
Abstract
BACKGROUND:
Manual physical therapists (MPTs) working in primary care get limited information about patient’s courses of (chronic) low back pain (LBP). Identification of kinesiophobia is mostly based on clinical perception.
OBJECTIVE:
The aim of this study was to evaluate the association between the scores with which manual physical therapists in a primary care setting identify kinesiophobia in patients with low back pain, and the patients’ self-reported measures of kinesiophobia.
METHODS:
The cross-sectional study comprised 104 patients with LBP and 17 MPTs. Patients first independently completed the Tampa Scale for Kinesiophobia (TSK-17). The therapists, blinded to the TSK-scores, rated their perception of a patient’s kinesiophobia using the Visual Analogue Scale-Estimation (VAS-est) and the accuracy of their ratings using the Visual Analogue Scale-Accuracy (VAS-ac). Kendall’s tau b was used to determine the level of correlation between scores on the TSK-17 and the VAS-est.
Introduction
Physical therapy (PT) requires a diagnostic procedure based on a clinical reasoning process that provides insight into a patient’s condition and a patient’s self-perceived health problems. PT diagnosis is defined as ‘a specific professional opinion on the health status of the patient, related to the underlying suffering and based on data from referral, history taking and clinical examination supplemented by medical and psychosocial data’ [1]. This definition of PT diagnosis is embraced by the World Confederation of Physical Therapy (WCPT) and is constructed according to the biopsychosocial model [2]. In cooperation with the patient, the aim of a PT diagnosis is to determine the indication for treatment, the strategy of most appropriate therapeutic care and the outcome prognosis [3, 4, 5]. For manual physical therapists (MPTs) working in primary care, very often there is only limited information available about the course of musculoskeletal pain, particularly in patients with chronic low back pain (LBP). Referral data are often superficial or the patient is the only source of information due to self-referral. MPTs in primary care practice also reported infrequent interactions with other health professionals, particularly with psychologists [6].
Most patients with chronic LBP will be treated in a primary care manual physical therapy practice in The Netherlands. Psychological factors, such as fear-avoidance beliefs and kinesiophobia, worsen the course and prognosis of LBP but are currently under-recognized and undertreated in manual physical therapy primary care practice [7, 8, 9, 10, 11].
With increasing evidence supporting the importance of psychological factors in manual physical therapy [12], a fundamental question concerns the extent to which MPTs can identify specific psychological risk factors related to fear-avoidance beliefs. In patients with (chronic) LBP these are possibly one of the most prominent psychological factors underlying chronicity [13, 14, 15]. Identification of fear-avoidance and other psychological factors in physical therapy is mostly based on clinical perception during the clinical reasoning process, without the use of validated measures in the diagnosis of factors such as fear-avoidance beliefs in patients with LBP [7, 16, 17]. Kori et al. [18] introduced the term ‘kinesiophobia’, defining it as ‘an excessive, irrational, debilitating fear of physical movement and activity resulting from a feeling of vulnerability to painful injury or re-injury’. The Tampa Scale for Kinesiophobia (TSK) is very often used as a validated patient reported outcome measure for kinesiophobia.
Across many domains there is a well-known lack of agreement between clinician interpretation and identification and patient-completed measures, and between attitudes and beliefs regarding psychosocial aspects of LBP and reported clinical behaviour [19, 20]. Agreement between the physician or (manual) physical therapist and the patient regarding diagnosis, diagnostics and the treatment plan has been associated with higher patient satisfaction and better health status outcomes in patients with LBP [21, 22]. A discordance between a patient’s cognitive-affective response to pain (i.e., LBP) and clinician-interpretation and judgment of fear-avoidance beliefs may result in low therapeutic alliance and hence a lack of an effective treatment plan and intervention.
To the best of our knowledge, only one published study has evaluated whether physical therapists are able to identify fear-avoidance beliefs in patients with LBP [23]. In this study, the ratings of physical therapists were compared to validated patient questionnaires (Fear Avoidance Beliefs Questionnaire [FABQ], Tampa Scale for Kinesiophobia [TSK] and Pain Catastrophizing Scale [PCS]), with the results showing no association between therapists’ ratings of perceived patient fear-avoidance and the questionnaire data, thus indicating a potential discordance between therapist judgments and commonly used patient reported fear-avoidance beliefs measures [23]. These findings emphasized the need for further study of the ability of MPTs, using a semi-structured interview during history taking, to identify the fear-avoidance beliefs of patients with LBP and to compare this clinician identification with patient completed measures.
In the diagnostic process preceding manual physical therapy, history taking is the most feasible procedure during the first consultation and can be used to generate both a comprehensive picture of the perceived health problems of a patient with LBP and as starting point for an individual treatment plan. Information on psychological factors can often be gathered during history taking by asking open and semi-structured questions such as ‘Which activities are hindered by your LBP’? (to trace impairments of movement-related functions and activity limitations), ‘What are your thoughts when you are experiencing LBP’? (to trace catastrophic cognitions, fear of pain and lack of self-efficacy), ‘What are your feelings when you experience back pain’? (to trace depression or anxiety) and ‘What do you do in response to LBP’? (to trace avoidance behaviour or pain resistance behaviour). The method underlying a (semi-)structured history taking, such as the often-used Somatic Cognitive Emotional Behavioural Social (SCEBS) method [24], is crucial as a first orientation on the prognostic psychological factors that may have influenced the course of a patient’s LBP. The assumption is that MPTs are competent in recognising kinesiophobia in patients with (chronic) LBP, in combination with other psychological factors.
The aim of this study was to evaluate the association between the scores and score accuracy with which MPTs working in primary care identify kinesiophobia in patients with LBP, using a Visual Analogue Scale for estimation (VAS-est) and for accuracy (VAS-ac), and the patients’ self-reported measures of kinesiophobia, using TSK. The scores for the MPT’s estimates were compared with scores obtained from the authorized and validated Dutch version of the TSK-17 [25] completed by participating patients with LBP.
Materials and methods
Study design
The design of the study was cross-sectional. The Medical Ethics Committee of Radboud University Medical Centre Nijmegen, The Netherlands, stated that obtaining ethical approval was not necessary for the present study.
Participants
An invitation to participate in the study was sent to 50 MPTs working in primary care practices in the south of the Netherlands, of whom 36 (72%) indicated interest (Fig. 1). These MPTs participated in a regional information session that outlined the purpose and content of the study and the expected contribution. Out of 36 interested MPTs, 17 (47.2%) registered for the study. These MPTs were asked to collect data during a period of six weeks on at least six patients with nonspecific LBP, preferably on the first patient each week who was referred or self-referred for the first time or who presented with a new episode of LBP and met the inclusion criteria. Based on the number of participating MPTs (
Patients had to meet the following criteria for inclusion as the best reflection of primary care practice: age 18–80 years and non-specific LBP (defined as LBP without a specific cause of the pain, e.g., systematic disease or organic disorder), no treatment in the previous three months by the same MPT, and the ability to read and understand Dutch questionnaires. Patients with a history of additional complaints, such as non-radicular pain, were only included if LBP was the dominant symptom. Patients whose history showed signs and symptoms suggested potential non-benign LBP (including previous lumbar surgery) or a specific pathologic condition (such as malignancy, neurologic disease, herniated disc, or rheumatic disease) were excluded. Patients were informed about the purpose and content of the study and their expected contribution. Patients gave oral informed consent.
Procedure
A semi-structured interview during the first consultation took place at the manual physical therapy practice. The MPTs were asked to complete a general questionnaire assessing demographic and professional characteristics. At the end of the first consultation, they rated their perception and identification of fear of (re-)injury due to movement and physical activity based on their own conclusions and interpretation of patient’s answers during history taking, and rated their own accuracy regarding patient’s kinesiophobia. The MPTs were blinded to the self-reported measures completed by the patients.
The patients were asked to complete a general questionnaire assessing demographic characteristics and duration of LBP. Patients were also asked to fill out the TSK-17 prior to history taking with the MPT. The completed questionnaire and the TSK-17 were kept by the practice secretary in separate sealed envelopes and returned to the investigator.
Measures
Demographic and biographical variables of patients and MPTs
The demographic questionnaire for patients included data regarding gender, age (years) and LBP duration (0–6, 7–12 and
Familiarity of MPTs with kinesiophobia and Tampa Scale for Kinesiophobia
The knowledge and familiarity of MPTs with the theoretical concept of kinesiophobia were tested with 8 expert-based multiple choice questions (score 0–8) (Appendix). Based on a consensus amongst experts (
Tampa Scale for Kinesiophobia
Patients filled out the Dutch version of the TSK-17 [25]. The TSK-17 is a questionnaire that includes 17 items that identify fear of (re-)injury due to movement and physical activities. Items are scored on a 4-point Likert scale with score 1 representing ‘strongly disagree’ and score 4 ‘strongly agree’. Total scores, ranging from 17 (no kinesiophobia) to 68 (extreme kinesiophobia), were calculated (which included reversing the scores for items 4, 8, 12 and 16). For patients with acute and chronic LBP, the psychometric properties of the Dutch version of the TSK-17 are good [25, 26] and a score of
Visual analogue scales for estimation and accuracy
MPTs rated their perceptions of a patient’s fear of (re-)injury due to movement and physical activities using the VAS-est (0
Statistical procedure
Descriptive statistics were used for MPT and patient characteristics in terms of frequency, mean, standard deviation, range and median. Patient’s (gender, age, and duration of LBP) and MPT’s (gender, age, clinical experience, familiarity of concept, and estimated accuracy) relevant variables in relation to the scores on TSK-17 and the VAS-est were divided into subgroups based on the medians. Kendall’s tau-b (
Flowchart of manual physical therapists’ (MPTs) responses and reasons for no interest, dropouts and missing.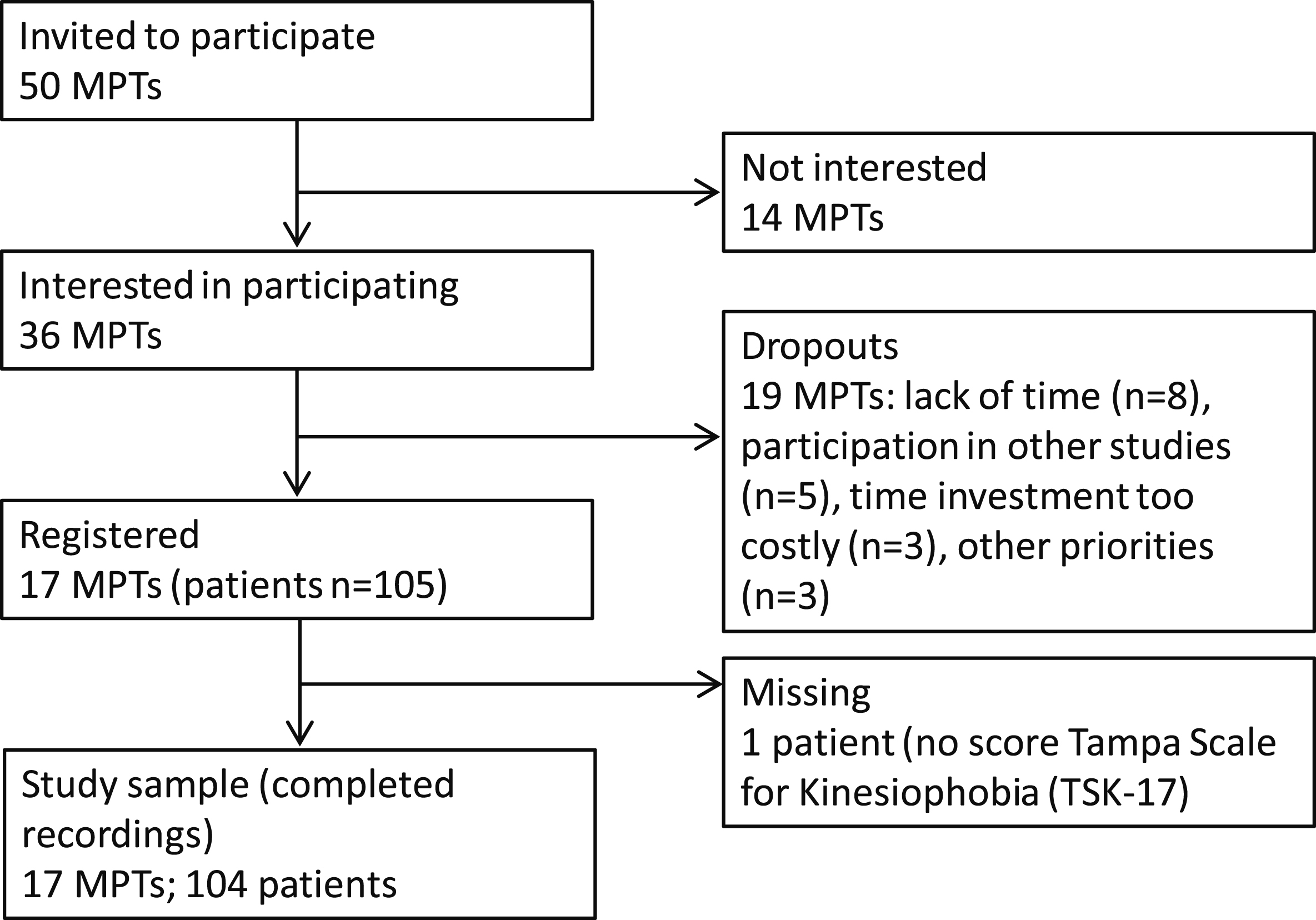
Response rates
All registered MPTs (
Therapist demographic and professional characteristics (
17)
Therapist demographic and professional characteristics (
Abbreviations: SD: Standard Deviation; MT: Manual Therapy; MSc: Master of Science; MPT: Manual Physical Therapy; LBP: Low Back Pain; TSK: Tampa Scale for Kinesiophobia.
The mean age of the MPTs was 41.4 years (SD
Patient demographic and self-rating measures (
104)
Patient demographic and self-rating measures (
Abbreviations: SD: Standard Deviation; wk: week; TSK-17 (17–68): Tampa Scale for Kinesiophobia (17
The patients’ mean age was 44.5 years (SD
The mean scores for the MPTs on the VAS-est and VAS-ac were 34.2 mm (SD
Median subgroups’ relationship between Tampa Scale Kinesiophobia (TSK-17) and Visual Analogue Scale estimation (VAS-est) in patients with low back pain (
104)
Median subgroups’ relationship between Tampa Scale Kinesiophobia (TSK-17) and Visual Analogue Scale estimation (VAS-est) in patients with low back pain (
Abbreviations: med
The TSK-17 scores showed a ‘fair’ association with the VAS-est scores (Kendall’s
Associations between the MPT’s ratings for VAS-est and the patient’s ratings for TSK-17 were ‘fair’ (Kendall’s
Discussion
Main findings
The present study showed only ‘fair’ associations between the MPT’s perception of kinesiophobia and patient’s self-reported kinesiophobia, suggesting some discordance between the clinician’s perception and identification of, and the scores obtained from a valid patient reported measure for kinesiophobia (TSK-17). Based on their self-reported knowledge of and familiarity with kinesiophobia, the participating MPTs felt sufficiently confident with the construct of kinesiophobia and therefore estimated the accuracy of their own ratings as sufficient. The correlation coefficient for VAS-est and VAS-ac was moderate.
The perception of a patient’s fear of (re-)injury due to movement and physical activities was measured with the VAS-est and the accuracy of the ratings was determined with the VAS-ac. The VAS is a standardized instrument (100 mm) that can measure different variables with high test-retest reliability and criterion-related validity, particularly pain [27, 28]. Based on the content and face validity, we used the VAS-est and the VAS-ac in this study under the assumption that the psychometric properties of the VAS are relevant for diverse variables. However, further research into the psychometric quality of the VAS-est and the VAS-ac is desirable.
All correlation coefficients for TSK-17 and VAS-est ranged between 0.25 to 0.50 (fair), except for the correlation of the TSK-17 and the VAS-est in patients with subacute LBP (7–12 weeks) (moderate). There were only minor differences within the range ‘fair’ between the correlation coefficients for the median subgroups ‘clinical experience’ in favour of the MPTs with clinical experience
These variables were related to the professional characteristics of MPTs with a more recently completed education and greater confident with the construct of kinesiophobia. Overall, there is considerable room for improvement in the implementation of current knowledge about psychological factors in manual physical therapy primary care, particularly fear-avoidance beliefs and kinesiophobia in managing patients with (chronic) LBP.
Discordance between therapist ratings and patient reported measure of kinesiophobia
Clinician’s ability to identify psychological factors, such as fear-avoidance beliefs, has been reported to be poor in comparison with formal screening tools. One (less plausible) explanation of the results of this study could be that the participating MPTs were consistently incorrect in interpreting the fear-avoidance beliefs of participating LBP patients. The most obvious reason is that the focus of MPTs in relation to patients with (chronic) musculoskeletal pain is mostly oriented towards impairments of body functions and structures, focusing particularly on structures related to movement and on neuromusculoskeletal and movement-related functions and pain, rather than considering the psychological aspects of pain [19, 30].
Another more plausible interpretation of the (only) fair associations between MPT and patient-reported measures of kinesiophobia is that the MPT’s perception of a patient’s kinesiophobia considered additional facets of the complex construct of kinesiophobia, facets that were not captured by the TSK-17 including patient non-verbal expressions and the use of characteristic words and behaviour during history taking. In addition, the MPT ratings may have been influenced during history taking by different but related theoretical constructs, such as pain catastrophizing, fear avoidance, disability and disuse.
The discordance in this study between the MPT’s perceptions of a patients’ kinesiophobia and patient-completed measures of kinesiophobia could form the basis of a discussion of the concurrent validity of the TSK-17 with the clinical identification of patients’ kinesiophobia. The findings of the present study are consistent with the study findings of Calley et al. [23] and Beales et al. [31]. These authors also found negligible to only fair associations between therapist ratings and patient-completed measures. These findings are also consistent with previous studies in which only fair associations were identified between clinician judgments and other psychosocial factors [20, 32, 33].
Familiarity with construct of kinesiophobia
All participating MTPs had many years of clinical experience in primary care practice and in the assessment of patients with acute, subacute and chronic LBP. Due to this clinical experience, their familiarity with patients with LBP is preserved in memory patterns that facilitate efficient communication with their patients [4, 5]. It is likely that the participating MPTs were able to recognize and identify psychological factors. Most of the MPTs were sufficiently familiar with the theoretical construct of kinesiophobia but unfamiliar with the TSK-17, and did not use the TSK-17 in practice. Therefore, their perception and identification of patient’s kinesiophobia and the accuracy of their ratings were probably based on recognition of clinical patterns in patients with LBP. However, these clinical patterns are only implicit rather than explicit in this study and it would be beneficial to elucidate these patterns with greater transparency, including the influence of attitudes and beliefs of MPTs on the management of patients with LBP [32, 34, 35, 36].
Severity of kinesiophobia
The TSK-17 provides information on the severity level of kinesiophobia, and a score of
Clinical impact of discordance
The discordance between MTP perceptions and patient reported measures of kinesiophobia may result from suboptimal communication between the MPT and the patient and from over- to under-recognition and from over- to under-treatment of kinesiophobia in patients with (chronic) LBP. Improving this communication may improve recovery from LBP and increase patient satisfaction. This discordance between MPT perceptions and patient measurements of kinesiophobia is only one aspect in the dynamic process of clinical reasoning. However, it remains a very important feature because the presence or absence of kinesiophobia as a prognostic factor for chronicity of LBP may impact the intervention strategy and the choice of treatment modalities. It is difficult to choose an adequate treatment plan and intervention strategy based only on patient-completed measures of kinesiophobia or the identification of kinesiophobia by the MPT. Additional information on other aspects of kinesiophobia is needed to facilitate optimal communication between patient and MPT, and to allow the formulation of an adequate treatment plan, intervention strategy and treatment modality.
The TSK-17 provides little information on specific activities relevant to patient pain-related fear (such as limitations in changing and maintaining body position, carrying, moving and handling objects, and walking and moving). In contrast, the International Classification of Functioning, disability and health (ICF) core set for low back pain provides detailed information on body functions, activity limitations and participation restrictions, particularly for patients with LBP [37, 38, 39, 40]. If a patient experiences pain-related fear related to only one or a few activities (e.g., lifting, bending, carrying or prolonged sitting), the patient, upon re-exposure to the feared activity, can reduce pain-related fear of (re-)injury [41, 42, 43]. The use of 100 standardized photographs (PHODA
Limitations of the study
The response rates of practices, MPTs and patients were low. Although the MPT sample was comparable to the non-registered MPTs and to the national average [46], and the patients sample to participants in another Dutch study [47], the low number of participating MPTs may have led to selection bias and thus limited the external validity of the study findings. A major concern for future studies should be increasing the response rates, which would substantially enhance the generalizability of the study findings.
Most MPTs work in a primary care setting as individual practitioners. Gaining a comprehensive understanding of an individual patient with (chronic) LBP is very important and at the same time very difficult because of the poor availability of clinical data prior to the MPT visit. Just over 50% of the patients included in this study had experienced LBP for more than 13 weeks and could be considered to have chronic LBP. It can be reasonably assumed that the patients would have seen other health professionals, such as a family physician or another physical therapist, prior to their enrolment. However, at the moment of the first appointment relevant data on earlier diagnostic procedures and treatments are often unavailable, referral data are often superficial or the patient is the only source of information due to self-referral.
Few data are available on the sharing of information and referral prior to an MPT visit. Very little attention has been paid in literature to the inter-professional sharing of information with MPTs working in primary care, particularly with those managing patients with (chronic) LBP. Based on a qualitative study [48], one recently published study described the inter-professional character of private physiotherapy practice in Canada [6]. Besides frequent contact with physiotherapists and family physicians (daily/weekly via written and oral messages sent through patients), the frequency of inter-professional interaction with psychologists was very low. There is, clearly, room to increase inter-professional sharing information in primary care settings.
This may also limit the generalizability of this data to MPTs working in other settings, for example, rehabilitation settings for patients with chronic pain. Only one of the participating MPTs was working in a rehabilitation setting. In this setting, a multidisciplinary team of health professionals with extensive knowledge of the course of LBP allows for a mutual support network for every member of the team. In the Netherlands, many MPTs practise in primary care and most patients with chronic musculoskeletal disorders (such as LBP) will be treated in a primary care manual physical therapy practice, with the attendant limitations of availability of clinical information. Therefore, the open and semi-structured interview during history taking provides an opportunity to develop a comprehensive picture of each patient with (chronic) LBP. In this study, we had no control over the content of history taking. There are indications that history taking by MPTs tends towards the somatic rather than the psychological [7, 24]. We recommend that, in addition to their extensive history taking, MPTs who manage patients with (chronic) LBP use validated questionnaires to screen for fear-avoidance belief and kinesiophobia. Systematic use of these questionnaires would improve the MPT’s ability to estimate these psychological factors with greater accuracy and thus help provide more appropriate management to patients with (chronic) LBP.
The identification of patient’s kinesiophobia was only based on history taking by the MPTs as a narrow aspect of the dynamic clinical reasoning process and their perception was measured using VAS-est. It should be noted that history taking by MPTs is mainly characterized by querying bio-medically oriented factors in relation to LBP [7, 24, 49, 50, 51]. and does not sufficiently address psychological factors as recommended in systematic reviews and in national and international LBP guidelines [9, 10, 11, 52, 53, 54, 55]. It may be worthwhile to develop a more comprehensive clinical tool that includes history taking and which captures the physical activity-related behavioural aspects of pain-related fear of (re-)injury during a clinical examination. A more comprehensive clinical tool might more consistently reflect the multidimensional construct of kinesiophobia and other related psychological factors.
In addition to many years of clinical experience, most participating MPTs were educated in the biomedical model of pain. In the context of this study no specific training was provided in the identification of psychological factors that correlate with pain-related fear of (re-)injury or kinesiophobia, so that the unbiased identification of patient’s kinesiophobia could be assessed. Perhaps better education of MPTs in the recognition and identification of pain-related fear factors, in combination with patient reported measures, followed by the incorporation of these factors in movement and activity-related programs (such as graded exposure in vivo programs) would improve the association between the MPTs’ perception and accuracy and patient-reported measures of kinesiophobia.
Conclusion
In summary, in patients with LBP the association between an MPT’s perception of a patient’s kinesiophobia and a patient’s self-reported kinesiophobia in a primary care setting were rated as fair. We would now encourage MPTs not to rely solely on their personal clinical perception of a patient’s kinesiophobia, but also to use validated self-reported measures such as the TSK-17 to supplement their clinical judgment. Further studies including larger patient numbers and a wider range of scores that cover the full severity of the TSK-17 are needed to explore the associations between clinician perception and patient’s self-reported kinesiophobia in relation to musculoskeletal pain, particularly LBP.
Conflict of interest
None to report.