
Abstract
BACKGROUND:
Cervical radiculopathy (CR) is a disease of the cervical spine and a space-occupying lesion that occurs because of pathological problems with cervical nerve roots. Nerve root injury to produce functional disability.
OBJECTIVE:
The purpose of this study was to examine the effects of neural mobilization with manual cervical traction (NMCT) compared with manual cervical traction (MCT) on pain, functional disability, muscle endurance, and range of motion (ROM) in individuals with CR patients.
METHODS:
A blinded randomized clinical trial was conducted. Thirty CR patients were divided into two groups – those who received NMCT and those who received MCT. The intervention was applied three times per week for eight weeks. It was measured in order to determine the pain and functional disability in patients with CR. The numeric pain rating scale (NPRS), neck disability index (NDI), ROM, and deep flexor endurance of patients were measured prior to the experiment, four weeks, and eight weeks after the experiment to compare the time points. A repeated-measures analysis of variance was used to compare differences within each group prior to the experiment. And Bonferroni test was performed to examine the significance of each time point.
RESULTS:
There were significant differences within each group prior to the intervention, four weeks after the intervention, and eight weeks after the intervention in NPRS, NDI, ROM, and deep flexor endurance (
CONCLUSIONS:
These results suggest that the NMCT can pain relief, recovery from neck disability, ROM, and deep flexor endurance for patients with CR.
Introduction
Cervical radiculopathy (CR) is a disease of the cervical spine and a space-occupying lesion that occurs because of pathological problems with cervical nerve roots. Annually, 83.2 people out of 100,000 are diagnosed with this disease [1, 2, 3]. The most common causes of CR include trauma, spondylosis, disk herniation, spinal instability, and osteophytosis, but rarely from oncogenous-related diseases. CR results compression and inflammation of nerve roots, while structurally and functionally causing neural inflammation, edema, hypoxia, ischemia, and fibrosis, and decreases neural mobility [4, 5, 6, 7].
Conservative treatment for neck problems typically includes therapeutic exercise (range of motion (ROM), strengthening), manual therapy (muscle energy techniques, non-thrust mobilization, manipulation), modalities (transcutaneous electrical nerve stimulation (TENS), laser, cryotherapy, traction), massage therapy, medication, and cervical collar [1, 3, 8]. Manual cervical traction (MCT) is one of the manual therapy methods applied to CR patients. Manual traction increases vertebral body distance and foraminal space, which reduces pressure on nerve roots, thus enhancing blood circulation, and relaxes surrounding muscles, while recovering mobility of the spine and alleviating pain [9, 10, 11, 12, 13, 14]. Also, vertical plane axial traction can help decrease disk and fiber stress [15].
Neural mobilization (NM) improves neural flexibility, lowering dynamic sensitivity of the nervous system, and increases blood flow, relieving pain; improved neural mobility and alleviated pain increases joint range of motion (ROM), heightening dynamic adaptability and helping body movement without resistance [7, 16, 17]. Improved neural mobility and alleviated pain increases ROM, heightens dynamic adaptability and helps body move without resistance [18, 19]. According to the previous research, it appeared pain reducing effects and improving range of dysfunction and joint motion with applying nerve mobilization to the patients who suffer from back pain and radiating pain. It is caused by stimulating nociceptor sensitivity, increasing blood flow and recovering movement of neuron effect [20, 21]. Also, patient who have CR have effect on reducing pain and increasing disability when applying neural mobilization [19]. However, opinions about NM, as applied to CR are conflicting, and in particular, there is little research on the application of NM to spinal neuropathy patients. Moreover, research on simultaneous application of manual cervical traction (MCT) and NM to CR patients is minimal.
The purpose of this study was to examine the effects of NM with manual cervical traction (NMCT) compared with MCT on pain, functional disability, muscle endurance, and ROM in individuals with CR patients.
Methods
Subjects
The calculation of the sample size was carried out with
Numeric Pain Rating Scale (NPRS)
A pain marked with numbers from zero to 10 was used to measure the NPRS [22]. The tester explained to the patients that “Zero is a condition when you have no pain at all. Ten means a condition when you have unbearable pain. Please mark your degree of pain condition with the pen” and had the patients score themselves. This pain scale can be easily understood because the degree of pain is identified with numbers and has high repeatability. Test-retest reliability is 0.76 [23].
The Korean Version of the Neck Disability Index (K-NDI)
For the functional assessment of neck pain, the Korean version of the NDI developed by Vernon and Mior [24] and translated by Song et al. [25] was used to measure cervical pain and functional disability. The NDI was created using a questionnaire with 10 questions based on the Oswestry Index, which evaluates restrictions to ordinary life in relation to lumbar pain. The subjects selected a score of one to six (0 to 5) in 10 items: reading, headache, concentration, work, driving, sleeping, leisure life, pain intensity, ordinary life, and raising an object. The higher the sum of each item’s score, the more severe the functional disability related to cervical abnormality. Zero to four points, five to 14 points, 15 to 24 points, 25 to 34 points, and 35 points or higher signify no disability, weak disability, moderate disability, severe disability, and complete disability, respectively. Its inter-item consistency is 0.82, and its inter-rater reliability is 0.93 [25].
Flow chart of the subjects.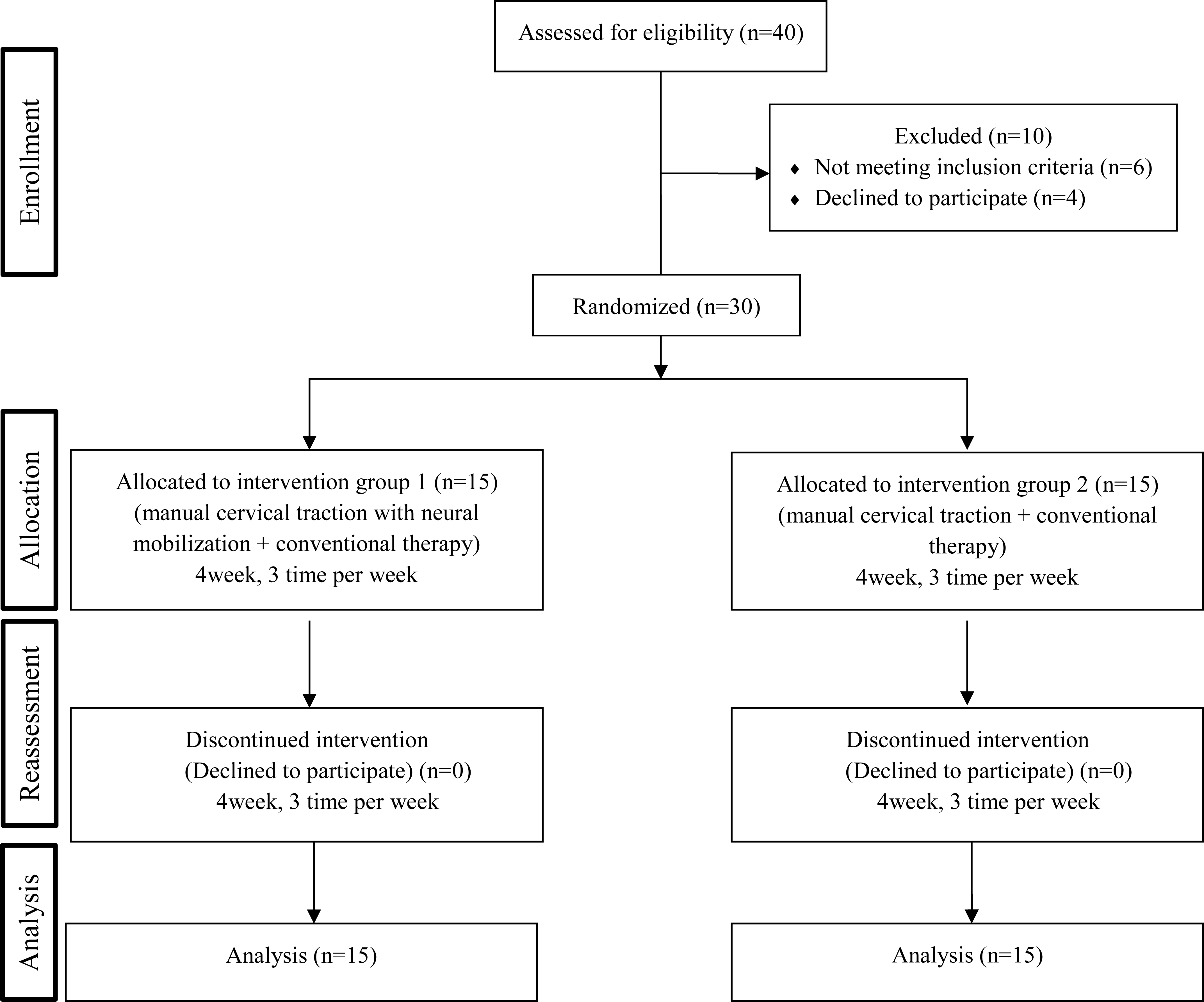
A cervical ROM instrument (Performance Attainment Associates, USA) was used to measure cervical ROM during cervical flexion and extension and cervical left and right side bending (SB), and cervical left and right side rotations. The subjects sat comfortably in a chair and looked straight ahead while the measurements were being taken. The goniometer was placed on the head of the subjects’ heads, and angles were measured using the device installed on the sagittal plane, coronal plane, and transverse plane. This tool’s inter-rater reliability is 0.66
Deep Flexor Endurance (by Cranio-Cervical Flexion Test (CCFT))
The CCFT aimed to selectively test deep flexor muscles of the neck. In this case, it was used to test the muscle endurance of the muscle groups. The amount of time that the patient was able to maintain a maximum of 60 percent voluntary contractile strength in the deep flexors was measured, and a biofeedback device (Stabilizer Pressure Biofeedback, Chattanooga Group Inc., USA) was used to measure maximum voluntary contractile strength of the cervical flexors. All of the measurements were taken three times and the average values were used for this study. The subjects rested for two minutes between each motion, and mmHg was utilized as the measurement unit. After resting for 2 minutes, each subject applied pressure with 60% of the maximum contractile force until the pressure gauge showed a difference of
In a supine position, the subjects maintained hip and knee joint flexion in their bilateral legs to prevent lumbar lordosis. The pressure biofeedback device was placed between the upper posterior cervical spine and the treatment table. The patient is instructed to move the head vertically (as if saying ‘yes’). The examiner provided a visual feedback with the pressure gauge while the subjects comfortably relaxed their heads without any movement. The measurements were taken on the treatment table with a hard base to measure any changes in the pressure gauge [27].
Experimental procedure
Prior to the treatment, the subjects’ general characteristics, NPRS, NDI, ROM, and deep flexor endurance (measured by CCFT) were examined. For eight weeks, they received NMCT and MCT treatment with conservative physical treatment three times per week. They received conservative treatment for 35 minutes and MCT treatment for 10 minutes each time. The experimental group received MCT accompanied by NM and the control group received MCT. The results were recorded on their clinical chart. After the four-week treatment, their NPRS, NDI, ROM, and deep flexor endurance were measured. Their NPRS, NDI, ROM, and deep flexor endurance were measured again using the same methods eight weeks after the treatment was applied (Fig. 1).
Conservative physical therapy
A hot pack for 20 minutes and TENS (Chungwoo Medical, CWM-601) was administered at a frequency of 60 Hz for 15 min. Two surface electrodes, 8.5
MCT
For MCT (Fig. 2), a manual therapist stood at the head of the treatment table facing the patient and covered the backside of the patient’s head with both hands hands (A). The therapist the bent his or her trunk back to apply traction power to the cervical spine for one minute (B) (Kaltenborn Grade 2). Grade 2 traction (tighten or “take up the slack”) that effectively separates the articulating surfaces and takes up the slack or eliminates play in the joint capsule [10].
Manual cervical traction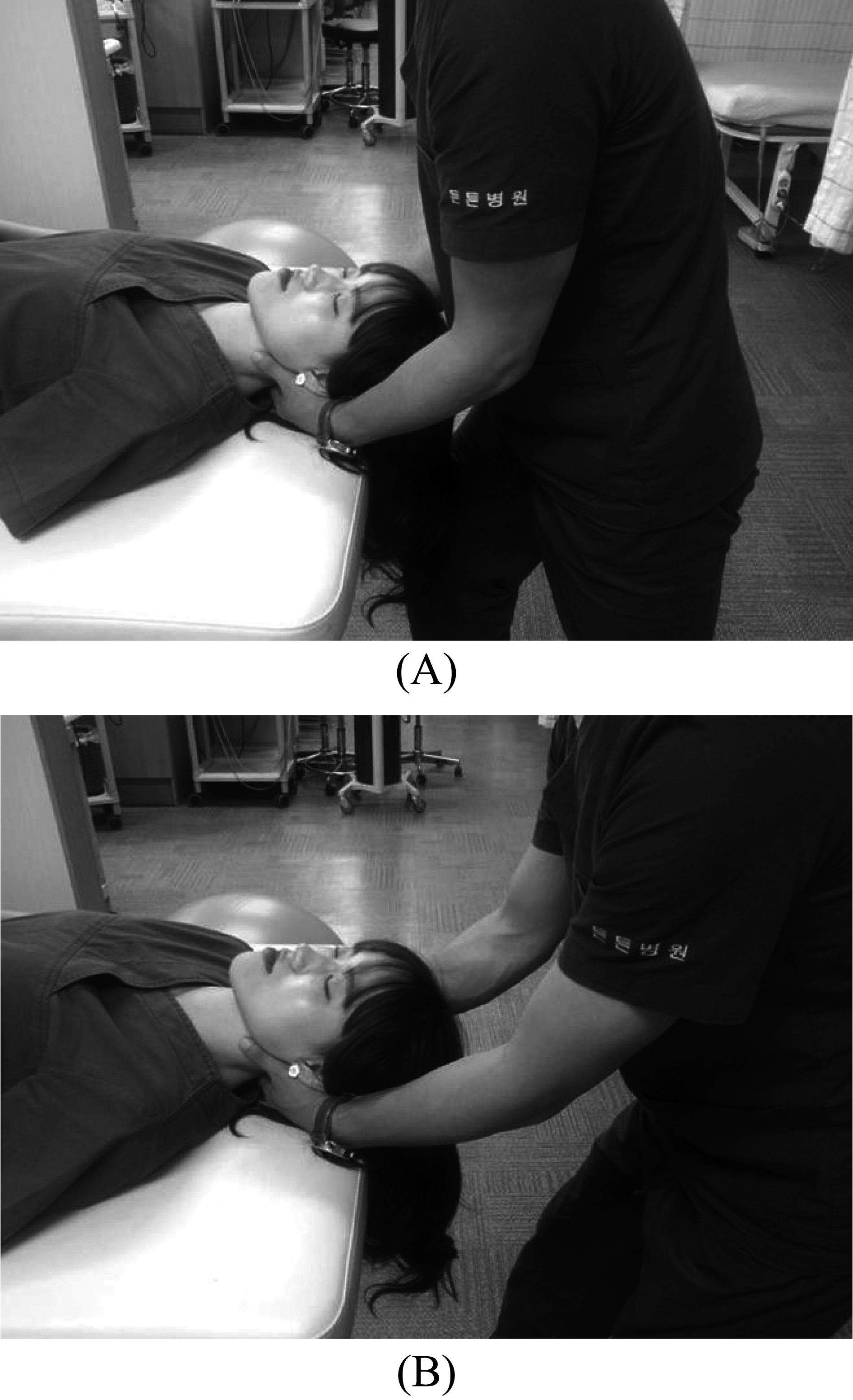
Neural mobilization with manual cervical traction.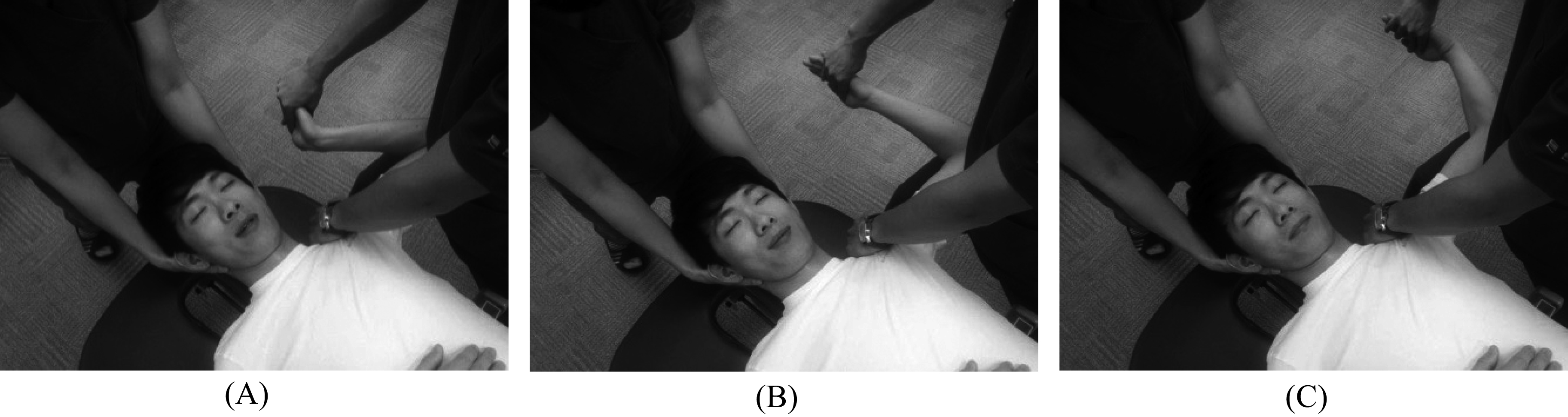
After one minute of traction power, the patient rested for 30 seconds. MCT was repeated six times for a total of 10 minutes.
Two manual therapists with more than five years of experience in the treatment and evaluation of the musculoskeletal system participated. This study was performed by the same therapist. For manual therapy, one manual therapist applied MCT (Kaltenborn Grade 2) for one minute while the other manual therapist applied neural mobilization using a slider technique in a smooth and rhythmic manner.
This study applied NM and MCT for ten minutes. And upper limb tension test 1 was applied as a preparatory posture. In this study, the slider technique consisted of the alternation of elbow extension (loads the median nerve) and wrist flexion (unloads the median nerve), with elbow flexion (unloading) and wrist extension (loading). NM and MCT of the median nerve were given at the same time. MCT was maintained for one minute while the elbow along with the wrist and fingers were moved in several positions to mobilize the median nerve. Figure 3: (A) In starting position, MCT was applied while the patient’s wrist was placed in a neutral position with the elbow flexion at 90 degrees. (B) During the application of MCT, the patient’s wrist and fingers were placed in full extension with full elbow flexion. (C) Maintaining the application of MCT, the patient’s wrist and fingers were placed in full flexion while the elbow was moved from full flexion to full extension [28]. After application for one minute, the subjects took a rest for 30 seconds. The same motions were repeated six times for a total of 10 minutes [29].
Statistical analysis
For comparisons in demographic and clinical baseline characteristics between groups, independent t or Chi-square tests were used for continuous and categorical variables, respectively. The Shapiro-Wilk tests (
Results
General characteristics of the subjects
General characteristics and homogeneity test results are presented in Table 1.
There were no significant differences at baseline between the two groups in terms of age, height, weight, NPRS, NDI, ROM, and deep flexor endurance (CCFT result).
Comparison of pain
Over time, pain significantly decreased in the NMCT group (pre: 7.00
Regarding changes in pain, the NMCT group’s pain decreased significantly more than the MCT group (NMCT change:
Comparison of NDI
There was a significant decrease in NDI over time for both the NMCT group (pre: 21.67
Comparison of ROM
ROM results are presented in Table 2.
The changes in flexion and extension were significantly greater in the NMCT group than in the MCT group (NMCT flexion change: 15.53
The NMCT’s changes in bending of the left and right sides were significantly greater in the NMCT group than in the MCT group (NMCT left side change: 10.33
The NMCT’s changes in rotation of the left and right sides were significantly greater in the NMCT group than in the MCT group (NMCT left side change: 10.13
Comparison of deep flexor endurance
General Characteristics of the Subjects at baseline. (
30)
General Characteristics of the Subjects at baseline. (
Data expressed as mean (SD). NMCT, Neural mobilization with manual cervical traction; MCT, Manual cervical traction; NPRS, Numeric pain rating scale; NDI, Neck disability index; ROM, Range of motion; Flex, Flexion; Exten, Extension; Rt, Right; Lt, Left; SB, Side-bending; Rot, Rotation; CCFT, Cranio-cervical flexion test.
Comparison of the range of motion
Data expressed as mean (SD). NMCT, Neural mobilization with manual cervical traction; MCT, Manual cervical traction; Flex, Flexion; Exten, Extension; Rt, Right; Lt, Left; SB, Side-bending; Rot, Rotation.
Over time, deep flexor endurance measured by CCFT significantly increased both in the NMCT group (pre: 8.18
Comparison of numeral pain rating scale and neck disability index.
Comparison of deep flexor endurance.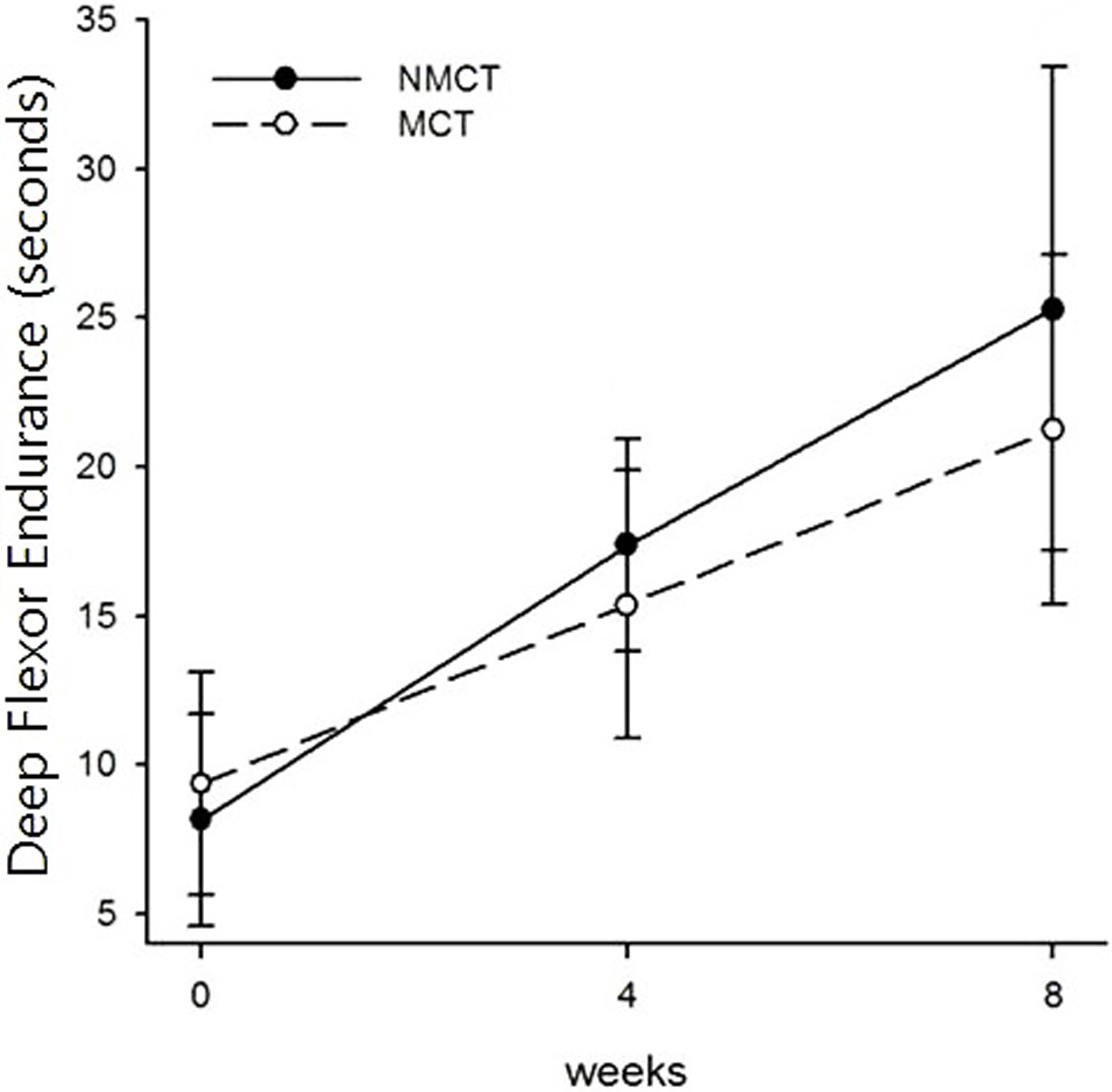
The result of the present study is that significant decrease in pain and NDI, and a significant increase in ROM and deep flexor endurance were observed following NMCT for eight weeks, when compared to MCT.
Lamba et al. [19] applied mechanical traction and NM to patients with C6–C7 radiculopathy and reported a decrease in pain from 6.6 prior to the treatment to 0.8 after the treatment. Savva and Giakas [29] simultaneously applied MCT and NM to patients with cervico-brachial pain 12 times and observed that pain in the cervical and brachial region decreased from eight points to one point and from seven points to zero points, respectively. They noted that such a decrease in pain reduced pressure on the cervical nerve roots, recovered movement of the neurological system, prevented elements that can aggravate pain resulting from CR, and alleviate pain by stimulating mechanical receptors. In the present study, total average changes from 7 point to 2.5 point after getting treatment. It can check the changes from severe pain to mild pain. The slider technique used in this study triggers movement of the nerves and does not cause tension in or pressure on the neurological system. This technique moves one joint on one side of the nerve track, thereby providing tension, and then moves another joint on the other side of the body to relieve tension, thereby inducing neural gliding and reducing the slope of tension [7, 28]. The result of the present study was similar to that of the previous studies.
Cervical traction increased intervertebral spaces, decreased pressure on the disks, and extended the muscles and ligaments of the spine [12]. Gupta [20] and Sarkari and Multani [21] applied NM to patients with lumbar and radiation pain and noted that recovery of nerve movement through stimulating the sensitivity of the nociceptors and increasing blood flow resulted in decreased pain and improvement in disability index. Cleland et al. [30] observed that a combined intervention of cervical traction and muscle-strengthening exercise applied to CR patients enhanced their NDI. Savva and Giakas [29] reported that simultaneous application of MCT and NM improved NDI. The above studies involved combining another treatment method together with cervical traction and showed a similar result to that of the present study in which MCT, accompanied by NM, significantly decreased the disability index. Our study’ total average change from 22 to 12 after getting treatment. As a results, by stimulating nociceptor sensitivity, increasing blood flow and recovering movement of neuron effect.
The methods used to measure physical ability in patients with cervical pain are muscle strength and ROM measurements [31]. Measuring the range of movements when neck and shoulder movements are disabled is a crucial element in determining the degree of disability and treatment [32]. Ylinen et al. [33] reported that cervical pain decreased cervical movements and muscle strength, and cervical pain patients had reduced mobility of the cervical spine, compared to healthy people [34, 35].
Marks et al. [36] reported that NM applied to cervico-brachial pain patients enhanced their lateral flexion and rotation. This result indicates that NM stimulates mechanical receptors, thereby increasing neural gliding and enlarging nerve-track distance and improving neural movements [16, 17, 21]. It also relaxes the nerves where they collide with each other, thus breaking nerve adhesion and moving the nerve roots without pain [37]. NM is regarded as having an impact on retraining the joints and muscles that are adjacent to the nerves. This present study’ results showed that increased of ROM.
Compared to healthy persons, patients with cervical pain have reduced ability to control the cervical region because of the weakening of deep muscles, such as the longus colli muscle and the longus capitis muscle. These patients experience a restriction in activity, which decreases the amount of physical activity thereby reduction the ability to adjust deep muscle strength [27, 38]. In the present study, deep flexor endurance increased more in the NMCT group than in the MCT group. The results of the present study support the use of NMCT as a possible therapeutic strategy for patients with CR.
Limitations
The limitations of this study are as follows: First, it is critical point not to use ultrasound to see nerve excursion, and we can’t generalize because we don’t another RCT study result. Second, the age range of the patients was narrow and the number of participants was small. Third, whether the treatment method can be applied to acute patients and bilateral patients was not verified, and objective measurement of the weakened upper-limb muscle strength, dysesthesia, and radiation pain could not be collected. Continuous future research, which complements these limitations, is necessary.
Conclusion
This study applied NMCT to CR patients and examined the effects of the therapy on the patients’ pain, NDI, ROM, and deep flexor endurance. This study demonstrates the superiority of the NMCT, with some advantages in the pain, NDI, ROM, and deep flexor endurance, compared with MCT in combination with physical therapy agents for the management of CR patients. Future research should verify the effects of NMCT with a larger number of subjects.
Conflict of interest
The authors have no conflict of interest to report.