
Abstract
BACKGROUND AND OBJECTIVE:
Nowadays, pulsed radiofrequency (PRF) is being used to control several types of musculoskeletal pain. Herein, we report a successful application of ultrasound (US)-guided PRF for a patient with refractory sciatic neuropathic pain.
CASE REPORT:
We applied US-guided PRF to a 50-year-old man, suffering from refractory neuropathic pain on the left foot following sciatic neuropathy for a period of approximately 6 months. We performed PRF on the level of piriformis muscle because the lesion of the sciatic nerve was presented digitally from the level of piriformis muscle on the magnetic resonance images. Under US guidance, the catheter needle was placed close to the left sciatic nerve, and dysesthesia and tingling sensation were reported to be less than 0.2 V. The PRF treatment was administered at 5 Hz and 5 ms pulsed width for 360 seconds at 45 V. After PRF on the left sciatic nerve, pain intensity – based on a numeric rating scale – decreased from 8 to 2. The reduction of pain was sustained for at least 6 months after the PRF procedure.
CONCLUSION:
We concluded that the PRF treatment is a very useful treatment technique for patients with refractory sciatic neuropathy.
Introduction
Peripheral neuropathic pain arises from damage or pathologic changes in the peripheral somatosensory nervous system. This neuropathic pain is often unresponsive to pharmacological or non-pharmacological treatments [1], which interferes with activities of daily living and reduces the quality of life [2]. Various medications or techniques have been applied for the management of refractory neuropathic pain, but complete pain control has rarely been achieved [3]. Therefore, the treatment of refractory neuropathic pain still remains to be a major clinical challenge.
Pulsed radiofrequency (PRF) – a technique first described by Sluijter in 1997 [4] – is known to be safe and effective in alleviating pain, which works by delivering an electrical field and heat bursts to targeted nerves or tissues without damaging these structures [5, 6, 7]. Conventional radiofrequency (RF) thermocoagulation exposes target nerves or tissues to a continuous electrical stimulation and ablates the structures by increasing the temperature around the RF needle tip [8]. In contrast to RF, PRF applies a brief electrical stimulation followed by a long resting phase. As such, PRF does not produce sufficient heat that allows structural damage [9]. The proposed mechanism of PRF is that the electrical field produced by PRF can alter pain signals [10]. To date, PRF has successfully been reported to modulate several types of pain, including neuralgia, joint pain, and myofascial pain [11, 12, 13]. Regarding the application to peripheral nerves, PRF procedures to various peripheral nerves, such as suprascapular, occipital, median, and pudendal nerves, were reported to effectively control pain [14, 15, 16, 17]. However, to the best of our knowledge, the use of PRF to manage neuropathic pain caused by sciatic nerve injury has not yet been reported in the literature.
In this study, we describe successful application of ultrasound (US)-guided PRF for a patient with refractory sciatic neuropathic pain.
Case report
A 50-year-old man presented to the emergency department of our university hospital with stupor mentality from acute drug intoxication (ADI) (each 30 tablets of Quetiapine fumarate 25 mg, Diazepam 2 mg, Zolpidem Tartrate 10 mg, Flunitrazepam 1 mg, and Flurazepam 15 mg). He had received medical management for impulse control disorder and personality issues at a local psychological hospital for the past 10 years. After the management of ADI, the patient’s mentality became alert 2 days after the onset of ADI. Four months after the onset of ADI, he visited the rehabilitation department of the same university hospital due to tingling sensation and piercing pain on his entire left foot. The patient provided informed consent for participation in the study. The study was approved by the local Institutional Review Board of our hospital. He had suffered pain on his left foot since the alert mental status 2 days after ADI onset. The numeric rating scale (NRS) score was 8 out of 10, which was not controlled by various medications, such as acetaminophen/tramadol hydrochloride 1950/225 mg, meloxicam 15 mg, and pregabalin 450 mg. Moreover, the severity of pain showed nearly no significant interval change during the 4-month period after pain onset. On physical examination, he showed motor weakness on his left lower extremity, which was manifested from when he became alert after ADI. He was unable to actively dorsiflex and plantarflex his left ankle and toes (Medical Research Council [MRC] [18]: 0/5), and showed diminished motor strength (MRC: 3/5) in the left knee flexor. Sensation to touch was markedly reduced on the dorsal and plantar surfaces of his left foot. Left ankle jerk was reduced. To diagnose the cause of symptoms, we performed an electrophysiological study, including nerve conduction study and electromyogram at 4 months after the pain onset. The electrophysiological findings indicated injury to the left sciatic nerve between the lumbosacral plexus and the upper thigh, with decreased recruitment of the biceps femoris and no recruitment of tibialis anterior, peroneus longus, and gastrocneminus (medial head) muscles. Positive sharp wave (3
Axial T1-, T2-, and T2-weighted fat suppression magnetic resonance (MR) images of piriformis muscle (A) and lesser trochanter (B) levels. On the piriformis muscle level, the left sciatic nerve showed an increased signal intensity on axial T2-weighted fat suppression MR image (blue arrow). On lessor trochanter level, enlargement of left sciatic nerve was presented on T1- and T2-weighted MR images (green arrows).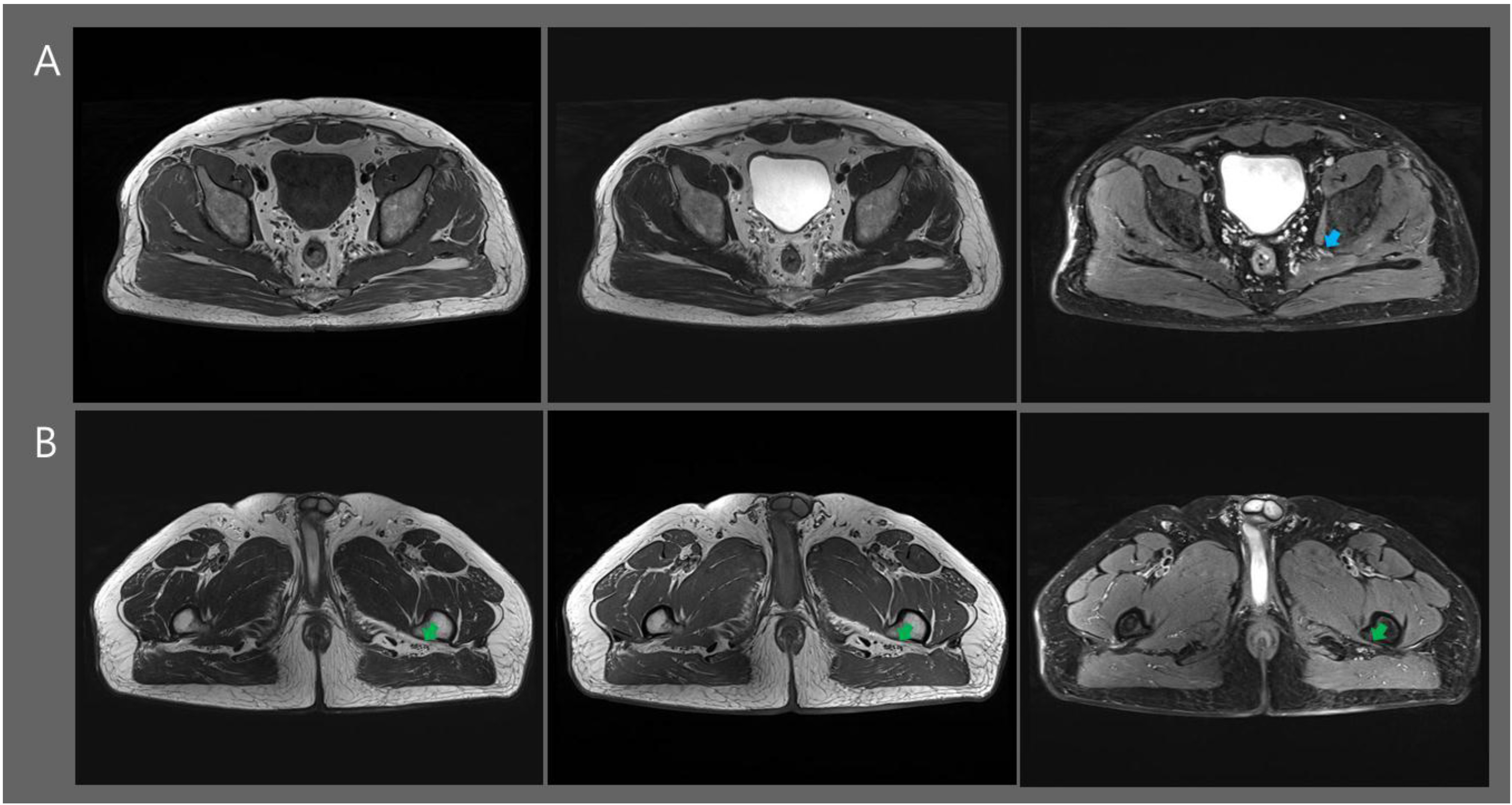
Prior to the PRF procedure, 4.5 months after pain onset, we performed a US-guided sciatic nerve block at the level of piriformis muscle with 5 mg dexamethasone mixed with 3 mL of 0.5% bupivacaine, 3 mL of 2% lidocaine, and 3 mL normal saline. The effect of sciatic nerve block was sustained for a period 2 weeks; the NRS score was sustained to be 5 during a 2-week period after the block procedure. We repeated a US-guided sciatic nerve block with the same method and medicine dosage. The NRS score was reduced from 8 to 5. However, the effect of this block was shorter than the previous block, which was sustained only for 1 week. Six months after pain onset, we performed the PRF procedure to manage his foot pain. The aseptic technique was applied in performing the PRF procedure. The patient was in a prone position, and the left thigh was scanned with axial images, from the hip to the knee using 6-MHz curved probe, equipped with LOGIQ P6 (General Electric, Republic of Korea). After identifying the left sciatic nerve at the piriformis level, the catheter needle (22-gauge active curved-tip electrode) was inserted, and the sensory simulation test was carried out using an RF generator (RFG4, Cosman Medical Inc., MA, USA) (Fig. 2). Under US guidance, the catheter needle was placed close to the left sciatic nerve, and the patient reported dysesthesia and tingling sensation with less than 0.2 V. PRF treatment was administered at 5 Hz and 5 ms pulsed width for 360 seconds at 45 V under the constraint that the electrode tip temperature did not exceed 42
(A) Transverse ultrasound image of the left sciatic nerve (arrows). GM: gluteus maximus, GT: greater trochanter, Pi: piriformis, blue arrowheads: catheter needle, red arrowhead: catheter needle tip.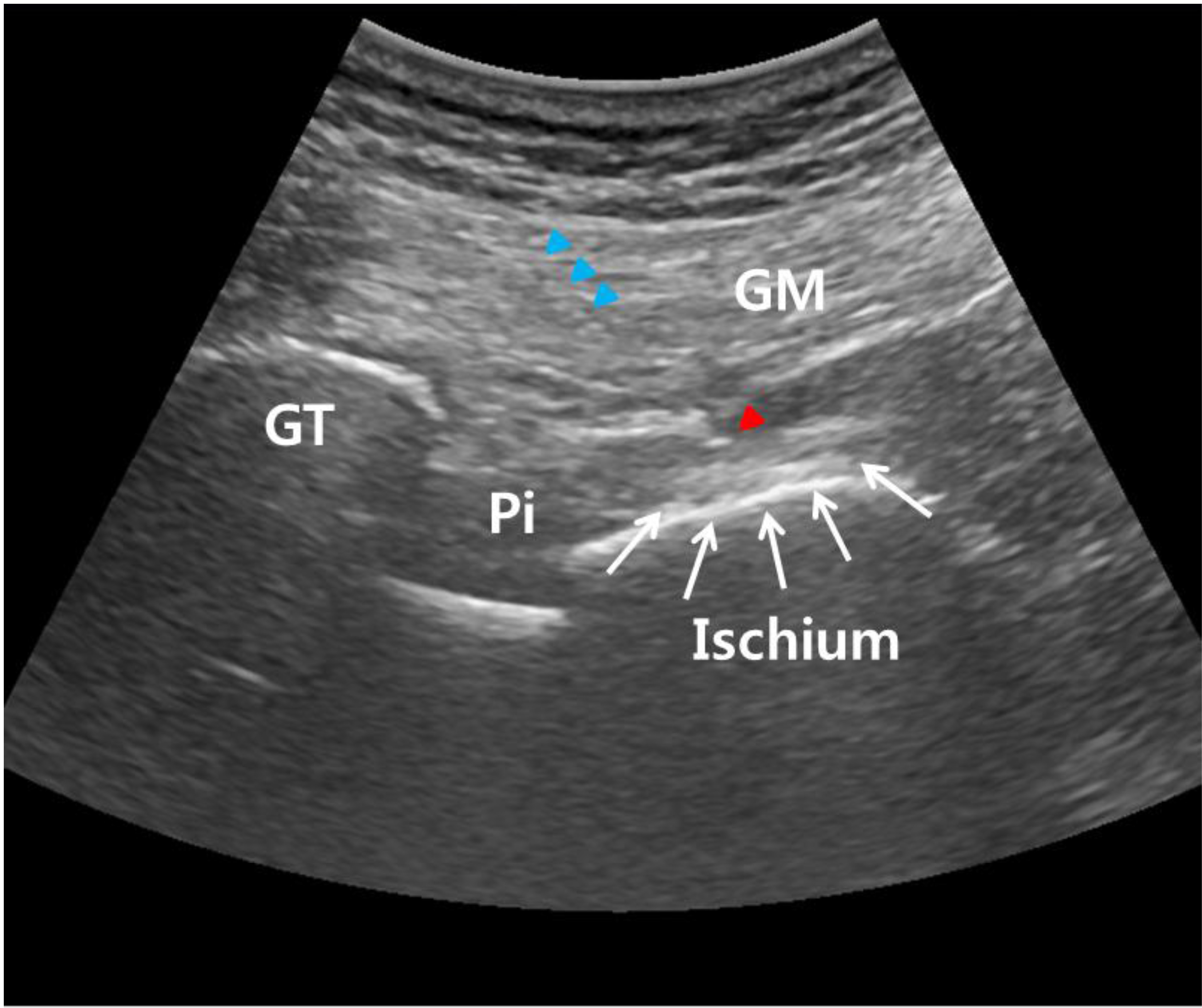
In the current study, we described the effective use of PRF for managing the refractory pain related to sciatic neuropathy. By physical examination, electrophysiological, and MRI findings, we diagnosed left sciatic neuropathy, which was thought to be injured around the piriformis muscle level. Moreover, the patient was in a state of stupor at the time of sciatic neuropathy; therefore, we assumed that his neural injury may have been caused by compression or stretch injury.
To control for neuropathic pain caused by sciatic neuropathy, prior to performing PRF, we performed sciatic nerve blocks with dexamethasone and local anesthetics (lidocaine and bupivacaine) twice. An injection of dexamethasone and local anesthetics has been known to block the transmission in nociceptive C-fiber, reduce ectopic discharge, and facilitate the recovery of nerve conduction following nerve injury [19]. However, in our patient, the pain control effect of the sciatic nerve block was mild to moderate, which was sustained for 1–2 weeks after the block. Therefore, we performed the PRF technique to manage his pain. After the application of PRF on the sciatic nerve, refractory neuropathic pain was reduced to the level that of bearable pain (NRS: 2), which lasted for at least 6 months.
The mechanisms behind PRF in reducing pain remain unclear. However, Higuchi et al. [20] showed that PRF to the dorsal root ganglion (DRG) increases the number of c-fos in laminae I and II of the dorsal horn. Increased expression of c-fos causes sustained activation of some pain-inhibition mechanisms. Cho et al. [21] found downregulated microglia activity in the spinal dorsal horn of a rat model of lumbar disc herniation after PRF on the DRG. Because microglia contribute to the development of chronic neuropathic pain by releasing several cytokines and chemokines that mediate pain signaling, a downregulation of microglia would possibly prevent the progression to chronic neuropathic pain. Regarding the PRF application to sciatic nerve, Hagiwara et al. [22] reported that an electromagnetic field of PRF applied to rat sciatic nerves enhances the noradrenergic and serotonergic descending pain inhibitory pathways and the inhibition of excitatory C-fibers. Lee et al. [23] reported a decreased tumor necrosis factor-
Several studies were reported showing the safety and effectiveness of the PRF technique for controlling various types of musculoskeletal pain [11, 12, 13]. As for the application to the sciatic nerve, to the best of our knowledge, two studies were reported to date. In 2008, Wilkes et al. [25] reported a long-term effect of PRF (2 Hz, pulse width of 20 ms, 2 cycles of 120 seconds at 42
Conclusion
In conclusion, we report a patient who showed good therapeutic response of US-guided PRF on the sciatic nerve for managing refractory neuropathic pain after sciatic neuropathy. Although further studies involving a greater number of patients with sciatic neuropathic pain are necessary, we think our study shows that PRF can be an effective treatment option for controlling refractory sciatic neuropathy.
Conflict of interest
None to report.