
Abstract
BACKGROUND:
LBP is one of the most common symptoms with high prevalence throughout the world. Conflicting conclusions exist in RCTs on cupping for LBP.
OBJECTIVE:
To assess the effects and safety of cupping for the patients with LBP.
METHODS:
Pubmed, Cochrane Library databases, and Embase database were electronically researched. RCTs reporting the cupping for the patients with LBP were included. The meta-analysis was conducted using Review Manager software (version 5.3, Nordic Cochrane Centre). The primary outcome was VAS scores. The secondary outcomes included ODI scores, MPPI scores and complications.
RESULTS:
Six RCTs were included in this synthesized analysis. The results showed that cupping therapy was superior to the control management with respect to VAS scores (SMD:
CONCLUSIONS:
Cupping therapy can significantly decrease the VAS scores and ODI scores for patients with LBP compared to the control management. High heterogeneity and risk of bias existing in studies limit the authenticity of the findings.
Introduction
Low back pain (LBP) is one of the most common symptoms affecting innumerable individuals throughout the world. A global review of the prevalence of LBP in the general adult population has shown its point prevalence to be approximately 12%, with a one-month prevalence of 23%, a one-year prevalence of 38%, and a lifetime prevalence of approximately 40% [1]. It is a generic term of kinds of back pains characterized by no identified histopathological changes and cannot clear its etiology from objective determinations. The symptoms of LBP could be acute/chronic lumbosacral pain accompanied with/without pain or numbness of legs. Female or older workers were at increased risk of experiencing LBP [2], students who sat with the spine positioned wrongly, or stood incorrectly, were more likely to present with LBP [3]. The risk factors of LBP included postmenopausal female, work-family imbalance, exposure to a hostile work environment, job insecurity, long work hours, certain occupation groups, unemployment, and sleep disturbances [4, 5, 6].
The current therapeutics of LBP consist of absolute bed rest at acute phase, analgesic or anti-inflammatory medications, physiotherapy, traction, alternative treatments and education regarding the prevention of LBP.
Cupping therapy is a common therapy in Traditional Chinese Medicine (TCM) field with a long history, which could be used to reduce the local chronic pain symptoms. Nowadays, more and more patients have shown an interest in using cupping therapy for the treatment of LBP due to their belief that it is more effective and safe than the current therapeutics. Although the cupping is safe ussually, it would leave local site skin pigmentation which would gradually vanish in a few days, and has been reported a complication of anaemia after excessive cupping therapy by an unqualified therapist in Korea in a case report [7].
There are many types of cupping including dry cupping, wet cupping, cupping with retention, moving cupping, shaking cupping, quick cupping and balance cupping. All of these types of cupping were frequently used in China, while dry cupping and wet cupping were widely used in Asian and Middle Eastern countries [8]. Dry cupping is using the negative pressure conditions of the cup to suck the skin into the cup without drawing blood. Wet cupping should prick the skin, so that blood of local site could be drawn into the cup. Cupping with retention is that cup is retained for a period of time on the skin after the dry cupping process completed. Moving cupping is characterized by moving on the skin by pre-daubing lubricating oil on the skin. Shaking cupping is a kind of cupping that after the cup sucked on the skin, the manipulator hold the body of cup to shake it. Quick cupping is characterized by quickly removing the cup once it sucks on the skin, which is on the contrary to cupping with retention. Balance cupping is a combination of cupping with retention, shaking cupping, quick cupping and moving cupping with established procedures.
Although cupping therapy has been used for LBP for a long time, it has been limited to assess its efficacy due to lack of high-quality, well-designed randomized controlled trials (RCTs). Nowadays, more and more RCTs concerning cupping therapy for LBP written in Chinese or English have been published. At present, there were 5 studies published in English were searched containing a description of systematic review on this topic. In 2011, a systematic review conducted by Kim of South Korea drew a conclusion that the current RCTs were few and showed low methodological quality [9]. In 2013 and 2015, there were two systematic reviews drew a conclusion that cupping therapy is promising for pain [10, 12]. In 2014, a systematic review of traditional medicine in east asian countries weakly recommended cupping therapy for both sub-acute and chronic LBP [11]. In 2015, a review about all aspects of TCM for neck pain (NP) and LBP indicated that cupping could be efficacious in pain and disability for chronic NP or chronic LBP in the immediate term [13]. Since there is no consensus on cupping therapy for LBP, we searched the existing RCTs published in English or Chinese language to make a synthesized analysis to test its effectiveness in patients with LBP.
Materials and methods
We conducted this meta-analysis according to the PRISMA (Preferred reporting items for systematic reviews and meta-analyses) statement [14].
Literature search strategy
The strategy of literature search was according to the guidance of the Cochrane Handbook. We electronically searched the Pubmed database, Cochrane Library databases, and Embase database from their inception up to 31st August 2016 to identify studies meeting the inclusion criteria. RCTs concerning cupping therapy for subacute or chronic LBP were searched in electronic databases by two authors independently. The search terms were as follows: ((Low back pain*) OR (back pain*, low) OR (pain*, low back) OR (lumbago) OR (lower back pain*) OR (back pain*, lower) OR (pain*, lower back) OR (low back ache*) OR (ache*, low back) OR (back ache*, low) OR (low backache*) OR (backache*, low) OR (recurrent low back pain*) OR (low back pain*, postural) OR (postural low back pain*) OR (low back pain*, mechanical) OR (mechanical low back pain*) OR (low back pain*, posterior compartment) OR (lumbar sprain) OR (lumbar myofasciitis) OR (lumbosacral pain*)) AND (cupping OR (cupping therapy) OR (dry cupping) OR (wet cupping) OR (cupping with retention) OR (moving cupping) OR (shaking cupping) OR (quick cupping) OR (balance cupping)). To ensure retrieval comprehensive, we manually searched the reference lists of all retrieved studies and published systematic reviews/meta-analysis, and included all identified relevant articles.
Eligibility criteria
Inclusion criteria
(1) Randomized controlled trial. (2) Participants enrolled in trials were diagnosed as nonspecific subacute or chronic LBP. (3) Intervention in experimental group was a kind of cupping therapy, which could be dry cupping, wet cupping, cupping with retention, moving cupping, shaking cupping, quick cupping or balance cupping. (4) Intervention in control group was medication or usual care. (5) The interested outcomes included one of the VAS (visual analogue scale) scores, ODI (Oswesty pain disability index) scores and MPPI (McGill present pain index) scores. (6) Language of included trials were published in English or Chinese.
Exclusion criteria
(1) Comorbid factors such as fracture, dislocation, tumor of lumbar spine which directly deduce the LBP symptom in participants. (2) non-RCT. (3) Sample size less than 15. (4) Studies without available data for statistics were excluded.
Study identification
Firstly, all titles of searched articles were viewed by two investigators independently. At this step, articles obviously unrelated to the topic were removed. Secondly, full articles were reviewed to remove the non-RCTs and articles without comparison group. Thirdly articles were removed due to the lack of interested outcome. The third investigator was involved in the study when there existed divergence on eligibility of enrolled studies.
Methodological quality assessment
The methodological scores of eligible studies were assessed by using Jadad scale [15]. Two independent investigators performed the methodological evaluation. The third investigator was consulted to resolve it once divergence occurs.
Flow diagram of study selection.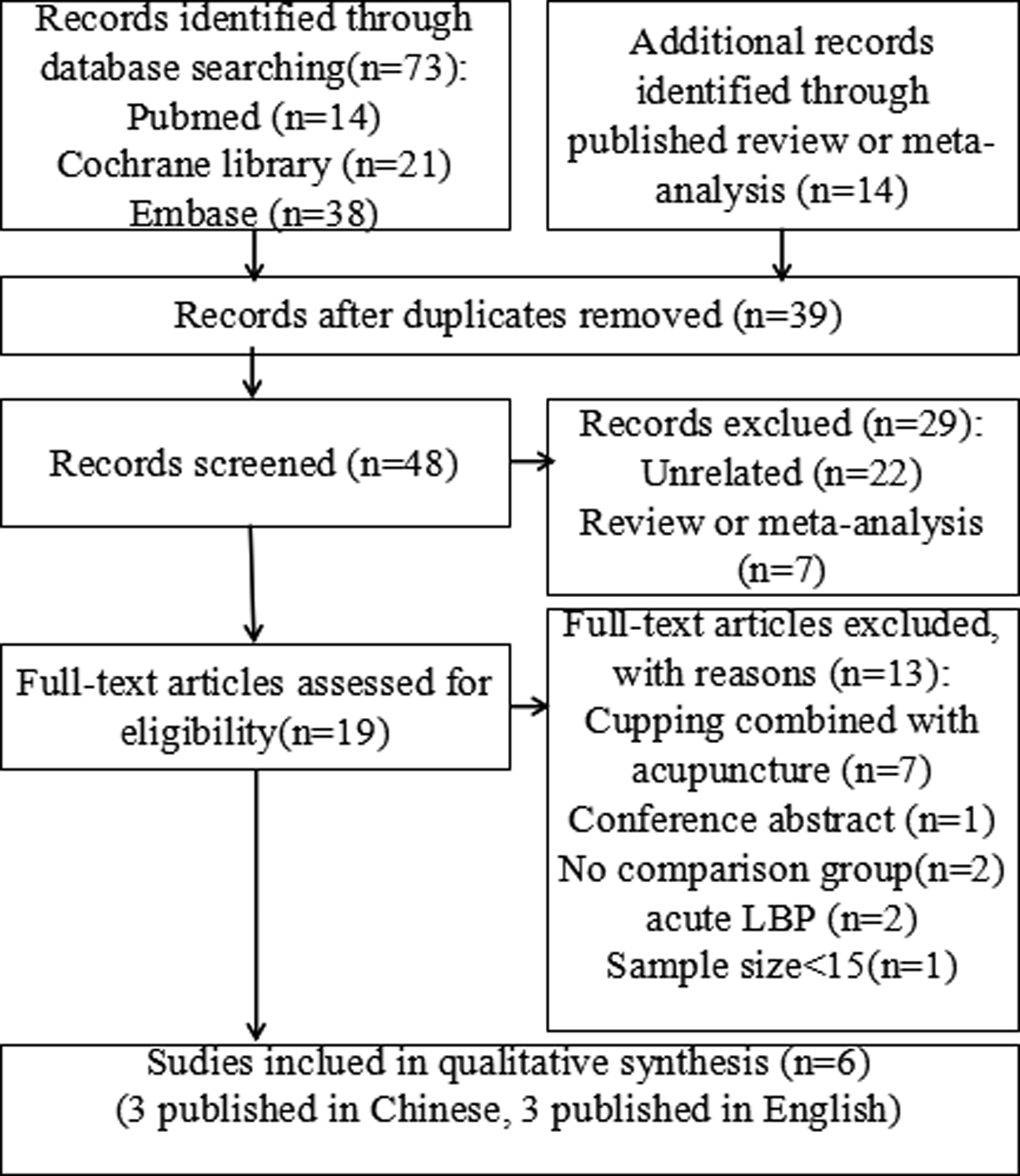
The primary outcome was VAS scores. The Secondary outcomes included ODI scores, MPPI scores and complications.
Data extraction
The following data from each study were extracted independently by two authors: first author’s family name, year of publication, diagnosis, interventions, sample size, mean age, interested outcomes, follow-up times, lost follow or withdraw, adverse events, the baseline of interested outcome before interventions, the interested outcomes at the chosen time point and end of follow-up period. Any disagreements were resolved by consensus.
Statistical analysis
Data analyses were conducted by using the Review Manager statistical software (version 5.3, Nordic Cochrane Centre). Standard Mean Difference (SMD) with 95% confidence intervals (CIs) was selected to describe the mean differences between cupping group and control group. A
The demographic characteristics of the patients of the included studies (cupping vs. control)
The demographic characteristics of the patients of the included studies (cupping vs. control)
Abbreviations: NLBP, nonspecific low back pain; PLBP, postpartum low back pain; VAS, visual analogue scale; ODI, Oswesty pain disability index; MPPI, McGill present pain index; NR, not report.
Comparisons of interested outcomes (cupping vs. control)
Abbreviations: VAS, visual analogue scale; ODI, Oswesty pain disability index; MPPI, McGill present pain index; NA, not available.
Jadad scores of the enrolled studies
Abbreviations: RCT, randomized controlled trial.
Literature search and study selection
A total of 87 studies were searched from electronic and manual searching. Specifically, 14 from Pubmed, 21 from Cochrane library, 38 from Embase, and 14 were manually searched from the reference lists of published systematic review or meta-analysis. After duplicated, 39 studies were removed and 48 studies remained for screening. Then 29 studies were excluded for obviously unrelated to the research topic after review the titles and abstracts, 19 studies remained for next full-text review. After full-text articles assessed for eligibility, 13 articles were excluded for reasons as follows: cupping combined with acupuncture (
Study characteristics
Six RCTs were included in this meta-analysis, 3 RCTs [18, 19, 20] published in Chinese were from China, 2 RCTs [21, 22] published in English were from Iran, 1 RCT [23] published in English was from Saudi Arabia. All the trials included were RCTs.
A total of 458 participants enrolled in this study, including 230 participants in cupping groups and 228 participants in control (medication or usual care) groups respectively. The participants in 4 RCTs [18, 19, 20, 21, 23]were diagnosed as nonspecific low back pain (NLBP), and participants in 1 RCT [22] were diagnosed as low back pain among postpartum women (Table 1).
As for the intervention aspect, there are many types of cupping therapy reported in cupping groups. Three RCTs [19, 20, 22] adopted dry cupping, 2 RCTs [21, 23] using wet cupping, and 1 RCTs [18] applied moving cupping. As for control groups, 3 RCTs [18, 19, 20] adopted oral medications (diclofenac sodium in 2 RCTs [19, 20] and dexibuprofen in 1 RCT [18]), and 3 RCTs [21, 22, 23] applied usual care. The treatment sessions were from 11 days to 3 weeks with different frequencies (Table 1).
All the included RCTs at least reported one of the interested outcomes. Four RCTs [18, 19, 20, 22] reported VAS score as their important indicator to evaluate the level of pain. Four RCTs [19, 20, 21, 23] adopted ODI score to evaluate the degree of limitation of daily life and activity ability. And 3 RCTs applied the McGill pain index to assess the present pain level. But among these 3 RCTs [21, 22, 23], there was 1 RCT [22] adopted the short-form McGill pain questionnaire which is quite different to the McGill present pain index. The data at baseline and each point of follow-up were abstracted in Table 2. There was no report of serious adverse event in the included RCTs.
Methodological quality assessment
As for the randomization aspect, all RCTs reported the method of random sequence generation, but only 3 RCTs [21, 22, 23] reported the appropriate randomization or allocation concealment process. Thus other 3 RCTs [18, 19, 20]existed a moderate degree of selection bias. Considering the specialization of the cupping process, all the RCTs did not use blinding of participants or personnel. So there exists high performance bias in all trials. Blinding of outcomes assessors was not applied in all these RCTs, so all the trials exist a high detection bias. Due to the relative short term of follow up, all the studies reported the situation of withdrawl and dropouts, and achieved high follow up rate. So there exists low risk of withdraw bias in all trials. The specific Jadad score of the enrolled studies were listed in Table 3.
Forest plot of VAS score.
Forest plot of ODI score.
Forest plot of MPPI score.
VAS scores
Four RCTs including 280 participants reported the follow-up end VAS scores. The results of pooled analysis showed that cupping therapy was superior to the control (medication or usual care) on decreasing VAS score (SMD:
ODI scores
Four RCTs [19, 20, 21, 23] adopted ODI score to evaluate the degree of limitation of daily life and activity ability. 1 RCT [23] reported the ODI scores in the form of median and range. So we estimated the mean and variance from the median, range, and the sample size according to the calculation method reported by Hozo et al. [24]. The sample of this trial was 40, so the mean was equal to the median, and the variance is equal to the quarter of range [24]. The results of meta-analysis involving 288 participants revealed that the cupping therapy showed significant advantages over the control (medication or usual care) on reducing the follow-up end ODI score (SMD:
MPPI scores
Three RCTs applied the McGill pain index to assess the present pain level. But among these 3 RCTs [21, 22, 23], there was 1 RCT [22] adopted the short-form McGill pain questionnaire which is quite different to the McGill present pain index. So only 2 RCTs [21, 23] were included in meta-analysis. Albedah’s study [23] reported MPPI scores in the form of median and range, we also used Hozo’s method [24] to calculate the data in the form of mean and variance. The results of meta-analysis found that there was no significant difference between two groups on MPPI scores (SMD:
Forest plot of sensitivity analysis of VAS score.
Forest plot of sensitivity analysis of ODI score.
Statistical tests of heterogeneity revealed that there were high heterogeneity with respect to all the interested outcomes. So we performed the sensitivity analysis to explore the source of high heterogeneity. We found that when we remove the trial of Akbarzadeh et al. [22], the heterogeneity of VAS score was turned to moderate (
Discussion
The main findings of this study are that cupping ther-apy can significantly decrease the VAS scores and ODI scores compared to the control management (usual care/medication) for patients with LBP. And there is no significant difference between cupping therapy and the control management on MPPI scores for patients with LBP. However the results of VAS scores and ODI scores are unstable according to the results of sensitivity analysis.
The VAS scores is a scale with 10 numbers, and elucidated as follows: no pain (0), mild (1 to 3), moderate pain (4 to 6), severe pain (7 to 9), and the worst pain possible (10), and is frequently used in patients with chronic musculoskeletal pain [25]. In this study, we found cupping therapy was superior to the control management on decreasing VAS scores. That means cupping therapy shows advantages on alleviating pain over the control management (medication or usual care) for patients with LBP. In the included RCTs, there were 2 RCTs’s results showed a negative results as regards to VAS scores between dry cupping and diclofenac sodium for LBP [19, 20]. And there were 2 RCTs’s results reported cupping therapy can significantly decrease the VAS scores compared to the control management [18, 22]. The trial of Hong et al. [18] reported moving cupping was superior to dexibuprofen on decreasing the VAS scores. The moving cupping therapy method might be the key factor contributing to the positive result. The trial of Akbarzadeh et al. [22] reported dry cupping was superior to usual care on decreasing the VAS scores.
The ODI scores is an important tool to measure a patient’s permanent functional disability in the management of spinal disorders [26]. The test is considered the “gold standard” of low back functional outcome tools [27]. In our study, the result revealed that cupping therapy showed more advantages over the control management on decreasing ODI scores. It is suggested that in the aspect of improving the disability condition induced by LBP, cupping therapy is better than the control management. In the included RCTs, there were 2 RCTs’s results showed a negative results as regards to ODI scores between dry cupping and diclofenac sodium for LBP [19, 20]. And there were 2 RCTs’s results reported wet cupping therapy can significantly decrease the ODI scores compared to the usual care [21, 23]. The advantage of dry cupping compared to diclofenac sodium on decreasing ODI scores didn’t show a significant difference.
The MPPI scores is a standard and well-used index of current pain. Patients rate their current pain on a 6-point scale from “no pain” to “excruciating” [28]. Although there exists significant advantages of cupping therapy on down-regulating the MPPI scores compared to the usual care in both 2 included RCTs, the result of meta-analysis showed no statistical significance. The Hozo’s calculation method [24] and the high heterogeneity between 2 RCTs might contribute to this result.
There were high heterogeneity in the results of all interested outcomes. Although, sensitivity analysis can find the main source of the heterogeneity, there still exists statistical significant difference in heterogeneity. We noted possible causes as follows: firstly, although all the included participants were patients with LBP, the patients enrolled in the study of Akbarzadeh et al. [22] were postpartum women with nonspecific LBP. Generally postpartum women have higher prevalence and level of pain compared to the normal [29, 30]. Secondly, as for experimental interventions, there were many types of cupping therapy, and the treatment session and frequency were not the same in trials (see Table 1). Thirdly, as for the control interventions, there also existed different types of medication and usual care (see Table 1). Fourthly, the drawback of design of RCTs (such as without blinding of participants or personnel due to the cupping therapy was well-known by participants and particularity of the cupping for the personnel) also contributed to the high heterogeneity. Fifthly, the calculation method used on the data of MPPI scores and ODI score in Albedah’s study might create heterogeneity.
There existed different degrees of risk of bias in trials. According to the situation of methodological quality assessment, moderate degree of selection bias in some trials, high performance bias, high detection bias, and low risk of withdraw bias in all trials were found. All trials did not involve independent examiners, which may have contributed some observer bias, a distortion, conscious or unconscious, in the perception or reporting of measurements [31]. And at the process of calculation on the data of MPPI scores and ODI score in Albedah’s study, calculation bias might exist.
The findings need to be further confirmed by subgroup analysis based on different types of cupping and control management, and meta-regression to find the source of high heterogeneity based on more well-designed and high-quality RCTs.
There also exist some limitations in this meta-analysis. Firstly, many types of cupping therapy and different control managements were included in cupping groups and control groups respectively, and it is difficult to conduct subgroup analysis or Meta regression due to the lack of enough trials. Secondly, the frequency of cupping, duration of each session, location of acupoints, experience of manipulators in each trial were different. These factors might strongly influence the clinical effects of cupping. Thirdly, the included Chinese RCTs [18, 19, 20] showed low-scoring of Jadad scores, and the inlcuded English RCTs [21, 22, 23] showed fair-scoring of Jadad scores. The qualities of original trials may potentially impact results of each trial and meta-analysis. Additionally, we did not test the publication bias due to the limitation of number of RCTs.
Conclusion
Cupping therapy is a promisingly effective and safe therapy method for subacute or chronic low back pain. Cupping therapy can significantly decrease the VAS scores and ODI scores compared to the control management (usual care/medication). High heterogeneity and risk of bias existing in trials limited the authenticity of the findings.
Conflict of interest
The authors declare that they have no conflict of interest.
Footnotes
Acknowledgments
This work was supported by Guangdong province natural science foundation of China (Grant No. 2015A 030313724), and Production, study and research pro- ject of Guangdong province department of science of China (Grant No. 2013B090600144).