
Abstract
STUDY DESIGN:
A prospective observational comparative study.
BACKGROUND:
Because epidural corticosteroids are more effective for pain relief when delivered close to the site of pathology, lumbar spinal stenosis with multilevel stenotic areas can be treated more effectively when medications cover all of the stenotic areas. Distribution of medications to the pathologic sites is considered an important factor in the effectiveness of inter-laminar epidural injection.
OBJECTIVE:
To determine whether spread of a lidocaine and triamcinolone mixture over the stenotic areas improves clinical symptom of spinal stenosis more effectively.
METHODS:
Twenty-four patients with lumbar spinal stenosis were enrolled in this study. A lumbar inter-laminar epidural injection under fluoroscopic guidance was administered to each patient. A numeric rating scale (NRS), claudication distance, the Romberg test, and the Oswestry Disability Index (ODI) were checked pre-injection and at 2, 6, and 12 weeks after the epidural injection. Vertebrae that showed more than moderate stenosis were considered stenosis levels. Inter-laminar epidural injection was performed with radiopaque contrast and lidocaine mixed with triamcinolone acetate. When the contrast covered all of the stenosis levels, this was considered a sufficient distribution (SD) and when the contrast did not cover all stenosis levels, this was considered an insufficient distribution (ID).
RESULTS:
At 2 weeks, percentages of NRS improvement were 71.4 (IQR, 20.2) in SD group and 50.0 (IQR, 31.4) in ID group (
CONCLUSION:
Coverage of the stenotic area by the lidocaine, triamcinolone, and contrast dye mixture during inter-laminar epidural injection was an important predictor of acute pain reduction.
Introduction
Spinal stenosis involves narrowing of the spinal canal and causes symptoms of neurogenic claudication [1]. Many nonsurgical treatments have been evaluated, including medications, physiotherapy, and epidural steroid injection [2]. However, high- and moderate-grade evidence for these treatments is lacking [3] and no definitive clinical guidelines have been suggested to date.
Epidural injection is a procedure in which soluble agents, such as, local anesthetics or steroids are injected into the epidural space by transforaminal, inter-laminar, or caudal approaches to control pain. Among these, inter-laminar epidural injection is most commonly performed, and shows short term pain relief in cases of herniated cervical or lumbar disc, spinal stenosis, discogenic pain, and radiculopathy [4]. Because the inter-laminar approach spreads medications to multiple levels of the lumbar spine [5], it is a good choice in cases of diffuse targets, such as multilevel spinal stenosis [6].
The efficacy of inter-laminar epidural injection in lumbar spinal stenosis depends on a number of factors, including age and sex [7]. The severity of lumbar spinal stenosis has a debatable correlation with clinical improvement due to epidural injection [7, 8, 9]. Because epidural corticosteroids are more effective for pain relief when delivered close to the site of pathology [10], lumbar spinal stenosis with multilevel stenotic areas can be treated more effectively when medications cover all of the stenotic areas. In cases of lumbosacral radicular pain, parasagittal inter-laminar epidural injection is more effective for pain relief than midline inter-laminar epidural injection because the needle tip is closer to the pathologic lesions [11]. Therefore, distribution of medications to the pathologic sites is considered an important factor in the effectiveness of inter-laminar epidural injection.
We hypothesized that if the contrast dye covered the stenotic areas, inter-laminar epidural injection would be more effective in relieving pain associated with spinal stenosis. Therefore, the aim of this study was to determine whether coverage of the contrast dye over stenotic areas results in greater improvement of the clinical symptoms of spinal stenosis.
Methods
Patients
This was a prospective observational comparative study. Patients were recruited from our outpatient department who were diagnosed with spinal stenosis confirmed by magnetic resonance imaging (MRI) from March 2012 to November 2012. Inclusion criteria were 1) claudication symptoms and signs irrespective of low back pain, 2) no resolution of pain by medication or physical modalities, 3) central stenotic regions revealed by lumbosacral MRI, 4) neither hip joint nor vascular problem by physical examinations, 5) no previous intervention within 3 months before enrollment, 6) no previous lumbosacral surgery, and 7) no contraindication for the epidural injection, such as, pregnancy or acute infection. Epidural fibrosis has been reported in over 80% of patients after surgery [12]. Therefore, we excluded patients who underwent lumbosacral surgery.
All patients gave written consent for this procedure, and their information was acquired. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Parameters
A numeric rating scale (NRS) ranging from 0 to 10, claudication distance, the Romberg test, and the Oswestry Disability Index (ODI) were measured pre-injection and at 2, 6, and 12 weeks after epidural injection. The version of the ODI was the same as that used in a previous study [13]. Percentage (%) of NRS improvement after the epidural injection was expressed as the changes of NRS divided by the initial NRS. Percentage (%) of NRS improvement at more than 70% was considered as ‘more effective in NRS’. Less than 70% NRS improvement was considered as ‘less effective in NRS’. A decrease of ODI of more than 8 or less than 8 was considered as ‘more effective in ODI’ or ‘less effective in ODI’, respectively. We determined the criteria of responder as 8 point according to a previous study in which median difference of ODI between ‘better’ group and ‘worse’ group was 8 [14]. Basic patient information was collected, including height and body weight. Claudication distance was measured on the treadmill with a usual walking speed ranged from 5 to 6 km per hour until the symptoms were reported. The Romberg test was measured as time to failure (seconds) in the eyes-closed state and on firm ground to evaluate proprioceptive function [15]. All the parameters were checked by one physiatrist who did not participate in the analysis of MRI and fluoroscopic images for the prevention of bias.
All patients underwent lumbosacral MRI, and the level of central stenotic areas was judged by morphological grading. Stenosis was classified into none, mild, moderate, or severe as described in a previous study [16], and when the spinal canal showed more than moderate stenosis and matched the clinical symptom level, that level of the spine was considered the stenosis level.
Epidural injection technique
Inter-laminar epidural injection was performed in the lateral decubitus position with the lumbar spine flexed to widen the interspinous area. One percent chlorhexidine and lidocaine solutions were used for sterilization and anesthesia of the skin respectively around the lower lumbar area. After confirmation of the L3-4 level by fluoroscopy (SONIALVISION Safire 2; Shimadzu, Kyoto Japan), a 20-gauge Tuohy needle (Contiplex
Inter-laminar epidural injection was performed at the L3-4 level and the degree of contrast spread was measured as a real distance (mm) using PACS image calipers. Contrast was sufficiently distributed over the stenotic area (1A) and insufficiently distributed over the stenotic area (1B).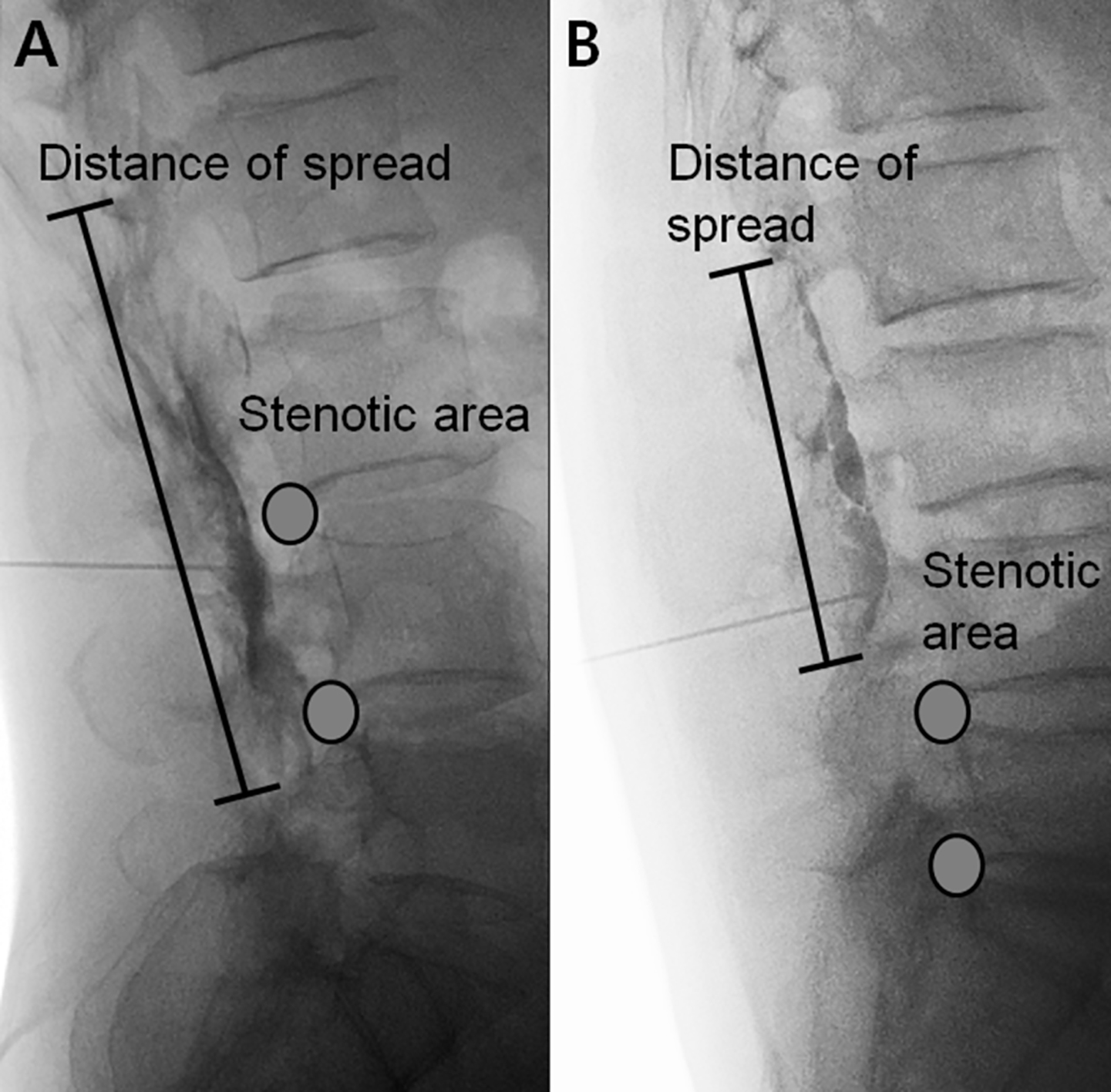
All patients were asked not to change their current medications to determine the accurate effect of inter-laminar epidural injection. Their medications were nonsteroidal anti-inflammatory drugs or gabapentin or both.
When the contrast covered all of the stenosis levels, this was considered sufficient distribution (SD) (Fig. 1A) and when the contrast did not cover all stenosis levels, this was considered insufficient distribution (ID) (Fig. 1B). To prevent bias, the patients did not receive any information about the groups they belonged to.
To determine the difference in clinical improvement between SD and ID, the difference in ODI values at 2 weeks was set as the primary outcome and subjected to Mann-Whitney U test. Changes in other parameters were also compared between the two groups using Mann-Whitney U test. To determine the correlation between effectiveness and contrast distribution, chi-square tests were performed. To identify the correlation between clinical improvements and contrast distribution, Pearson’s correlation analysis was conducted. The SPSS 22.0 software (IBM SPSS Statistics; IBM Corporation, Somers, NY) was used for the statistical analysis, and a
Stenotic levels that reflected more than moderate stenosis in the MRI were considered stenosis.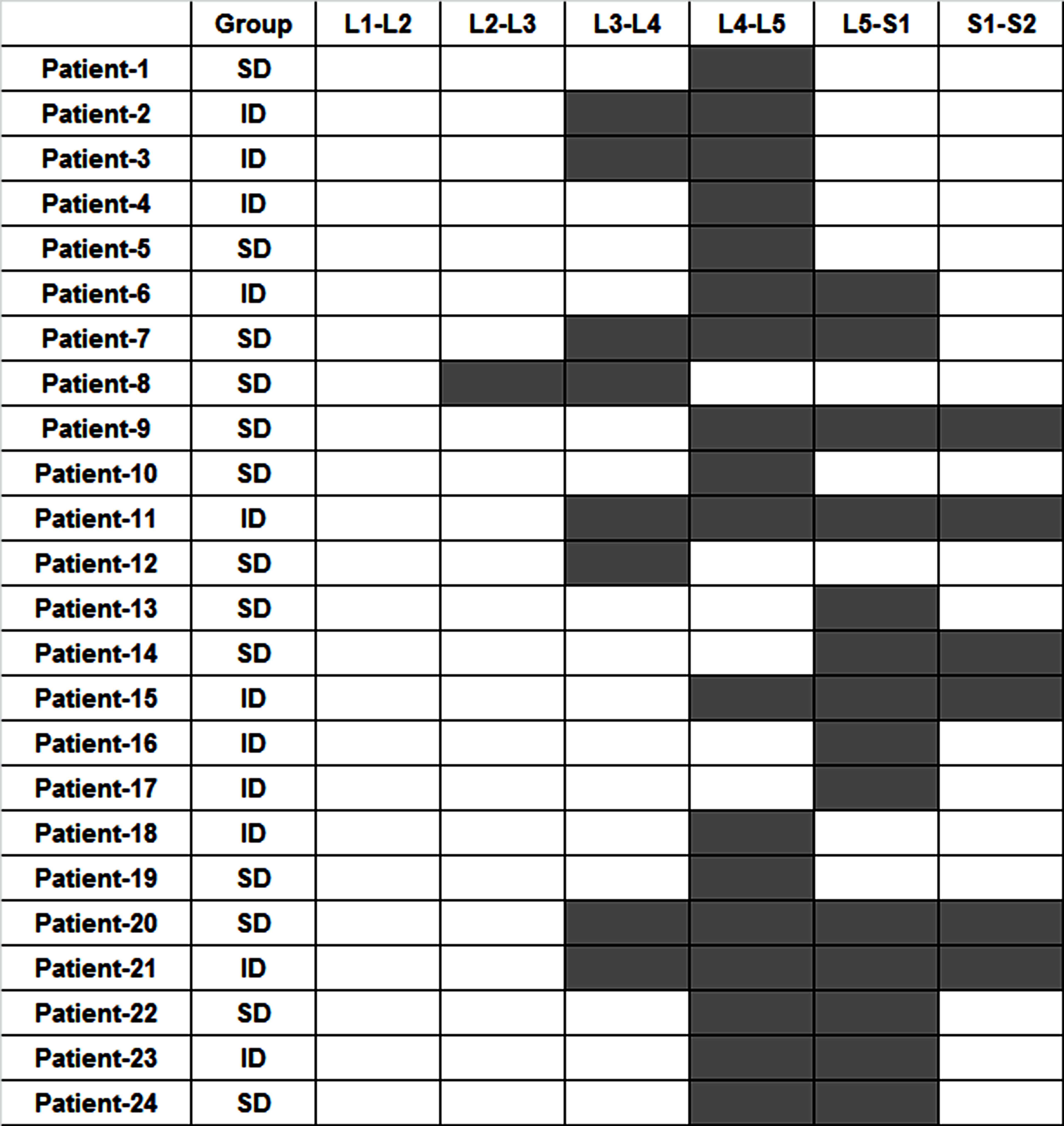
A total of 24 patients participated in our study, comprising 6 males and 18 females (average height 151.1 cm with one standard deviation 30.0), their average age was 67.5
Central stenotic levels as shown on MRIs ranged from L2-3 to L5-S1; the distribution is presented in Fig. 2. After inter-laminar epidural injection, contrast was distributed along the epidural space at an average distance of 53.2
When the patients were divided into two groups (SD and ID), initial NRS, initial claudication distance, initial Romberg test time, and initial ODI were not significantly different between the groups. At 2 weeks, percentages of NRS improvement were 71.4 (IQR, 20.2) in SD group and 50.0 (IQR, 31.4) in ID group (
Box plot graph showing the percentage of numeric rating scale (NRS), change of Romberg test, decrease of Oswestry Disability Index (ODI), and change of claudication distance 2 weeks after the inter-laminar epidural injection in sufficient distribution (SD) and insufficient distribution (ID) groups.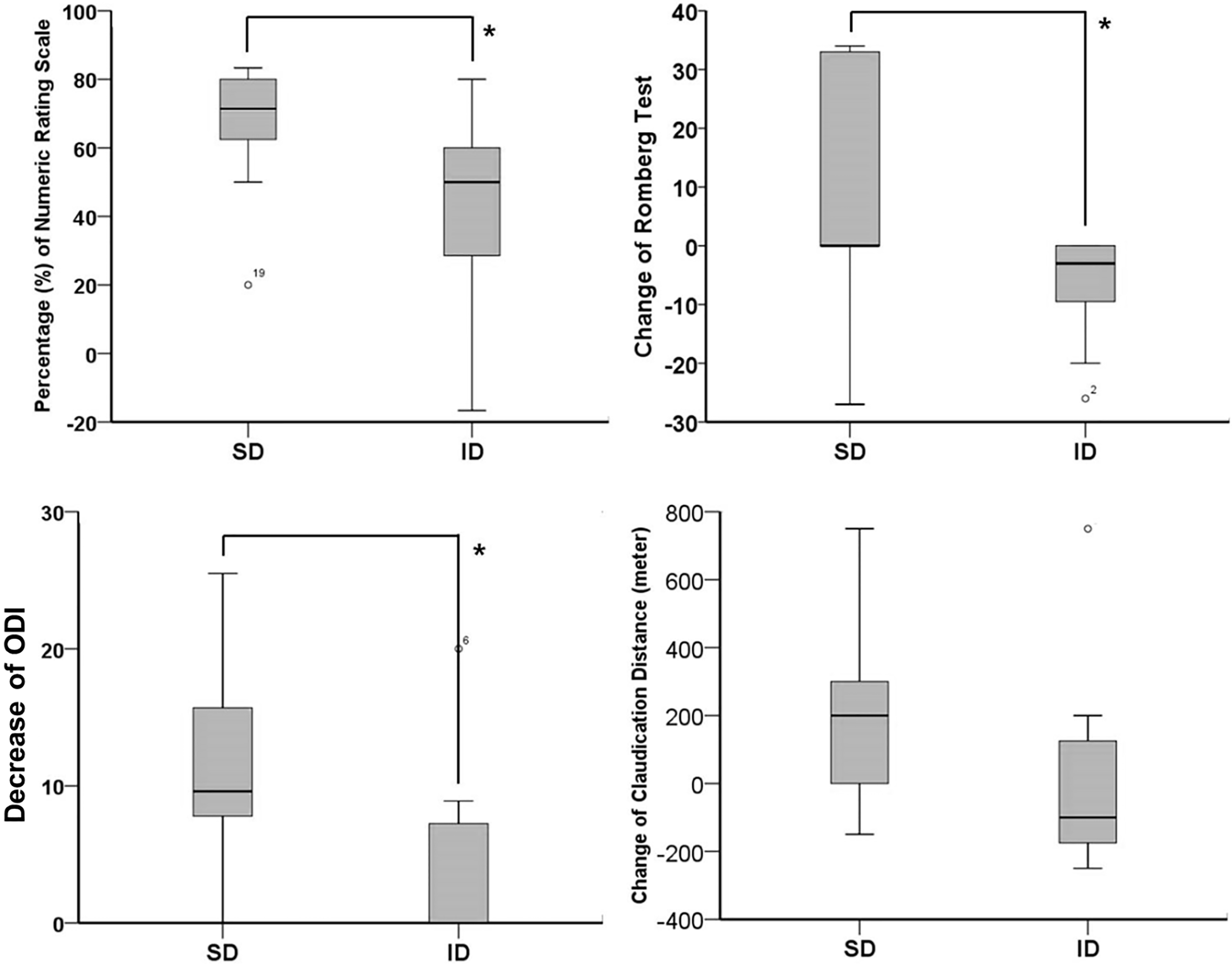
Box plot graph showing the percentage of numeric rating scale (NRS), change of Romberg test, decrease of Oswestry Disability Index (ODI), and change of claudication distance 6 weeks after the inter-laminar epidural injection in sufficient distribution (SD) and insufficient distribution (ID) groups.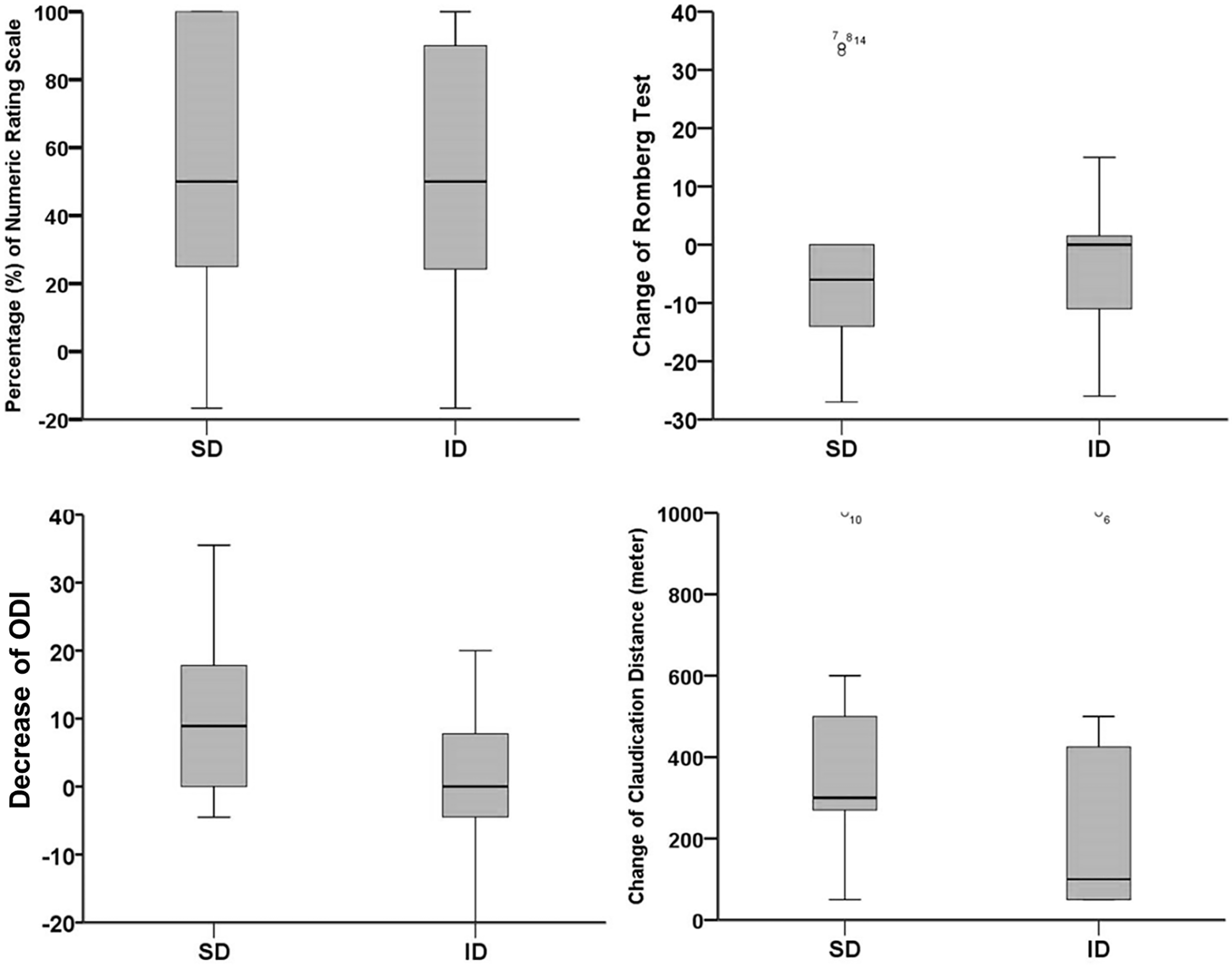
Box plot graph showing the percentage of numeric rating scale (NRS), change of Romberg test, decrease of Oswestry Disability Index (ODI), and change of claudication distance 12 weeks after the inter-laminar epidural injection in sufficient distribution (SD) and insufficient distribution (ID) groups.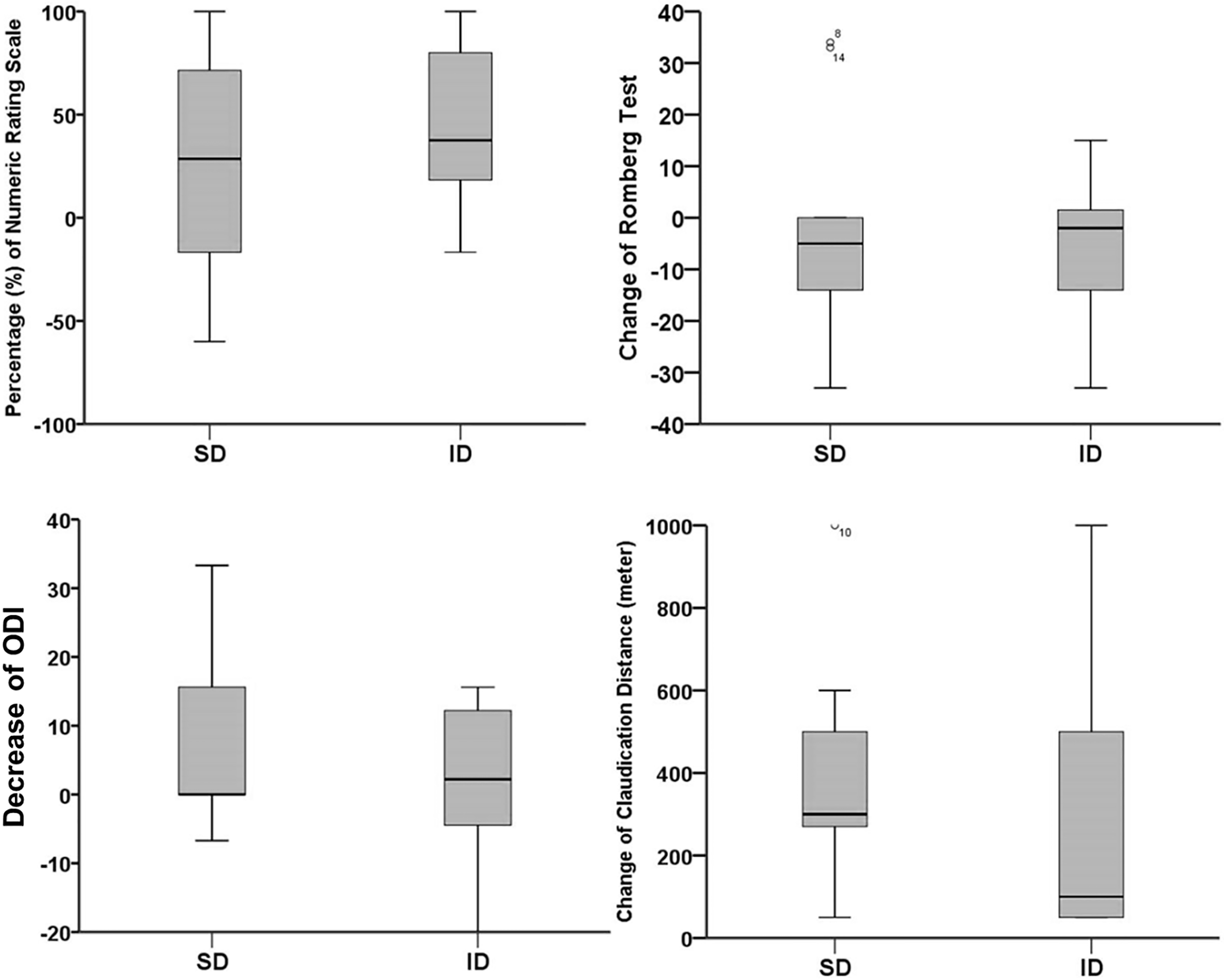
Both groups showed significant change of NRS (F
At 2 weeks after the injection, 7 patients in the SD group showed ‘more effective in NRS’ and 6 patients showed ‘less effective in NRS’. In the ID group, only one patient showed ‘more effective in NRS’ while 10 patients showed ‘less effective in NRS’, which was significantly different (
Number of patients who showed ‘more effective’ and ‘less effective’ in numeric rating scale (NRS) and Oswestry Disability Index (ODI) at 2 weeks, 6 weeks, and 12 weeks after the interlaminar epidural injection according to the contrast distribution
Sufficient distribution (SD) was defined when the contrast covered all of the stenosis levels and insufficient distribution (ID) when the contrast did not cover all stenosis levels.
The average distance (mm) of the contrast distribution showed no correlation with the percentage of NRS improvement, change of claudication distance, change of Romberg test, or decrease of ODI at any time point; the correlations between the distances of contrast distribution and all clinical parameters at 2 weeks are presented in Fig. 6.
Correlations between the distance of contrast distribution and changes in the numeric rating scale (NRS), claudication distance, Romberg test, and Oswestry Disability Index (ODI) at 2 weeks. There were no significant correlations between the distance of contrast distribution and any of the parameters.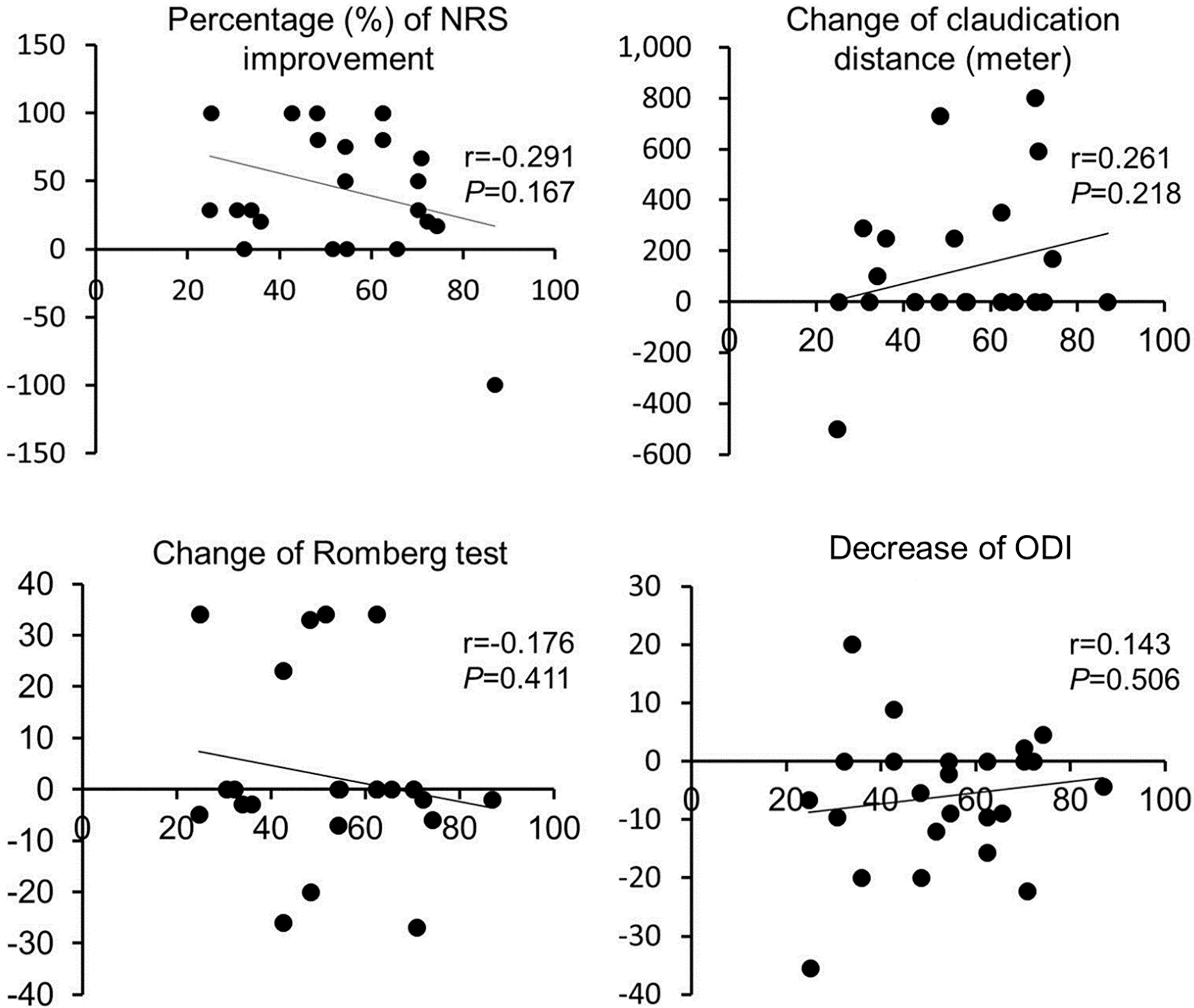
In our study, we found that a contrast distribution that covered the stenotic area showed greater short term reduction in pain with the inter-laminar epidural injection than did insufficient distribution over the stenotic area. Moreover, a wide contrast distribution that did not cover the stenotic area did not show better results, emphasizing the importance of the accurate distribution of contrast in spinal stenosis.
Injected materials for inter-laminar epidural injection at L3-4 traveled one or two vertebral levels caudad or cephalad, which always included the most stenotic level in our cases. We used the same volume of injected materials in all patients, but the distribution range varied. This might be due to needle tip position, gender, lumbar lordosis, operative history, and degree of stenotic areas according to previous studies (5, 8, 18). We performed the inter-laminar epidural injection in the lateral position instead of prone position because the fluoroscopy could not be rotated during the procedure.
We used 8 ml of the mixture of lidocaine and triamcinolone acetate in the inter-laminar epidural injection by midline approach. This amount was enough to cover the posterior and anterior parts of epidural space in all the patients, which would reduce the pain from central canal stenosis caused by facet joint hypertrophy or disc problems if the stenotic level was covered by the drugs.
In terms of the correlation of contrast distribution on clinical improvement, our results are consistent with a study by Manchikanti [19] in which inter-laminar epidural injection was found to be superior to caudal epidural injection in treating lumbar central spinal stenosis because caudal epidural injection might not reach the target level. Milburn reported that inter-laminar epidural injection was most effective when performed at the maximal stenotic level, which supports our findings [10]. Cosgrove [7] suggested that successful response was not related to the severity of stenosis on MRI, which contradicts our results. Our study suggested that distribution of contrast to a more than moderate stenotic level was important for pain reduction. The study by Cosgrove [7] and Kuittinen [20] focused on the canal dimension area, not the stenotic level, and this contradiction can be explained by the fact that the symptom was not related to the canal dimension area but the stenotic level.
Four patients in SD group and four patients in ID group had stenotic areas at the level of L3-4, the injection site. In the SD group, stenotic areas ranged from L2-3 to S1-2. In the ID group, the stenotic areas ranged from L3-4 to L5-S1. Therefore, the superior effect in the SD group might not be due to close direction of medications into the stenotic areas.
In our study, all clinical symptoms in both groups were improved over time, with the exception of Romberg test time. A systematic review performed by Ammendolia showed that the evidence for surgical and non-surgical treatment to improve walking ability was of low and very low quality [21], which might explain the inconsistent effect of inter-laminar epidural injection on the claudication distance in our study.
Unexpectedly, Romberg test time in ID group decreased at 2 weeks after the injection, which was significantly different in paired t-test (
Median value of claudication distance change in ID group also decreased at 2 weeks after the injection. This paradoxical decrease might be due to the skewness of data and small sample size because its mean value increased to 4.5 meter. Claudication distance between baseline and 2 weeks after the injection was not significantly different in paired t-test (
The degree of contrast spread did not affect the clinical improvement in our study. The average distance of contrast spread was 53.2
Although all clinical parameters except claudication distance showed greater improvements in the SD group 2 weeks after inter-laminar epidural injection, this superiority was absent at 6 and 12 weeks. Because the role of inter-laminar epidural injection in spinal stenosis is short-term pain relief but its efficacy for long-term pain relief is unclear [24], the absence of a difference in clinical improvement between the SD and ID groups is plausible.
Limitations
Our study had several limitations. First, because significant dilution of the contrast (1:10) was used for contrast dispersion, some medications might have reached the stenotic level and been undetected in the ID group, resulting in NRS improvement, which might have decreased the possibility of detecting the difference.
Conclusion
We demonstrated that coverage of the stenotic area by contrast in inter-laminar epidural injection was important for acute pain reduction. Our results also revealed that contrast spread had a negative tendency of ‘more effective’ in pain reduction if the coverage of the stenotic area was not considered. To increase the success rate of inter-laminar epidural injection in lumbar spinal stenosis, the drugs must cover more than a moderate degree of the stenotic area, which can be achieved through optimal needle position or use of an epidural catheter.
Footnotes
Acknowledgments
This work was supported by the grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI16C3229) and ICT R&D program of MSIP/IIPT [Grant No. B0101-16-1081].
Conflict of interest
None to report.