
Abstract
BACKGROUND:
Sciatica-related Foot Drop is a peripheral nervous condition that produces a loss of power in the ankle dorsiflexion muscles. Functional electrical stimulation is a modality of electrical stimulation that produces muscle contraction in a functional movement of the limb. This technique was utilized with positive effects in central nervous afflictions but it is not known whether or not it has any influence in motor recovery following peripheral nervous system problems. This study aims to clarify the effects of functional electrical stimulation on foot drop caused by peripheral nerve compression resulting from lumbar disc herniation.
METHODS:
Fifty patients were enrolled in our study; of whom 25 were treated with EMG triggered electrical stimulation (EMG-FES) and 25 with heel-floor sensor triggered electrical stimulation (SWITCH-FES) during normal gait cycle. Patients received functional electrical stimulation (with a pulse of 60 Hz and phase duration of 200 ms) once a day, for 30 minutes during 5 consecutive days, over a period of 4 weeks. Electrical diagnostic tests (nerve conduction velocity/NCV and the amplitude of compound muscle action potential/CMAP), dynamometry and Osvestry Disability Index scores were measured at baseline and after treatment.
RESULTS:
We found that axonal loss was lower in the EMG-FES group than in the SWITCH-FES group (
CONCLUSIONS:
The overall results showed that there was a significant increase in all the parameters studied for both types of FES applications. However we found that the EMG triggered electrical stimulation technique had a higher influence on the quality of the muscle action control. For patients who cannot yet produce minimal muscle active contraction we recommend switch triggered stimulation first and then, immediately after the recovery of the motor control, to change to EMG triggered functional electrical stimulation.
Introduction
Foot drop refers to a significant weakness of ankle and toe dorsiflexion that can be caused by a number of clinical disorders. In the specialized literature foot drop was defined as a significant decrease of tibialis anterior and extensor halluces longus muscles force [1]. Using manual muscle testing (MMT), foot drop was categorized as the ankle dorsiflexion power at MMT grade 3 or less [2, 3, 4]. It can be present in paretic/paralytic lower limb determined by peripheral pathologies such as degenerative conditions of the spine as well as central nervous system pathology.
This relatively simple movement of foot elevation is of major importance in ambulation. In the swing phase of the gait cycle the inability of the patient to elevate the forefoot may cause multiple falls and injuries, reducing mobility and the quality of life. Furthermore, the pathologically modified gait cycle can lead to significant changes in the biomechanics of the lower limb and spinal level, inducing forces that could create inappropriate musculoskeletal structural changes. Properly management of this impairment during physiotherapy is, therefore, important and consequential.
The most common degenerative conditions that can cause foot drop are lumbar disc herniation and spinal canal stenosis. In two case series it has been observed that 57% of the patients suffering from foot drop had lumbar disk herniation [5, 6]. In another study that included 46 cases of foot drop related to lumbar disease, 52% of the cases were due to disc herniation [4]. In the majority of cases, the ankle dorsiflexion paresis appears when the sciatic nerve is compressed at the L4-L5 level (L5 root) between 32%–73% [6, 7], followed closely by L5-S1, then L3-4. Due to the fact that foot drop is seen as a serious problem underlying spinal pathology, almost all cases are recommended for surgical treatment. Although the surgical treatment has been noted to have a positive effect on foot drop recovery, there is a general nonresponse rate between 21% and 49% [2, 4, 7, 8].
Functional electric stimulation (FES) is a form of electrical stimulation applied in physiotherapy practices on a nerve pathway or motor point to produce muscle contraction that can be assimilated in the normal motor engram. The patient uses stimulation to execute a functional movement and, depending on the severity of the paresis, it can be used as a functional substitute [9]. In the case of foot drop, the stimulation is made on the common peroneal nerve. The forefoot is raised by electrical stimulation during the dynamic swing phase of the leg, and the patient’s gait is thus improved [10, 11].
The literature abounds in clinical studies regarding utilization of FES for patients with upper neuron problems such as multiple sclerosis, Parkinson and stroke but is utterly silent in what concerns the investigation of the effects of FES on peripheral neuronal regeneration and its muscle functional reintegration [12, 13, 14, 15, 16, 17, 18].
The present study wants to clarify if FES is potentially efficient in the functional re-education in foot drop and muscle re-innervation due to peripheral nerve injuries, and to compare two different techniques of employing FES.
Materials and methods
Participant recruitment and inclusion criteria
Fifty patients suffering from foot drop after surgical decompression of the sciatic nerve were enrolled in our study. We have only taken into consideration patients with motor deficit after surgical treatment because we wanted to exclude the neural compression factor and to see whether the FES treatment alone can be utilized as a last resort in the functional rehabilitation of the paralytic forefoot. After clinical examination, all patients were included in the study. We explained what the requirements were and all the patients gave their signed informed consent before the beginning of the trial. The study took place at the Physiotherapy and Medical Rehabilitation Center from the University of Medicine and Pharmacy “Grigore T. Popa” Iasi and it was carried out in accordance with the Helsinki Declaration.
The patients were selected after applying the following inclusion criteria: radicular nerve pinching caused by herniated lumbar disc; the presence of paretic sciatica after discectomy; foot drop syndrome; muscular manual force test (MMT)
Electrical stimulation
FES was applied in both subgroups in 20 physiotherapy sessions as follows: once a day for 30 minutes during 5 consecutive days, over a period of 4 weeks. Stimulation was performed on the affected limb by using surface electrodes according to the principle of transcutaneous electrical nerve stimulation (TENS). The scientific literature provides information about the frequency and phase duration on static electrical stimulation for peripheral nerve regeneration and axonal repair (20 Hz) but it does not provide these parameters for use of FES in peripheral nerve problems [19, 20]. Taking into account that, with FES, we wanted to produce a continuous functional movement of the ankle dorsiflexion and the frequencies lower than 40 Hz produced a jerky movement that could not be properly integrated in the gait cycle, we used a pulse of 60 Hz and phase duration of 200 ms.
The device used to deliver the functional electrical stimulation for the EMG-FES group was the sEMG
sEMG triggered muscle stimulation is a protocol that requires a patient to voluntarily contract a muscle in order to initiate a certain movement. The patient is asked to generate a maximum contraction during the 10 second capture time; the software will then identify the maximum muscle effort automatically. The sEMG evaluation is done through the detection of peak to peak signal and is returned as a graphic numerical scale. If the measured sEMG level generated by the muscles was equal to the previous registered signal level, it triggers the system to deliver electrical stimulation to the same muscles thereby assisting them during functional movements (Fig. 1).
EMG triggered functional electric stimulation technique. 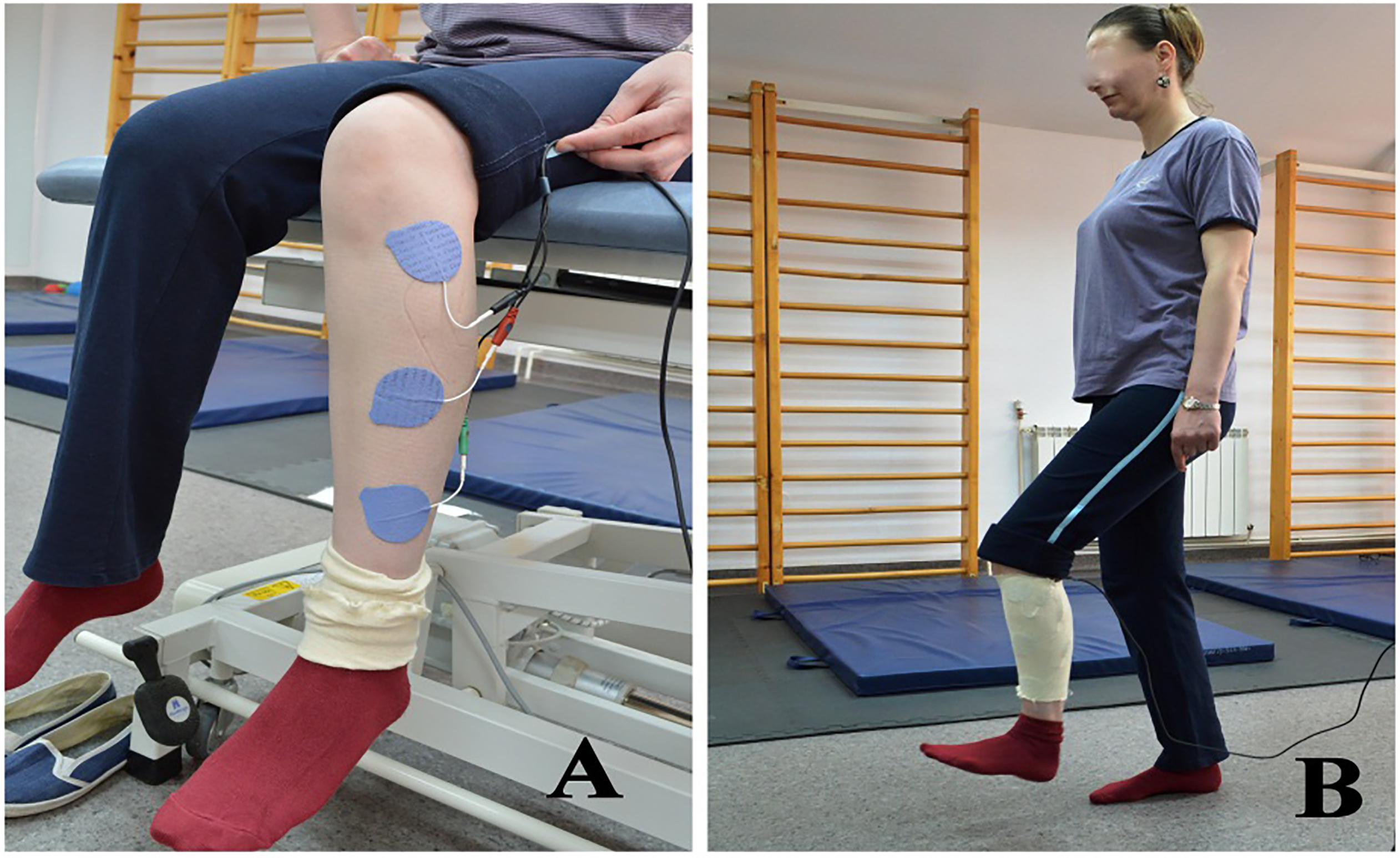
Switch triggered technique. 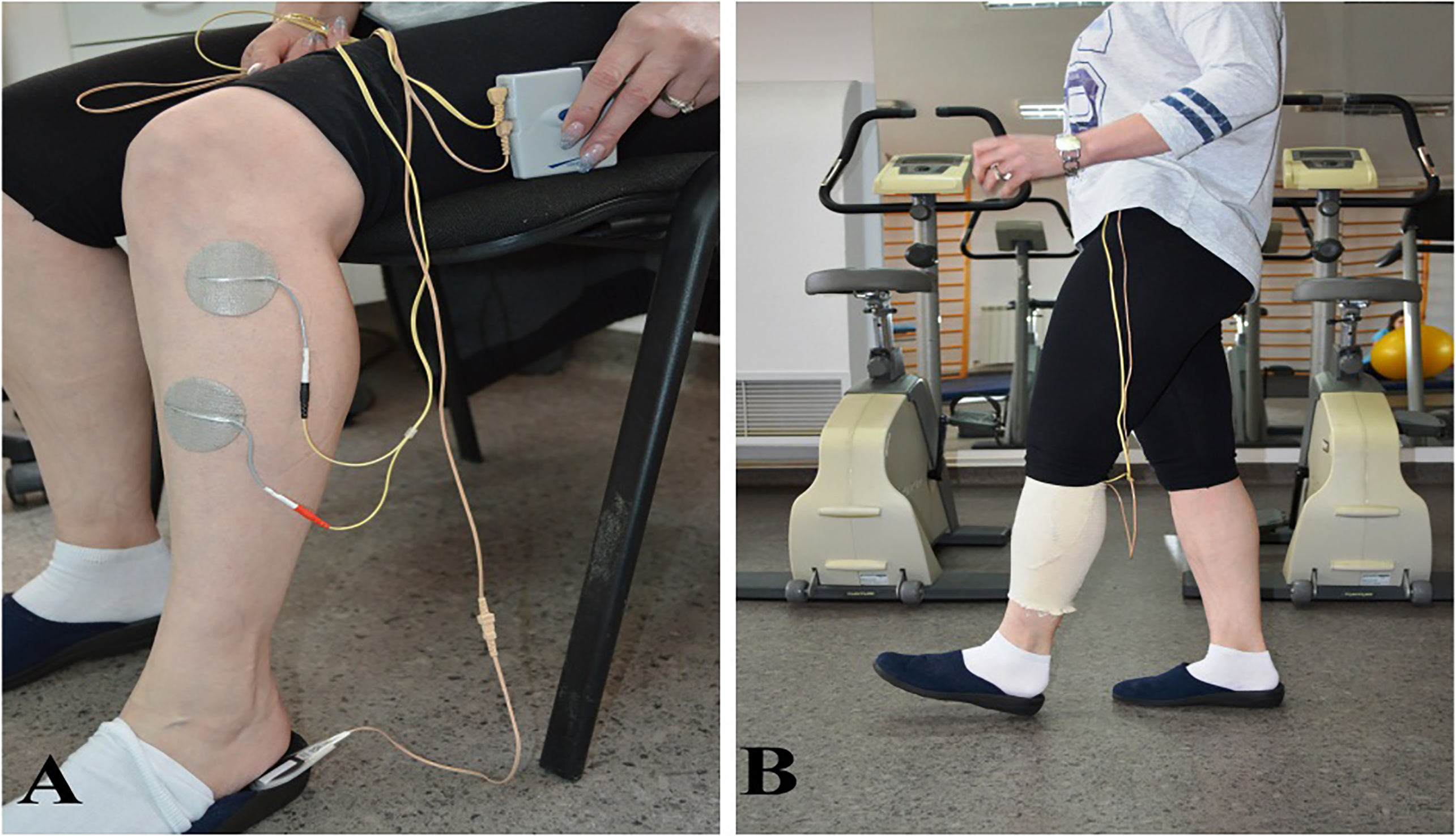
For the SWITCH-FES group electrical stimulation was done with ODFS – Pace 1.0 (Odstock Dropped Foot Stimulator) from Odstock medical Ltd. U.K. FES was administered percutaneously via round electrodes measuring 4 cm in diameter. The cathode electrode was placed immediately under the proximal head of the peroneus bone and the anode was placed on the anterior face of the tibialis anterior muscle. In the SWITCH-FES group the electrical contraction was determined by a foot-floor sensor mounted under the heel. When the heel is elevated during the gait cycle the electrical stimulation is transmitted (Fig. 2).
The demyelination and axonal loss were assessed by studying nerve conduction at the beginning and at the end of the treatment. For electrophysiological investigations the electromyograph Neuro – MEP Micro was used. The stimulodetection examination was realized in the motor fibers of peroneal nerve. We took into consideration the nerve conduction velocity (NCV-m/s) to evaluate the demyelination and the amplitude of compound muscle action potential (CMAP-mV) to evaluate the axonal loss [21]. The surface electrodes were used to obtain muscular response according to the principle “belly-tendon” (the active electrode was placed on the muscle belly and the reference electrode on its tendon). The ground was placed between distal stimulation and the recording electrodes. Proximal site of stimulation was placed behind the fibular head and distal site was ankle (between the extensor digitorum longus and extensor hallucis longus tendons. The extensor digitorum brevis muscle represented the collection point of the recording. For data acquisition, specific settings were used: sensitivity (500
Muscle force was tested also in order to correlate the functional restoration of the link between the nerve and muscle. The MMT as described by the Medical Research Council [22] is a manual force test performed by the physiotherapist and is too subjective to the physiotherapists experience and sensitivity to produce accurate data. To obtain more objective measurements we used the “make test” from the handheld dynamometry technique (HHD). The muscle force test was performed twice and we took into consideration the sum of the two muscle force values. We used a Baseline
The overall functional status was evaluated by the Oswestry Disability Index (ODI) because foot drop caused by radicular compression is closely related to lumbar column status. ODI is an index derived from the Oswestry Low Back Pain Questionnaire used by clinicians and researchers to quantify disability for low back pain and its related dysfunctions. The self-completed questionnaire contains ten topics concerning intensity of pain, lifting, ability to care for oneself, ability to walk, ability to sit, sexual function, ability to stand, social life, sleep quality, and ability to travel. Oswestry Disability Index is currently considered by many as the gold standard for measuring the degree of disability and estimating quality of life in a person with low back and leg pain [26].
Statistical analysis
The statistical analysis of the results was performed using the BioStatAnalystSoft software package. Because we have only a limited number of patients, we tested the normality of the distributions and we used the Shapiro-Wilk normality test. In our study all data was normally distributed except for gender. In the case of gender analysis, we opted for the nonparametric Chi-square test. The results were expressed as mean
Results
In our study the first group was made up of 25 patients (14 males and 11 females), with mean age of 44.40
We did not find any statistical differences in gender (Chi-square test,
The results for both groups of nerve conduction velocity were not statistically significant. However, in the analysis made on CMAP we found differences between the two groups. For the EMG-FES group CMAP registered initially 1.252
Data analysis before and after the treatment
Data analysis before and after the treatment
At the end of therapy, CMAP increased for the EMG-FES group with 0.642
The most important and different results between the patients treated with EMG-triggered electrical stimulation versus switch group were found in the scores of the tests that evaluated the functional status related to capacity of movement and capacity of carrying out normal life activities. The Dynamometry results were at the beginning 11.04
The ODI initial score (35.84
In this study, we presented two different techniques for functional electrical stimulation in peripheral nerve pathology, after having noticed the lack of published scientific evidence comparing Switch with EMG triggered FES, Also, we were interested in the uses and effects of functional electrical stimulation on peripheral nerve pathologies such as radicular nerve compression. The technique is widely used in cases of foot drop from central nervous system affliction and its effects are highly documented [9, 10, 11, 12, 13, 14, 15, 16, 17, 18].
Although the nervous system is an integrated one, the functional reeducation in a peripheral nervous system affliction differs consistently in its mechanisms from that of the central nervous system. In order to regain central motor control, the peripheral nerve must first regain its integrity and conductibility. The problem with the utilization of FES on a peripheral nerve injury is that there is insufficient valid data to provide useful insights regarding the appropriate stimulation settings.
In our study, we enrolled fifty patients suffering from foot drop secondary to lumbar spinal disc herniation. They received 20 intensive physiotherapy sessions of FES training by means of two different modalities of triggering the electrical stimuli. We wanted to identify if there is a difference on the peripheral nerve regeneration and muscle functional reintegration when using EMG as opposed to SWITCH triggering of the electrical stimuli. At the end of the treatment, the evaluation showed that the EMG-FES group had slightly better results than the SWITCH-FES group. The EMG-FES group showed improvements in CMAP (
The results registered for NCV test at the end of the treatment were similar with those from the beginning of the treatment due to the short period of nerve compression. These outcomes can be considered normal, as the nerve did not have time for demyelination [21]. However, in the EMG-FES group, we measured significant p values for CMAP, so the number of axonal loss was significantly lower than in the SWITCH-FES group.
Moreover, we noticed a significant difference in muscle control in favor of the EMG – triggered stimulation. This may be explained by the different modality of triggering the electrical stimulation. In the SWITCH-FES group, the stimulation was determined by means of a foot-floor sensor while raising the heel. This means that the stimuli activated the muscle without any participation from the patients, which makes this technique a passive one.
The EMG triggered electrical stimulation training group involved voluntary muscle contraction to trigger the FES. A prerequisite for this type of stimulation is the capacity of the paretic muscle to tens at a level that allows for an EMG signal to be measured by a surface electrode which makes this an active technique for the patient [9]. In contrast to the foot-floor switch technique, where the patient follows a pre-established electrical pattern of movement, in the EMG triggered stimulation technique the movement pattern is activated and determined actively by the patient. EMG triggered technique therapy implies more motor control and cognitive abilities from the part of the patient. EMG triggered stimulation may be more effective than the simple or switch triggered techniques in improving motor control [26, 27]. In our patients, lower limb electrical stimulation improved walking ability, increased mobility and increased voluntary EMG activity in EMG triggered FES. In the FES group we obtained increased isometric contractions of dorsiflexors and plantar flexors and improved walking ability.
In the EMG triggered group we noticed an important correlation between the subjective overall functional status felt by the subjects (ODI score) in relation to the increased motor control of the dorsal ankle flexion (Dynamometry).
Conclusions
In this study we evaluated the influence of functional electrical stimulation over sciatica-related foot drop syndrome. The overall results showed that there was a significant increase in all the parameters studied for both types of FES applications. However, we found that the EMG triggered electrical stimulation technique produced better results in the quality of muscle action.
The most physiologically appropriate neural pathway for the reinforcement of the dorsiflexors muscles would be to use homonymous EMG signals in order to provide immediate and direct autogenic feedback in dorsiflexion control.
Our recommendation for clinical practice is to start with the passively triggered technique if the patient does not have the possibility to tense the muscle and then, immediately after the recovery of motor control, to change to EMG triggered functional electrical stimulation.
Footnotes
Acknowledgments
This study was made possible with support from the University of “Grigore T. Popa” Medicine and Pharmacy Iasi, as part of the research grant No. 3110.
Conflict of interest
The authors declare no conflicts of interest.