
Abstract
BACKGROUND AND OBJECTIVES:
Normal dorsiflexion (DF) required for normal gait is achieved through balance of the tibialis anterior (TA) and extensor hallucis longus (EHL). Imbalance may induce ankle and foot deformities and exacerbate pathology. EHL dominance is associated with progressive TA weakness, attributable to muscle non-use. When the EHL dominantly dorsiflexes the ankle, the big toe extends at the metatarsophalangeal joint (MTPJ) and pure ankle DF is absent. The effects of active MTPJ flexion on TA and EHL muscles, TA/EHL ratio, and the force applied during active DF in EHL-dominant (EHL-D) and EHL-non-dominant (EHL-ND) subjects were compared.
METHODS:
The 38 subjects were divided into EHL-D and EHL-ND groups. All subjects performed active ankle DF with and without active MTPJ flexion. Surface electromyographic data, ankle active range of motion, and DF force were measured. Two-way mixed analysis of variance was used to evaluate differences in dependent variables.
RESULTS:
Compared to the EHL-ND group, the EHL-D group exhibited less TA activity, more EHL activity, and a reduced TA/EHL activity ratio. Active application of MTPJ flexion during DF significantly reduced muscle imbalance, whereas EHL activity decreased and the TA/EHL activity ratio increased. The DF force decreased significantly with MTPJ flexion in both groups.
CONCLUSIONS:
Active MTPJ flexion can reduce EHL and/or increase TA activity and increase the TA/EHL activity ratio during active ankle DF in both EHL-D and EHL-ND subjects.
Introduction
The muscles involved in ankle dorsiflexion (DF) are the tibialis anterior (TA), extensor hallucis longus (EHL), extensor digitorum longus (EDL), and peroneus tertius (PT) [1, 2]. All of these enter the foot under the extensor retinaculum and are innervated by the deep peroneal nerve [3]. The main function of DF is to retain the foot in dorsiflexed position at heel strike, to allow toe clearance at the end of the swing, and to allow the tibia to move over the talus at the mid-stance phase of gait [4]. Additionally, maximum ankle DF with the knee in full extension follows just before heel-off in the gait cycle [5, 6]. The TA is the strongest ankle dorsiflexor at mid-stance. The EHL and EDL activate the foot and toes at heel-strike and engage in DF to allow toe clearance during the swing [7]. The PT is not active during the stance phase and acts primarily to support the lateral longitudinal arch and transfer the center of pressure of the foot to a medial position [8]. Thus, if the TA is weakened, a normal gait pattern cannot occur, and the tibia cannot move over the talus at mid-stance.
Among various relevant factors, an imbalance between the activities of the extrinsic toe extensors and the EHL is considered to be a cause of toe deformity. Prolonged extension of the metatarsophalangeal joint (MTPJ), flexion of the proximal interphalangeal (IP) joint in patients with hammer toes, and extension/abduction of the MTPJ in patients with hallux valgus (HV) may also contribute to muscle imbalance (i.e., shortening of the extrinsic toe extensors and lengthening of the intrinsic toe extensors) [9]. Such length adaptation (over a period of time) shifts the length-tension curve of the extrinsic toe extensors toward a shortened length range with increasing tension, particularly when the MTPJ is extended. Such distal-initiated DF (activated by the EHL/EDL) alters the range of motion (ROM) of the ankle [10]; the ankle remains in plantar flexion, triggering lengthening of the TA. The concept of synergistic dominance suggests that the TA will thus become weak, and the EHL/EDL ratio will decrease and become dominant. Thus, individuals with weak TAs rely on the EHL/EDL ratio to achieve the ankle DF required for activities of daily living. This increases the extent of EHL/EDL dominance associated with progressive TA weakness attributable to non-use of the muscle. When the EHL dominantly dorsiflexes the ankle, the big toe extends at the MTPJ; pure ankle DF is absent. Sahrmann [9] suggested that the extrinsic toe extensors could be effectively extended by directing a patient to flex the MTPJ during ankle DF and to maintain such flexion thereafter. Kisner and Colby [2] also recommended active MTPJ as useful exercises for the ankle and foot. Additionally, ankle DF is not concurrent with MTPJ flexion during standing and gait, and toe flexion strength induced by MTPJ flexion could decrease the risk of falls [11], as well as maintain balance, because the toe-plantar foot surface should contact the ground during standing [11].
However, no study has explored the effect of MTPJ flexion during ankle DF in EHL-dominant (EHL-D) subjects. Therefore, the aim of the present study was to compare TA and EHL activity, the TA/EHL activity ratio, the active range of motion (AROM), and the force during ankle DF with and without MTPJ flexion in individuals who were EHL-D or EHL-non-dominant (EHL-ND). Our research hypothesis was that the activities of the TA and EHL muscles, the TA/EHL activity ratio, the DF AROM, and the force applied during ankle DF with and without MTPJ flexion would differ between EHL-D and EHL-ND individuals.
Methods
Participants
A power analysis performed after completion of a pilot study with 5 subjects indicated that a formal study required at least 13 subjects to obtain a confidence level of 0.05, a power of 0.80, and an effect size of 0.29 (G*power software 3.1.2; Franz Faul, University of Kiel, Kiel, Germany). Thirty-eight subjects (age
Characteristics of participants (mean
SD)
Characteristics of participants (mean
Abbreviation: BMI; body mass index, DF; dorsiflexion.
Surface electromyography (EMG)
The activities of the TA and EHL were measured via surface EMG (TeleMyo DTS; Noraxon, Inc., Scottsdale, AZ, USA) fitted with a wireless telemetry system. Skin impedance was minimized by rubbing with an alcohol swab, shaving of hair, and debridement. Bipolar electrodes (Ag/AgCl) were placed 2 cm apart. To analyze TA activity, an investigator palpated the TA muscle while the subject dorsiflexed the foot. Bipolar electrodes were placed parallel and just lateral to the medial shaft of the tibia (the shin) at approximately 25–33% of the distance between the knee and ankle [14]. EHL electrodes were placed 3 finger-widths above the line between both ankle malleoli, just lateral to the crest of the tibia [15]. Noraxon MyoResearch version 1.06 software was used for EMG signal processing. The EMG signals were amplified, band-pass filtered (20–450 Hz, Lancosh FIR), and notch-filtered (60 Hz). Data were next recorded at 1,000 Hz and processed into root-mean-square values with a window of 50 ms. The maximum voluntary isometric contraction (MVIC) was employed to normalize the EMG data of each tested muscle. To collect MVIC data, we used positions employed for manual muscle testing [16]. For TA analysis, each subject assumed a long-sitting position on a table with the hip and knee of the test leg flexed to 90
Goniometry
Ankle DF AROM was determined using a universal goniometer with a 1
Active range of motion (AROM) of the ankle joint during ankle dorsiflexion (DF) in prone position (A). AROM during DF without metatarsophalangeal joint (MTPJ) flexion (B).
Ankle DF force was measured using a hand-held dynamometer (MT-100; Sakaimed, Tokyo, Japan) running a Noraxon software program (HHD-N). The manual indicates that the MT-100 has a range of 0–1,000 kilogram-force (kgf) and an accuracy of
Measurement of ankle dorsiflexion force with hand-held dynamometer synchronized with Noraxon.
Before all tests, each subject stretched the ankles, MTPJs, and IP joints to reduce possible inconvenience or pain during experimentation. Each subject underwent ankle DF AROM assessment, MVIC for EMG data collection, measurement of maximal ankle DF to allow muscle activities to be assessed, and DF force measurement, in that order. The muscle activities and forces generated during ankle DF were measured instantaneously via surface EMG and the HHD-N. The PI provided verbal instructions and ensured that the resistance applied was consistent. Another investigator (HJJ) read and recorded the EMG data and forces. The subjects were barefoot during all procedures.
Each variable was measured in the presence and absence (in random order) of MTPJ flexion. Learning effects and fatigue were minimized by having the subjects draw lots. Each subject rested for 3 min between measurements of MVIC and ankle DF forces, and also between assumption of different positions [18].
Ankle DF without MTPJ flexion (absence of MTPJ flexion)
To measure ankle DF AROM in the absence of MTPJ flexion, each subject was positioned prone with the test knee flexed to 90
Ankle DF with MTPJ flexion (presence of MTPJ flexion)
Ankle DF with MTPJ flexion was performed in the same position as described above (for the assessment of ankle DF without MTPJ flexion). Each subject actively flexed the MTPJ prior to ankle DF measurement. The verbal instruction was: “Curl your toes down first, and move your ankle as much as you can, without moving your hip or knee.” Each subject performed MTPJ flexion prior to ankle DF measurement to become familiar with flexion. Each subject was allowed to rest after stretching the ankles, MTPJs, and IP joints to reduce possible inconvenience or pain. Each subject reported that she/he felt comfortable performing active MTPJ flexion after familiarization.
Statistical analysis
The test-retest reliability of the surface EMG data was assessed by calculating ICCs (with CIs); we employed the following criteria:
Two-way mixed models of variance were used to analyze between-group interactions (EHL-D group vs. EHL-ND group) and within-group differences in MTPJ positions (with or without MTPJ flexion). The dependent variables were: the activities of the EHL and TA muscles; the TA/EHL activity ratio; the AROM; and the ankle DF force. The level of statistical significance was set at
Results
Test-retest reliabilities of surface EMG measurements
The test-retest reliabilities of the EMG data for the TA and EHL, with or without MTPJ flexion, were good: TA [ICC (95% CI)
Muscle activities and the muscle activity ratio
No significant interaction was evident in terms of TA muscle activity (F
Muscle activity of the tibialis anterior (TA) in extensor hallucis longus dominant (EHL-D) group and EHL non-dominant (EHL-ND) group, with and without metatarsophalangeal joint (MTPJ) flexion. 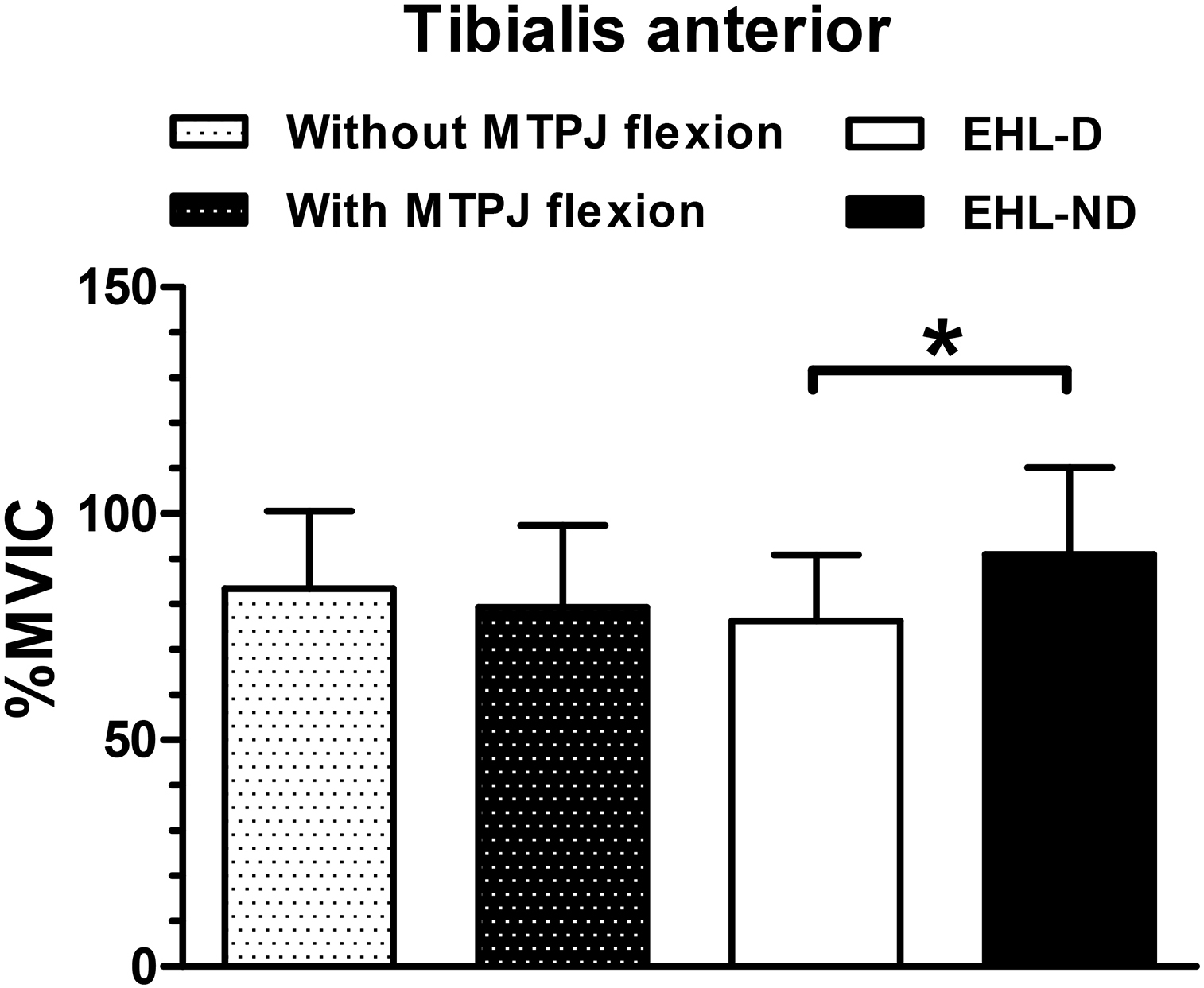
A significant interaction in terms of EHL muscle activity was evident (F
Muscle activity of the extensor hallucis longus (EHL) in extensor hallucis dominant (EHL-D) group and EHL non-dominant (EHL-ND) group, with and without metatarsophalangeal joint (MTPJ) flexion. 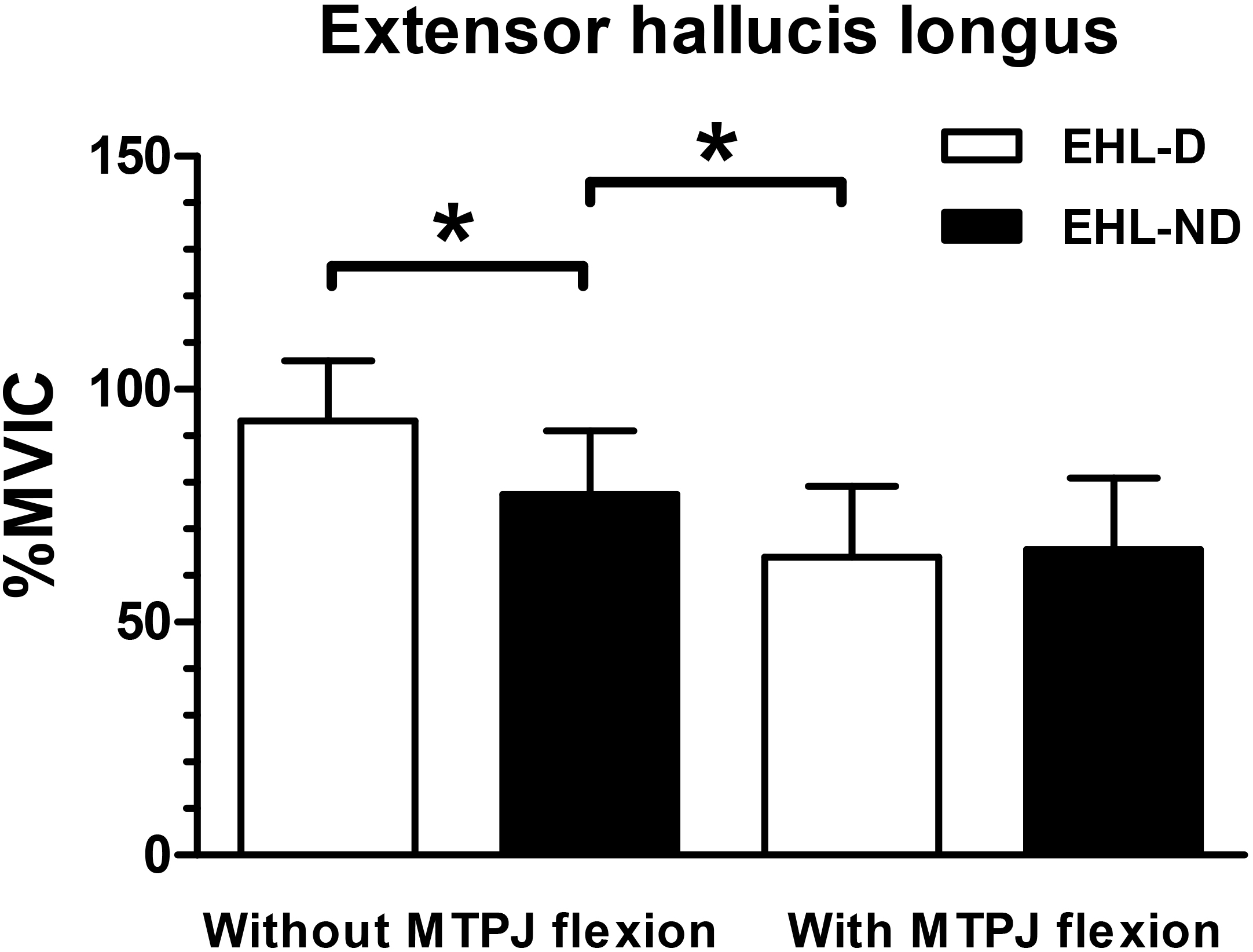
No significant interaction was evident in terms of the TA/EHL ratio (F
Ratio of tibialis anterior (TA) to extensor hallucis longus (EHL) activity in extensor hallucis dominant (EHL-D) group and EHL non-dominant (EHL-ND) group, with and without metatarsophalangeal joint (MTPJ) flexion. 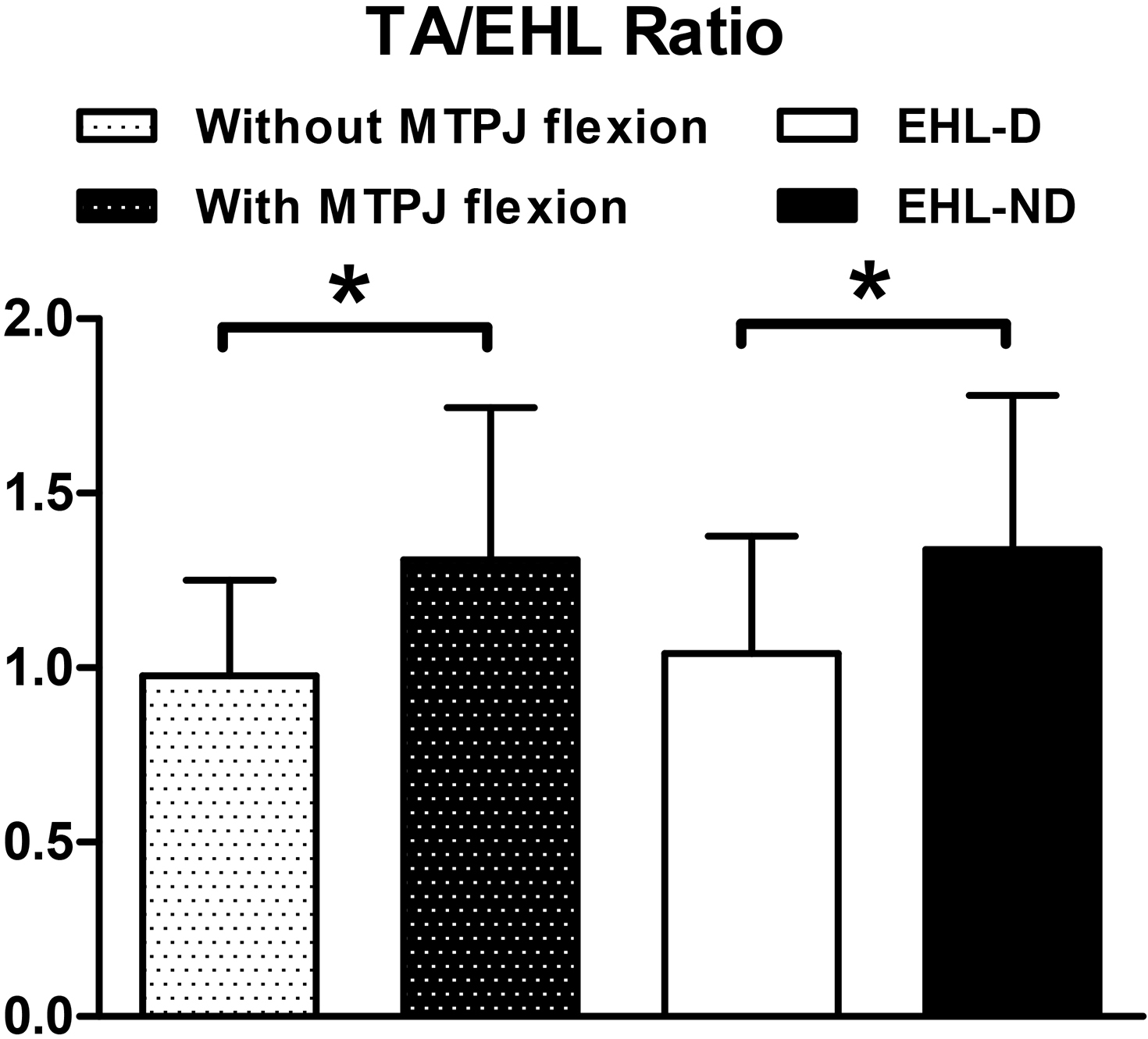
Dorsiflexion active range of motion (AROM) in extensor hallucis longus dominant (EHL-D) group and EHL non-dominant (EHL-ND) group, with and without metatarsophalangeal joint (MTPJ) flexion. No significant differences were found. 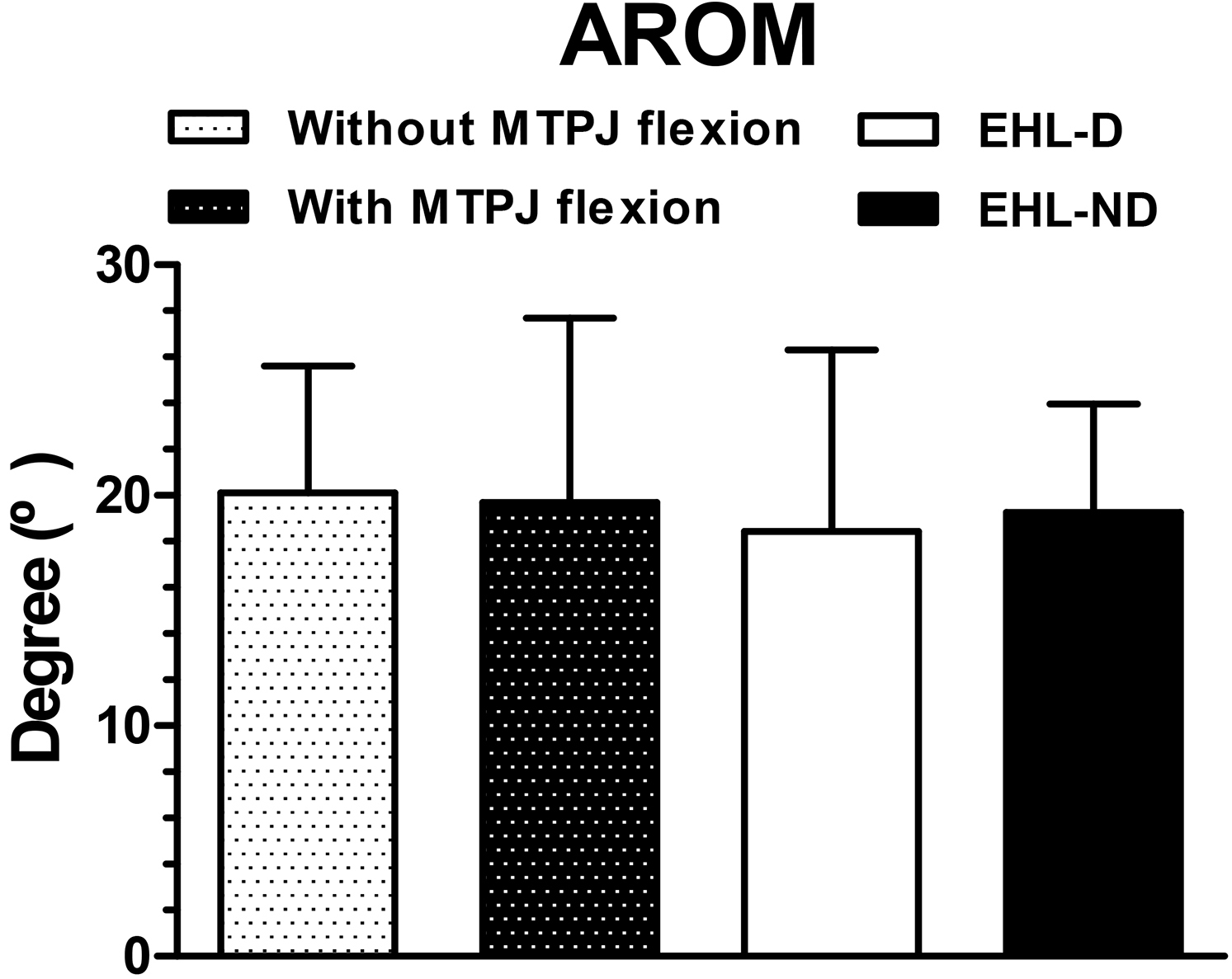
Dorsiflexion force in extensor hallucis longus dominant (EHL-D) group and EHL non-dominant (EHL-ND) group, with and without metatarsophalangeal joint (MTPJ) flexion. 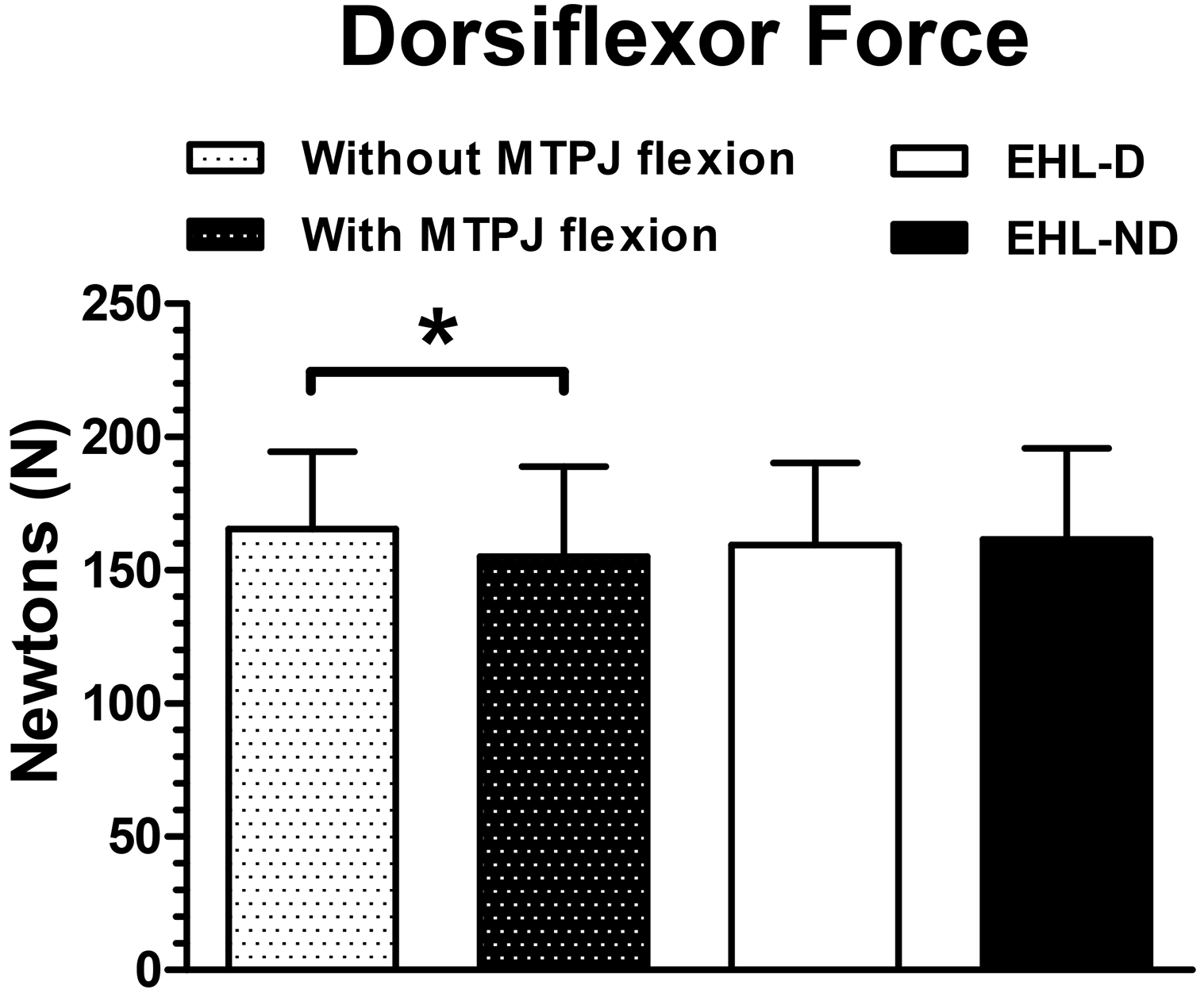
No significant interaction or main effect of either MTPJ position or group was evident in terms of DF AROM (F
Discussion
We studied the effect of MTPJ flexion on TA and EHL muscle activities, the TA/EHL activity ratio, and ankle DF force in EHL-D and EHL-ND subjects. To the best of our knowledge, this is the first study to measure TA and EHL muscle imbalances in EHL-D and EHL-ND subjects, and to explore the interventional effects of MTPJ flexion.
Our results showed that the EHL-D group had significantly less TA activity compared with the EHL-ND group. This finding supports the research hypothesis. The concept of synergistic dominance explains the increase in EHL dominance associated with progressive TA weakness attributable to non-use of the muscle. However, TA muscle activity was not significantly different with or without MTPJ flexion in both groups. This finding did not support the research hypothesis. Previous research reported that TA activity was significantly increased with use of a soft toe spreader compared to the activity during walking without a toe spreader. Thus, increases in weight-bearing loading or stance time might facilitate TA activity as extrinsic support (mechanical stability) [26]. In this study, MTPJ flexion did not increase stance time during maximal ankle DF, even in a fixed position. Thus, MTPJ flexion did not increase TA activity in EHL-D and EHL-ND subjects, although the results showed that TA activity decreases in EHL dominance.
In the absence of MTPJ flexion, the EHL-D group showed significantly greater EHL activity than the EHL-ND group. In the EHL-D group, the EHL activity decreased significantly with MTPJ flexion compared to the activity in the absence of flexion. The TA/EHL ratio was significantly lower in the EHL-D group than in the EHL-ND group. Moreover, this ratio increased significantly with MTPJ flexion compared to the ration in the absence of flexion. These findings support the research hypothesis. Active MTPJ flexion during DF significantly reduced muscular imbalance; EHL activity decreased and the TA/EHL activity ratio increased. The mechanism behind this change is believed to be reciprocal inhibition. MTPJ flexion improved muscle balance via the mechanism of “reciprocal inhibition”. With contraction of an agonist muscle (flexor hallucis longus with MTPJ flexion), inhibition reduces the activation of an antagonist muscle (EHL) [2]. Reciprocal inhibition is attributable to excitation of inhibitory interneurons by afferent stimuli from agonist muscle spindles, which in turn inhibit alpha motor neurons of the antagonist muscle [27, 28]. Additionally, with maintenance of MTPJ flexion, the plantar fascia is not maximally stretched, and the risk of injury is thus reduced. Another explanation is that synergist muscles work together and affect each other during movement [29, 30]. Thus, TA activity might be increased when EHL was decreased to achieve the same DF AROM. We confirmed that DF AROM did not affect either the MTPJ position or group. Finally, the observed reduction in EHL activity with active MTPJ flexion during DF showed that EHL activity can be reduced by actively flexing the MTPJ, which elongates a short-adapted EHL. As muscle length adaptation can affect muscular tension, and as EHL activity dominates the length-tension curve, the EHL can develop more tension when the muscle is shortened (i.e., in the absence of MTPJ flexion). However, active MTPJ flexion during ankle DF curtails the capacity of the EHL to generate tension because the EHL is now lengthened. Thus, when prescribing exercise for TA activation, one should consider the relative activation of synergistic muscles. MTPJ flexion is helpful during DF exercise for isolated TA activation.
The DF force fell significantly with MTPJ flexion in both groups. These results support our research hypotheses. No previous studies have examined the DF force with MTPJ flexion; thus, it is not possible to compare the results of this study with others. However, the EMG activity ratio of the TA to the EHL during maximal DF showed that the DF force is more dependent on relative muscle activity of the TA and EHL. Thus, one might assume that MTPJ flexion is method for increasing DF force and selective activity for TA activation relative to EHL activation.
Our study had several limitations. First, the work was cross-sectional in nature; we did not explore the long-term effects of active MTPJ flexion during ankle DF. Second, all subjects were healthy and asymptomatic; our results thus cannot be generalized to larger populations. In fact, all subjects could be classified as “weak” in terms of ankle DF, as measured by the fifth percentile threshold of ankle DF strength [23]. Third, it was difficult to determine EHL dominance, which we defined operationally by reference to a TA/EHL ratio crossover of unity. Use of a different criterion might have changed our findings. Fourth, we measured only TA and EHL activities. Other muscles involved in ankle DF and big toe motion (including the EDL, PT, and abductor hallucis longus) were not studied. The effects of active MTPJ flexion in the context of the activities of other extrinsic and intrinsic muscles should be explored. Additionally, we did not assess the gastrocnemius and soleus muscle, even though active MTPJ flexion might induce overactivity in these muscles and cause pain; these muscles should be considered in a future study. Moreover, longitudinal studies are required to determine the long-term effects of active MTPJ flexion on the activities of diverse muscles during ankle in subjects with ankle and foot pathologies and deformities.
Conclusions
We measured the activities of ankle dorsiflexor muscles, DF AROM, and DF forces to demonstrate the effects of active MTPJ flexion in EHL-D and EHL-ND subjects. Such flexion during ankle DF efficiently inhibited EHL activity and increased the TA/EHL activity ratio in the EHL-D group. We thus suggest that active MTPJ flexion effectively reduces EHL activity and is associated with a higher TA/EHL activity ratio during active ankle DF in EHL-D subjects.
Footnotes
Acknowledgments
All authors contributed to the concept, design and data collection and analysis of this study. We appre- ciate Hye Jin Park for the data collections.
Conflict of interest
The authors have no personal, financial, or other conflicts of interest.