, which included 682 cases where metal components were obtained (503 hip replacements, 79 knee arthroplasties). The following fractured components were included in this study: seven hip resurfacing implants, five total hip replacement (THR) stems (three cemented, two uncemented), one monopolar femoral head, one modular revision femoral stem. Two samples were obtained from the same patient who was revised because of loosening and fracture of a primary stem, and later due to breakage of a revision stem (Table 1). All of the included patients had modest to medium physical activity levels prior to revision with UCLA score ranging from 2 to 6, in all cases BMI was lower than 35.
Short summary of the subjects' data included in the study
Short summary of the subjects' data included in the study
1Indicates components revised from the same patient; 2The following tissue samples were included: FH – femoral head, PT – periprosthetic tissues, FS – bone fragments obtained near the fractured femoral stem; 3Reaction of periprosthetic tissues according to Morawietz scale (Type I-IV); in cases where Type IV was observed, presence of ALVAL was graded according to the Oxford ALVAL scale (Grade 1-3), AVN – avascular necrosis of the femoral head.
Additionally, as reference samples we included undamaged components of the same type and one sample of medical grade cast ASTM F75-12 CoCrMo alloy. This study did not include fractured screws used for fixation of acetabular components, as their failure is a well understood phenomenon secondary to loosening of the acetabular component.
All retrieved components were either sterilized by autoclaving or disinfected by submersion in formalin for 72 hours, washed with soft nylon brush in a mild detergent, photographed and examined using optical microscope. Next samples were observed using scanning electron microscopy (SEM: FEI Inspect S, FEI, Holland; JEOL JSM 6400, JEOL, Japan), elemental composition of samples was determined using energy-dispersive X-ray spectroscopy (EDS; EDAX, USA). Then selected samples were cut using a diamond saw (Buehler Isomet Low speed saw) and metallographic slides were prepared and examined using a metallographic microscope (Eclipse 150, Nikon, Japan) and SEM.
In most cases during the revision procedures samples of periprosthetic tissues were obtained from regions adjacent to the femoral head and sent for pathological evaluation as a routine screening procedure for periprosthetic infections [19]. In patients with resurfacing implants fragments of bone from the femoral head were also obtained; additionally, samples from regions around fractured stems were available in two cases (Table 1). All samples underwent routine processing to prepare hematoxylin and eosin (H&E) stained microscopic slides which were examined by a pathologist at a magnification of 200–400×, using conventional microscopy and polarized light (to detect polyethylene particles). The samples were then evaluated using a histopathological scale, initially developed by Morawietz et al. [19]. Briefly, the scale includes four types of reactions: Type I – reaction to wear particles, Type II – infection, Type III – mixed reaction, Type IV – indifferent type, including fibrosis as well as lymphocytic infiltration. If lymphocytic infiltrations were present (lymphocyte-dominated vasculitis associated lesion - ALVAL), samples were additionally evaluated using Oxford-ALVAL scoring system [20] (Grade 1: less than 5 lymphocytes around vessels, Grade 2: 5–10 lymphocytes, Grade 3: more than ten lymphocytes).
Based on the implant type, data from patients' history and preoperative findings, three main groups of components were distinguished in this study: resurfacing implants, cast CoCrMo stems and the remaining components.
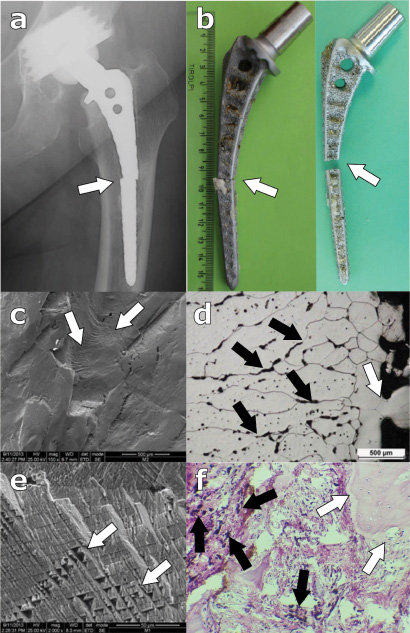
The femoral components of the Durom system included in this study (Fig. 1a) consisted of two parts: the femoral cap and a thin stem, which facilitates implantation and contributes to load transfer in vivo (Fig. 1b) and was manufactured from wrought-forged high-carbon content CoCrMo alloy (Co-28Cr-6Mo 0,20-0,25%C). The stem was pressed into the spherical part by means of a taper connection (Fig. 1b,c), which was tight only in its deeper part (Fig. 1c). In all retrievals fractures occurred at the junction between the stem and the cap (Fig. 1d,e). Optical and scanning electron microscopy demonstrated a typical pattern seen in fatigue fractures – a portion of the fractured stem showed signs of polishing, while the reminder was matt; breakage occurred in an area where the stems diameter was sharply decreased in this area (Fig. 1d,e,f). Metallographic studies did not demonstrate any material defects or presence of corrosion in the fractured stems, material porosity was also very low (below 1%). In some cases small cracks were visible near the area where fatigue fracture was initiated (Fig. 1f). In all patients failure was associated with avascular necrosis of the femoral head (AVN), which had a characteristic appearance seen during revision surgeries and was confirmed in histological studies (Fig. 1g). Periprosthetic tissues around the implants exhibited presence of fibrotic (type IV) or inflammatory (Type 1) reaction with a small number of macrophages and very few metal particles (Fig. 1h). Mild perivascular lymphocytic infiltrations (Grade 2 ALVAL reaction), suggesting adverse reaction to metal debris was present in three cases.

Breakage of the Durom hip resurfacing components. a. Typical radiographic appearance with migration of the cap (arrow); b. Disassembled Durom femoral components. Black arrow indicates the stem, the white arrow its receptacle on the femoral cap; c. Cross-section of the taper connection of an assembled component. Arrows indicate the superficial part where the stem was not tightly engaged into the cap; d. Breakage site – view from the inner side of the cap. Arrow indicates crack initiation site; e. Breakage site at the stem. Arrow indicates that the fracture occurred below the undercut of the stem; f. SEM image of a metallographic section of a fractured component. The white arrow indicates the area of the breakage, the black arrow indicates fatigue cracking of the stem; g. Microscopic slide of a bone fragment from the femoral head with features typical for avascular necrosis. Arrows indicate “shadows” of necrotic cells; h. A typical morphology of periprosthetic tissues seen in most Durom cases. Arrows indicate small vessels with no lymphocytic infiltrations.
At revision of the fractured uncemented Autophor stems, their proximal parts migrated moderately, while distal parts beneath the breakage areas were still attached to the bone (Fig. 2a,b). These components were cast from CoCrMo alloy, had a square profile with pronounced corners and featured sintered beads on their surface to allow osseointegration (Fig. 2b). In microscopic studies evident signs of fatigue fracture of both stems were seen. SEM studies revealed characteristic striations corresponding to crack initiation sites near sintered beads (Fig. 2c). Metallographic studies of these presence of multiple small voids in both the retrieved and unused stems, so that the porosity of the alloy was in the range of 5–10%, as opposed to less than 1% found on the reference ASTM F75-12 sample. In retrieved components the pores contributed to propagation of intragranular corrosion and cracking arising from junctions with sintered beads (Fig. 2d). Areas adjacent to striations exhibited signs of brittle fracture with the crystalline structure of the alloy visible in SEM studies (Fig. 2e). Periprosthetic tissues obtained from regions around the articulation demonstrated fibrosis with presence of small clusters of macrophages loaded with metallic debris (type I reaction), while bone samples from region adjacent to the breakage site contained fragments of fibrous tissue with macrophages (type I reaction) containing metallic debris (Fig. 2f).
Breakage of the Autophor stems. a. Radiographic appearance. Arrow indicates the breakage site; b. Retrieved components. Arrows indicate breakage sites; c. SEM image of a fracture site near the corner of a stem. Arrows indicate fatigue striations; d. Metallographic section of an area near the breakage site. White arrow indicates corrosion at the junction site with the sintered bead, black arrows indicate propagation of cracking and corrosion through pores; e. Area of brittle fracture with crystalline structure of the alloy well visible (arrows); f. Fragment of tissues obtained near the breakage site. White arrows indicate trabecular bone, black arrows indicate macrophages loaded with metal debris.
The Weller monobloc cemented stems cast from CoCrMo fractured at the distal parts, and subsided in the cement mantle due to loosening (Fig. 3a,b). These stems featured a square profile with rounded edges, and had a satin finish to allow good cement fixation (Fig. 3b). In the retrieved samples component migration and micromotions resulted in polishing of the breakage areas (Fig. 3c). Similarly as in the Autophor stems crack initiation sites were found near rounded corners (Fig. 3d), and the porosity of the cast alloy was increased (Fig. 3e). Despite polishing of the fracture sites, remnants of fatigue striations were still visible in SEM studies (Fig. 3f). Periprosthetic tissue samples from these patients obtained near the articulating surfaces contained giant cells (Fig. 3g) with multiple polyethylene debris visible sin polarized light (Fig. 3h), which is typical for aseptic loosening (Type I reaction). Samples from regions adjacent to the breakage were not available.
Breakage of the Weller stems. a. Radiographic appearance. Arrow indicates the breakage site; b. Retrieved component. Arrows indicate breakage sites; c. Breakage areas exhibiting polishing of their surface. Crack initiation site visible near one of corners (arrows); d. SEM view of the crack initiation site (arrows); e. Metallographic section of the alloy near the breakage area. Multiple pores (indicated by arrows) visible; f. SEM image of the polished part of a breakage area. Arrows indicate remnants of striations; g. Sample of periprosthetic tissues obtained near the bearing surface with multiple giant cells (arrows) visible. Sample classified as type I; h. Tissue sample from Fig. 3g viewed using polarized light. Arrows indicate PE debris well visible in these conditions.
The fractured monobloc femoral head included in this study (Fig. 4a) was made of two elements cast from CoCrMo alloy with increased (3–5%) porosity: the spherical part and the part intended for taper for connection with the femoral stem (Fig. 4b,c). Both parts were fitted together by means of a press-fit connection (Fig. 4b,c). The fracture of our implant occurred within the lower part of the element intended for taper connection, near an undercut (Fig. 4c,e); the area where both elements forming the head joined remained undamaged. SEM studies of retrieved components demonstrated features of fatigue failure, with presence of cracking at the element intended for taper connection, surrounded by areas exhibiting features of brittle fracture (Fig. 4f). Metallographic studies of the CoCrMo alloy used in both components demonstrated increased (3–5%) porosity (Fig. 4g) of the material. Periprosthetic tissues were characterized by presence of a small number of macrophages, with a large number of metallic debris (Fig. 4h).
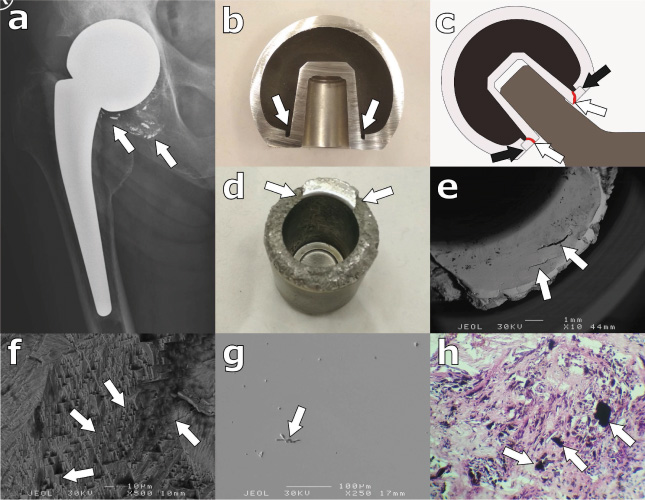
Breakage of a monoblock femoral head. a. Radiographic appearance. Arrow indicates area where metallic debris were present; b. Cross section of the component. Arrows indicate undercuts near the taper connection; c. Schematic diagram demonstrating where the fracture of the head occurred (white arrows, red cracking marks). Note that the part intended for taper connection was press-fitted into the head in areas indicated by black arrows; d. Gross view of the broken taper part. Arrows indicate areas where the brittle fracture occurred; e. SEM image of the part intended for taper connection. Arrows indicate fatigue cracking of this part; f. SEM image of the part of the taper connection where brittle fracture occurred; g. SEM image of a metallographic section of the alloy near the breakage site. Arrows indicate small pores; h. Microscopic slide of periprosthetic tissues around the fractured implant. Arrows indicate metallic debris of various sizes.
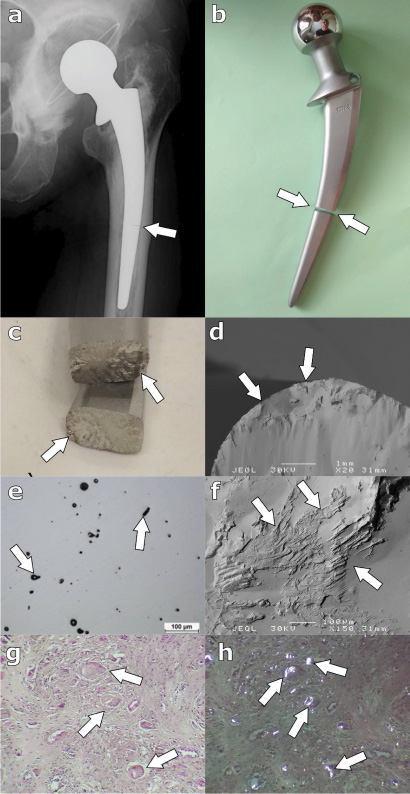
A different failure mechanism was observed in case of the modular revision stem manufactured from forged TiAl6V4 alloy (Fig. 5a). This component was implanted in one of patients which was earlier revised because of breakage and loosening of an Autophor stem and showed localized signs of corrosion on the surface of the implant visible as dark bluish spots (Fig. 5b,c). Similar spots were present in two areas of the breakage surface; the discolorations exhibited characteristic striations (Fig. 5c). These marks were most likely caused corrosion caused by contact with metal particles released from the previously implanted prosthesis, although using EDS we were unable to demonstrate presence of CoCrMo alloy residues. SEM studies demonstrated crack initiation sites near within corrosion marks, polishing of some grains near crack initiation sites (Fig. 5d). Signs of brittle fracture with partial pull-out of grains and intergranular cracking were visible in other parts of the breakage surface (Fig. 5e). Metallographic studies of this implant did not demonstrate presence of localized defects, material porosity was below 1%. Periprosthetic tissues in this patient contained clusters of macrophages loaded with metallic, and PE debris (Fig. 5f).

Breakage of the Restoration revision stem. a. Radiographic appearance. Arrow indicates the fracture site; b. Macroscopic view of the fractured implant. Arrow indicates the breakage area; c. Corrosion marks on the femoral neck indicated by arrows; d. SEM image of the crack initiation site of the component (black arrow). White arrows indicate areas where grain polishing was observed; e. Brittle fracture of the remainder of the neck. Arrows indicate intergranular cracks; f. Microscopic slide of the periprosthetic tissue sample. Arrows indicate clusters of macrophages loaded with metallic debris.
Breakage of metal components in joint arthroplasty is a relatively rare complication and most literature available on this topic are medial case reports, which did not investigate the mechanisms of implant failure [4,6,10,12,14,15,21–24]. Some of these papers identified material flaws and specific design features, such as modular necks in THR as main causes of failure [1,7,8,11,25]. In this study we examined a series of fractured metal components obtained as part of a retrieval program and found that breakage typically occurred in fatigue mechanism and was more common in implants from CoCrMo alloy. Fractures were caused by local overload, material flaws, stress raising features of implant geometry and corrosion. Examination of periprosthetic tissues suggests that breakage was a secondary phenomenon related to aseptic loosening or AVN of femoral heads in resurfacing components.
This study is limited in several ways, predominantly due to a small number of examined samples which do not represent well-functioning implants. This limitation is an inherent feature of all retrieval studies, and most other papers regarding implant breakage also included small number of samples [1,5,6,10,11,16,18,20,26]. Although a detailed examination of all retrievals was conducted, fracture sites of some samples, especially the Weller stems were damaged due to implant micromotions. Consequently studies of these implants have a limited accuracy, as features which could more precisely indicate failure mechanisms were most likely lost. In recent years much attention has been paid to fractures of modular necks in THRs [1,5–8,11]. Examination of such components would be very interesting, however since they were never used in our institution we obtained only three samples (with no breakage cases) from patients referred from other institutions for revision surgeries. Some of conclusions regarding failure modes of retrieved components were based on examination of periprosthetic tissues, however data from these samples alone is insufficient to determine the failure mechanism, as a given histological pattern may be associated with various biomechanical conditions [9,19,20,24,25]. Similar limitations apply to radiographic evaluation of the implants, as retrospective analysis of the radiographs did not allow a precise identification of the breakage event in most cases.
The largest group of implants included in this study were Durom hips. In these components a common failure pattern was observed – breakage occurred in the undercut region of each stem, which acted as a stress raiser and crack initiation site. In these components breakage occurred as a secondary phenomenon related to aseptic loosening or avascular necrosis of the femoral head. In resurfacing implants AVN results from damage to the vascular network supplying the femoral head during implantation of the metal cap [27,28], and is a common cause of early failure as documented in multiple studies [4,13,27,28]. As the bone underneath the femoral component became necrotic and soft, loads applied to the articulating part caused fracture of the short Durom stem and subsequent migration of the cap. Typically such cases are not associated with formation of pseudotumors, and this was the case in the present study as confirmed by histological studies [20,26–28].
The cast CoCrMo alloy stems fractured as a result of implant loosening. In case of the Weller stems progressive osteolysis and deboning from bone cement in the proximal femur resulted in overloading of the distal part which was still attached to the cement mantle, as reported for other cemented designs [2,3]. In our Autophor retrievals a similar mechanism was observed - proximal osteolysis caused fracture near the well-fixed distal part. Such failure mode has been described in other studies regarding this type of stem [17]. These findings were consistent with histology of periprosthetic tissues, which exhibited inflammatory reactions to wear debris, especially pronounced in patients with the Weller stems [19,20]. It should be noted that certain features of implant geometry, such as pronounced corners and sintered beads contributed to failure of these implants, since they acted as stress raisers and crack initiation sites [1,23,25]. Additionally increased porosity of the alloys and in case of the Autophor stem corrosion arising from junctions of sintered beads also weakened the material [2,22]. Similar mechanisms contributed to failure of the monobloc femoral head. Suboptimal design of this implant featured an undercut around the taper connection which acted as stress raiser; the material was also weakened by increased porosity. It should be noted that monobloc heads are aimed at low demand, inactive patients. Failure of such component in absence of severe overload or trauma is alarming.
Fracture of the modular titanium revision stem seems to be a consequence of material corrosion related to presence of metal debris from the previous revision surgery. Such corrosion induced fractures have been widely described in modular THRs with CoCrMo necks and femoral stems manufactured from titanium alloys [1,5–7,10,11,15,16,22,23,25,29]. It was demonstrated that such components fretting corrosion at the stem – neck junction initiates material erosion, cracking and subsequent fatigue fractures of both CoCrMo and Ti alloy components [5,6,11,14,16,23]. A similar mechanism was most likely involved in our study, since the retrieved component demonstrated evident signs of localized corrosion. This is partially consistent with findings from pathologic examination of periprosthetic tissues, which contained metallic debris, in contrast to ALVAL reactions commonly seen in such cases [16,20,25,26]. However, it should be underlined that since the previous implant also fractured in this patients, it is not possible to determine to which extent debris from the modular revision component contributed to the inflammatory reaction [19].
It should be also noted that our EDS analyses did not demonstrate residues of material from the previously retrieved stem, which was most likely related to limited sensitivity of this method. Application of more sensitive analytical techniques would also have limited validity, due to artifacts and scratches caused by surgical tools and metal debris released after breakage. It should be however underlined that all previously published studies regarding corrosion-induced implant fractures included EDS examination only to confirm the composition of the alloy, and not to detect corrosion products; we are therefore unable to verify our methodology [1,14,22].
Other authors who examined fractured implants indicated that breakages related to corrosion of components were often associated with formation of pseudotumors, and presence of pronounced perivascular lymphocytic infiltrations (ALVAL) [8,9,14,16,19,20,26]. In this study no pseudotumors were observed, periprosthetic tissues obtained from areas near breakage sites contained macrophages loaded with metallic debris, while samples obtained near bearing surfaces had features typical for aseptic loosening (type I reaction, presence of macrophages), or avascular necrosis of the femoral head (Durom cases) [19,20]. Mild ALVAL (Grade 2) was seen in some Durom cases, however it is likely that this reaction was associated with wear of their bearing surfaces, as demonstrated by other authors [19,20]. These findings are consistent with studies of retrieved femoral stems, which demonstrated that most of them failed due to overload associated with progression of osteolysis and implant migration.
Some authors have previously suggested that certain patient-related parameters, such as severe obesity and high levels of physical activity, could be associated with increased risk of implant breakage [1,4,6,11–13,26]. Since we included samples from a small cohort, we are unable to conduct meaningful statistical analysis how such parameters affect the risk of breakage. Additionally none of our patients were severely obese or participated in high-impact activities. It should be however underlined that to date there are no studies which could identify patient-related risk factors of implant breakage based on datasets from large group of participants.
Conclusion
Our study demonstrated that implant breakage is a rare complication of joint arthroplasty. We found that in most cases it occurred in fatigue fracture mechanism as a phenomenon secondary to implant loosening or avascular necrosis of the femoral head in case of hip resurfacing components. Presence of material defects and stress raisers such as sharp edges or undercuts in implant material may promote component breakage and we conclude that such features should be avoided in newly designed implants. We also found evidence, suggesting that presence of metal debris released from loose implants has the potential to initiate corrosion induced fatigue fracture of revision components. This indicates the need for meticulous debridement of periprosthetic tissues from metal debris during revision procedures.
Footnotes
Acknowledgements
This study was supported by a grant from the Polish National Science Center (DZ 2012/05/D/NZ5/01840).