
Abstract
BACKGROUND:
Mechanomyography (MMG) has been used to investigate mechanical characteristics of muscle contraction in clinical and experimental settings.
OBJECTIVE:
The aim of this study was to determine the test-retest reliability of mechanomyographic amplitude (MMG
METHODS:
There were ten young adults participating in this study. Accelerometers were used to detect surface MMG signals from three trials of 5-s MVICs of the rectus abdominis, external obliques, erector spinae, and multifidus in the vertical, transverse, and longitudinal directions. Intraclass correlation coefficient (ICC), standard error of measurement (SEM), and minimum detectable change were calculated.
RESULTS:
Good to excellent test-retest reliability of mechanomyographic amplitude (MMG
CONCLUSIONS:
This study demonstrates that MMG is a reliable measurement to detect the activation amplitudes of trunk muscles during MVIC.
Introduction
Mechanomyography or the mechanomyogram (MMG) is a method used to record dimensional changes in active skeletal muscle fibre contractions at low frequency oscillations [1, 2]. Analysis of MMG signals allows examination of various aspects of muscle function, such as neuromuscular fatigue [3] and neuromuscular disorders in adult and paediatric populations [4], the control of external prostheses, and measuring the effectiveness of anaesthesia [5]. Currently the standard tool for measuring muscle contraction is electromyography (EMG). When recorded simultaneously with EMG from the same muscle, MMG exhibits a similar pattern [6]. While EMG amplitudes measure the motor unit action potentials during muscle contraction, MMG detects the mechanical oscillations of contracting muscle fibres [7].
MMG is a mechanical signal that can be recorded from the surface of a contracting muscle when the movements of muscle fibers cause vibrations as the source of the wave generation [8]. A number of sensors can be used to record MMG, including accelerometers, microphones, piezoelectric sensors, and laser sensors [9]. In general, the wave propagation has been reported as muscle oscillations in the lateral [10, 11, 12, 13], longitudinal [14] and transverse [14, 15] directions. Additionally the transverse direction of MMG signal propagation could be produced when the oscillation frequency less than 25 Hz, otherwise it would be shown in the longitudinal direction [16]. Thus a triaxial accelerometer has been used for MMG recordings of muscle oscillation amplitude [17].
Reliability refers to the reproducibility of measurements when repeated at random in the same subject, representing one of the principal characteristics of an outcome measure in clinical trials. Measurement reliability is important to consider when choosing the primary outcome measure for clinical trials and should be assessed and assured through a quality control program based on randomly selected duplicate assessments [18]. Reliability is a method to measure the consistency or repeatability of measurements that includes relative reliability and absolute reliability. Relative reliability represents the relative consistency of measurements that can be explained using an intraclass correlation coefficient (ICC) [19]. Moreover, absolute reliability is the degree of the repeated measurements that uses standard error of measurement (SEM) and Bland and Altman’s 95% limits of agreement to represent outcomes. SEM also represents the absolute measurement error expressed as a percentage of the grand mean (SEM%) with an acceptance level of
The reliability of MMG has been tested on limb muscles. Akataki et al. [22] confirmed the reliability (average ICC
Methods
Participants
Ten healthy volunteers (5 men and 5 women, 23.5
Instruments
The MMG signal was collected using a set of triaxial accelerometers (LIS331DLH; STMicroelectronics, Inc., Geneva, Switzerland, 3
Experimental protocol
For MVIC measurements of trunk muscles, each participant lay on the bed with legs held immobile with a belt in the supine position for abdominal muscles and in the prone position for back muscles. The investigator applied resistance on the shoulders for 5 s during MVICs. The participants performed three trials, one for familiarization and two experimental trials. The order of testing for each muscle was randomized. A 5-min rest was allowed between each muscle trial, whether practice or test trial, and a 1 h rest was allowed between test and retest to avoid fatigue.
The postures held for evoking MVIC of related trunk muscles included the following: (1) RA by a resisted curl-up with resistance applied in a symmetrical manner on the shoulders of the participant by the investigator; (2) right EO by a resisted crossed curl-up with the right shoulder towards the left and resistance applied on the right shoulder by the investigator; left EO was in an opposite direction; and (4) MF and ES, let the participant be in prone position with hands on the neck to lift the head, shoulders and elbows just off the examination table in the meanwhile symmetrical manual resistance was provided to the scapular region by the investigator.
Signal processing
MMG signals (ms
ICC, SEM, %SEM, MDC, %MDC for MMG
measures of trunk muscles during MVIC
ICC, SEM, %SEM, MDC, %MDC for MMG
Note. MMG, mechanomyography; EO, external obliques; RA, rectus abdominis; ES, erector spinae; MF, multifidus; ICC, intraclass correlation coefficient; SEM, standard error of measurement; %SEM, standard error of measurement as a percentage of the grand mean; MDC, minimal detectable difference; %MDC, minimal detectable difference as a percentage of the grand mean. A paired t-test was performed to determine the differences in MMG
The raw data of MMG and RMS data during MVIC from one participant.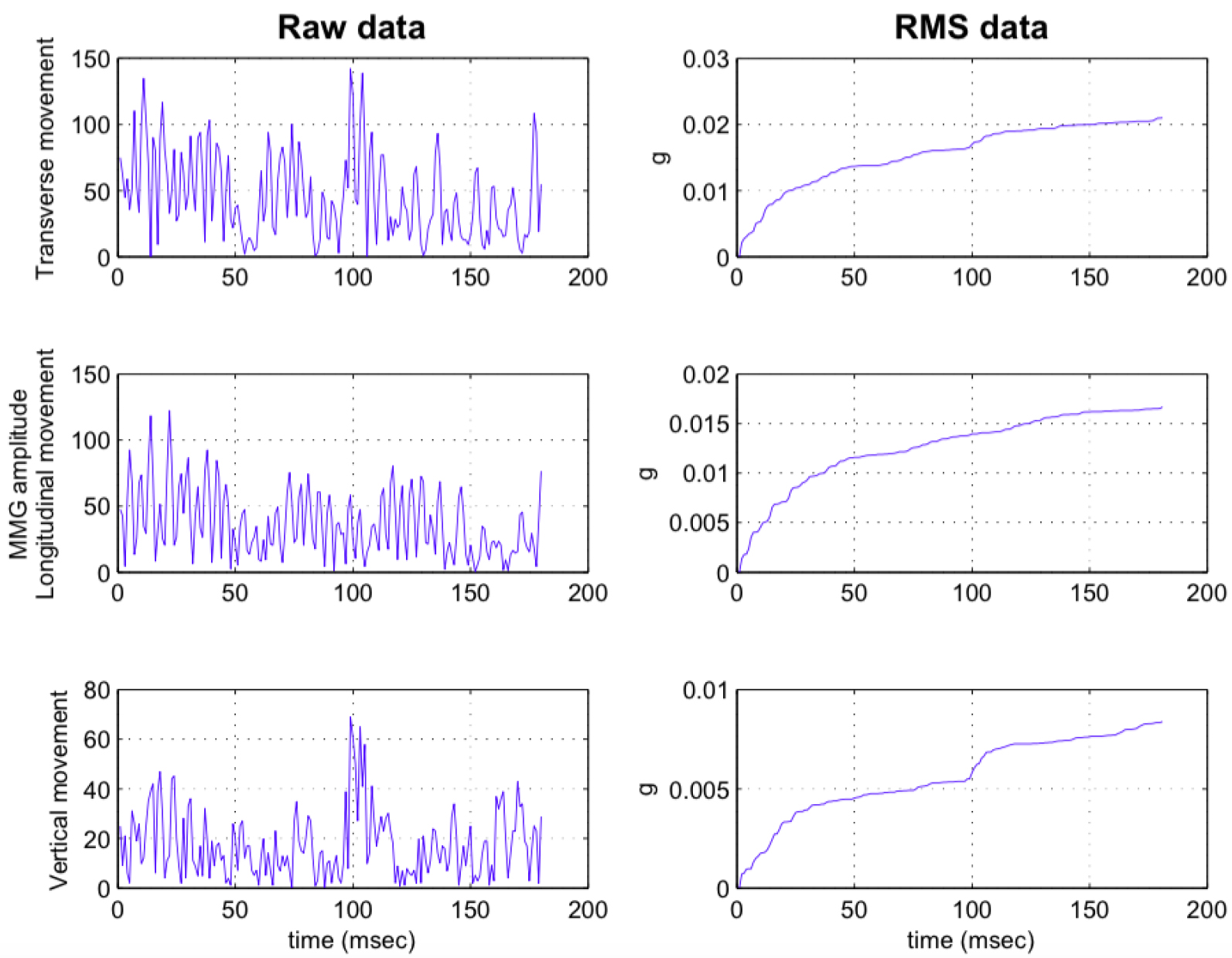
Absolute reliability of the MMG
Note. MMG, mechanomyography;
The comparison of trunk muscle MMG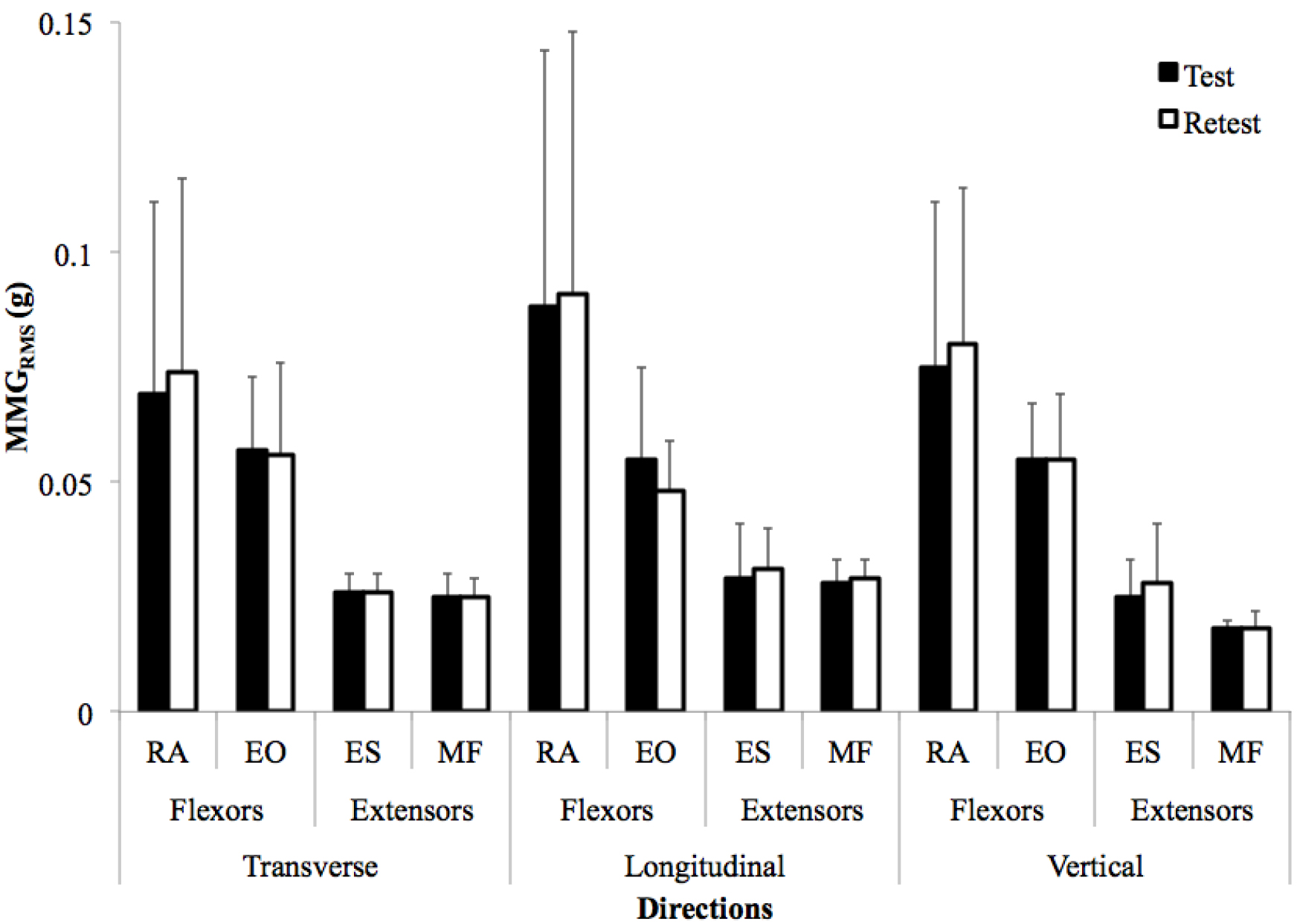
Descriptive statistics included mean and standard deviation for age, body height, body weight, and MMG
where
Results
The original data of MMG and MVIC from one participant was demonstrated as Fig. 1. The reliability and measurement variability statistics for MMG
Discussion
In this study, we assessed the test-retest reliability of MMG for MVIC of trunk muscles. To measure the level of agreement between test-retest measures, indices such as ICC were used. ICCs found in this study indicate good to excellent relative reliability of MMG signals of trunk muscles during MVIC. Relative reliability is the degree to which individuals maintain their position in a sample with repeated measurements, which are affected by between-subject variability. Compared with studies of limb movements, which have reported poor to good reliability for ICCs within the 0.36–0.93 range [21], this study clearly showed that MMG for trunk muscle activation during MVIC is a detectable and reliable measurement.
Using ICCs alone does not reflect the comprehensive features of reliability. The Bland and Altman method for absolute reliability provides an alternative approach and supplements the ICC measurements for assessing reliability in clinical research. Absolute reliability is the degree to which repeated measurements vary for individuals [20]. Apart from the Bland and Altman method, SEM and MDC can also be used to quantify measurement errors caused by repeated measurements. The Bland-Altman plot provides a visual interpretation to inspect the size and range differences in measurements and any bias or outliers. The 95% CI for the mean difference indicates systematic bias in measurements [18]. Furthermore, we also found good to excellent reliability with good agreement in measurements from the Bland-Altman plots. We have demonstrated that MMG is a reliable measurement to detect oscillations of trunk muscles during MVIC with an acceptable SEM, except for the RA muscle.
There are several limitations in the study. First of all, a limited study population of healthy young adults was recruited in this study; therefore, the test-retest reliability of MMG measurements for trunk muscles in this study cannot be generalized for the entire population. In addition, we did not determine the torque produced by the torque transducer synchronized with MMG during MVIC quantitatively because of the limitation of measurement setup for MVIC of trunk muscles. And the manual resistance from the operator during MVIC could introduce artefacts due to movement such as limb tremors, which are difficult to identify and remove from MMG signals as a source of variability [30].
In addition, MMG
These findings indicate that MMG amplitude measurements show good test-retest reliability for MVIC of trunk muscles with good to excellent ICCs and acceptable SEM% and MDC. MMG appears to be a reliable tool for investigating trunk muscle responses during isometric contraction. The MMG in this study is a reliable measurement for detecting the activation amplitudes of trunk muscles during MVIC; for clinical relevance, we suggest using a lightweight mechanomyographic sensor as a wearable sensor for measuring not only mechanical characteristics of muscle contraction levels during dynamic activities, but also for rehabilitation as a biofeedback tool to monitor muscle activities of the trunk muscles Furthermore, future work applying MMG ought to further investigate the mechanical characteristics of trunk muscles and establish the reliability of MMG measurements of trunk muscles in individuals with low back pain.
Conflict of interest
None to report.
Footnotes
Acknowledgments
The authors acknowledge the grant (BMRP349, CMRPD1B0221, EMRPD1G0241, 98-2410-H-182- 022-MY2, 99-2410-H-182-039) from Chang Gung Memorial Hospital and Healthy Aging Research Center of Chang Gung University in Taiwan, and thank all participants in this study.