
Abstract
BACKGROUD:
Although the effect of exercise in patients during the subacute and/or chronic subacromial impingement syndrome has been reported, only a few studies have examined the effect of pain free exercise in the acute phase of this disorder.
OBJECTIVE:
To compare the effect of training using the Neurac technique which combines body segments suspension and vibration vs. manual therapy, on various relevant outcome parameters in patients with acute subacromial impingement syndrome (PASIS).
METHOD:
Twenty-six patients underwent a 4 week intervention program. Using random assignment, half of the patients were treated using the Neurac device while the other half was treated using manual therapy. The outcome parameters consisted of shoulder pain, shoulder function, range of motion (ROM) and the isokinetic strength of the external and internal rotators at 60 and 180
RESULTS:
Following either modes of interventions, the pain, function, and ROM improved significantly compared to pre-intervention levels in both groups. Time-by-group interaction was observed for the rotational strength which increased significantly and exclusively in the Neurac group.
CONCLUSIONS:
Given its positive effect on shoulder pain, function, ROM and the isokinetic strength of the external and internal rotators, we recommend the application of the Neurac technique in PASIS.
Introduction
Subacromial impingement syndrome (SIS) has shown to be the most common diagnosis of shoulder dysfunction, constituting 74% of shoulder pain cases [1]. Patients with SIS present with pain, dysfunction [2], limitation of range of motion (ROM) [3], and muscle dysfunction [4]. The lower activity of lower and middle trapezius, and serratus anterior, higher activity of upper trapezius have been observed in patients with SIS [5]. Imbalance of these muscles cause inadequate scapula upward rotation and posterior tilt which may contribute to a decreasing of subacrmial space [6]. Additionally, weakness of glenohumeral joint (GHJ) rotators especially that of the infraspinatus and subscapularis has been identified in patients with SIS [7]. This variation may result in abnormal glenohumeral movement which in turn may contribute to a reduction in the subacromial space [6, 8] and SIS [9]. Therefore, GHJ rotation strength is an important factor in SIS.
Rehabilitation programs for treating SIS refer to the following four phases: acute, intermediate, advanced strengthening and return to activity [10]. The acute phase relates to the first 4 weeks following pain onset or surgical intervention [11]. The clinical approach includes manual therapy and strengthening exercise [10]. GHJ mobilization has been used to reduce pain and inflammation and to increase ROM because this technique can be restore capsular extensibility and stimulate joint receptor [12, 13], and scapula mobilization has been used to increase scapula upward rotation and posterior tilting. In previous studies, additional GHJ mobilization were significantly decreased pain [12, 14], functional scores and increased ROM [14] compared with the control group. Also, Yang et al. [15] reported scapula mobilization was significantly increased scapula posterior tilting compared with the control group. Strengthening exercise in the acute phase are performed for restoring muscle balance and are important for preventing muscle atrophy and reduction of the rate of recurrence [10]. With respect to the muscular component, strengthening exercise for SIS focus on the serratus anterior, the lower trapezius, and the rotator cuff [6, 8], which together provide maintenance of the normal scapulohumeral rhythm and a possible increase in the subacromial space which eventually leads to prevention of SIS [6, 8]. In a previous study, Merolla et al. [16] demonstrated that scapular stabilization exercise has significantly increased the infraspinatus strength in volleyball players. Another study argued that rotator cuff eccentric exercise could bring about relief of pain and improvement of function [17]. However, some pain following exercise was experienced [9, 18], and consequently the type and available range of exercise were limited [19].
Recently, the Neurac technique has been introduced for treating patients with musculoskeletal problems [20, 21]. The Neurac technique has evolved from the Redcord trainer by adding vibration. The objective of this technique is to recover normal movement patterns and muscle strength by using neuromuscular stimulation enabled by suspending a part of the body in a Redcord trainer [20, 21]. The technique consists of 4 main components: 1. exercising under a weight-bearing condition thus encouraging muscle co-activation to provide joint stability [20, 22]; 2. controlling exercise intensity by unloading bodyweight [20] thus enabling exercise till end range with pain free condition; 3. increasing exercise intensity by decreasing the elastic cord support [20, 21, 23]; 4. providing vibration and increasing muscular activity via stimulation of the muscle spindle [20]. Our previous study showed that pain, function and ROM were significantly improved post-Neurac technique in patients with acute phase SIS (PASIS) [24].
Since application of the Neurac technique is not supposed to provoke pain it could be effective intervention method for patients in the acute phase of SIS. However, clinical evidence is insufficient while the underlying mechanism is unclear [23]. Furthermore, only a few studies have examined the effect of the Neurac technique on shoulder rotators strength in the acute phase of these patients. Therefore the objective of the present study was to study the effect of the Neurac technique on shoulder rotation strength, pain, function, and ROM in PASIS while comparing the latter to those resulting from manual therapy applied to a parallel cohort with similar characteristics.
Methods
The present study was a single-blind, randomized, and parallel-group study, conducted at P Hospital, Yangsan, Korea. This study was registered in the Clinical Research Information Service, with enrollment number KCT0001133.
Principles of exercise using the Neurac technique
Principles of exercise using the Neurac technique
KSE, kneeling shoulder extension; KPU, kneeling push-up plus; SSA, supine shoulder abduction; SSE, supine shoulder external rotation.
Twenty-six female SIS patients, who visited P Hospital, Yangsan, Korea, volunteered to participate in this study from August 2014 to February 2015 (a period of 6 months). Participant characteristics are shown in Table 1. All patients were examined and diagnosed by a physician. Inclusion criteria were: pain duration of at least 3 weeks since the first episode; pain produced or increased during flexion and/or abduction on the symptomatic side and at least four positive findings in the following five tests [25]: Neer sign, Hawkins sign, empty can test, painful arc of movement during flexion and/or abduction, and pain with palpation on the greater tuberosity of the humerus. Exclusion criteria were: a history of shoulder surgery, symptoms related to the cervical spine, frozen shoulder, disorders of the acromoclavicular joint, degenerative arthritis of the GHJ, shoulder instability and knee pain since the Neurac technique is performed in the kneeling position. Prior to participation, all participants read and signed an informed consent form approved by the Inje University Ethics Committee for Human Investigations.
All participants were randomly assigned to a group following the block randomization (block size
Interventions
Both the Neurac technique and manual therapy were performed by one physical therapist who had 10 years of experience and received appropriate training for both techniques.
Neurac technique. A: Kneeling shoulder extension (KSE), B: Kneeling push-up plus (KPP), C: Supine shoulder abduction (SSA), D: Supine shoulder external rotation (SSE).
GHJ and scapula mobilization
GHJ, glenohumeral joint.
Patients belonging to group N performed 4 exercises, 3 days a week for 4 weeks. Using the Redcord trainer (Redcord AS; Staudbo, Norway), these exercises consisted of (Table 1, Fig. 1): kneeling shoulder extension (KSE) for increasing lower trapezius strength; kneeling push-up (KPU) for increasing serratus anterior strength; supine shoulder abduction (SSA) for increasing shoulder abductor strength and supine shoulder external rotation (SSE) for increasing rotator cuff strength. The Redcord Stimula (Redcord AS; Staubo, Norway) was applied for providing vibration at 50 Hz [26, 27] during application of the Redcord exercises. This device was connected to the vertical ropes of the Redcord trainer. We also used elastic cords and straps to support the patient’s bodyweight during exercise. Prior to the exercise program, the participants were evaluated using the Redcord trainer in order to adjust the intensity of the exercise according to the presence of pain, compensatory movement and/or weakness. Thus, unloading of bodyweight or placement of the hand strap closer to the shoulder joint enabled control of the external moment-producing forces. A patient could move to a higher level of difficulty when the symptoms at the exercising level of difficulty subsided. This progression was effected by gradually reducing bodyweight unloading or by placing of the hand strap more distally. Subjects who experienced any pain could modify exercise stage. If the patients had pain during the Neurac technique, they told the physiotherapist, and the pain intensity was measured. Patients were instructed individually in all exercise sessions by a physical therapist who was skilled at employing the Neurac technique. Three sets of four repetitions were performed for each exercise, with a 30-s rest period between sets and a 1-min rest between exercises. It took 15 minutes to complete all sets.
The intervention program for group MT consisted of shoulder joint and scapular mobilizations (Table 2) for 3 days a week for 4 weeks [1, 12, 15]. The former was applied with long-axis distraction, anterior-posterior and inferior gliding [1, 12]. Long-axis distraction lasted 30 s with a rest time of 30 s between sets. Anterior-posterior and inferior gliding consisted of 15 repetitions of intensive grade 1–2 and 3–4 while the rate of one mobilization was 1–2 s. A rest time of 30 s was applied between all sets (Fig. 2). Mobilization of the scapula consisted of superior-inferior gliding, upward-downward rotation, and posterior tilting [15] (Fig. 3). Three sets of 15 repetitions were performed, with a rest time of 30 s between sets. Patients were treated by a physical therapist who was skilled at employing the mobilization of GHJ scapular. MT took 15 minutes to complete, which is the same as for the Neurac technique, and is thus comparable to the effective Neurac technique time.
Glenohumeral joint mobilization. A: Long-axis distraction, B: Inferior gliding, C: Anterior-posterior gliding.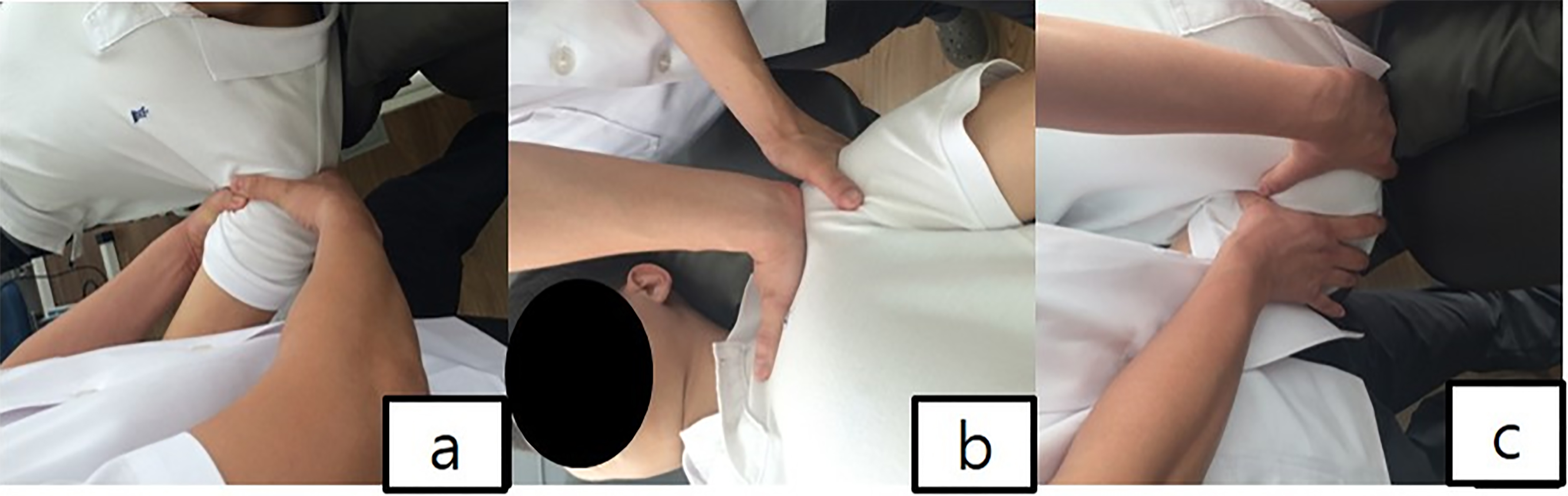
Scapular mobilization. A: Superior-inferior gliding, B: Upward-downward rotation, C: Posterior tilting.
Before and after the intervention, self-report questionnaires, ROM during internal and external rotation, and strength of internal and external rotators (IR, ER) were assessed. All evaluations were performed by the same evaluator who applied both the Neurac technique and MT.
Shoulder IR and ER strengths were measured with patients in the seated position with seatbelts placed over the chest and pelvis for proximal stabilization. For both ER and IR the arm was aligned with the scapular plane and abducted to 45
Shoulder pain level was evaluated using visual analog scale (VAS; 100 mm), which is believed to be reliable and validity to change [30]. A VAS score of 17 mm has been reported as the minimal clinically important difference [31].
Shoulder function was evaluated using the Shoulder Pain and Disability Index (SPADI), a 13-item self-administered questionnaire. This questionnaire has been shown to be valid and very reactive in evaluating pain and function, and SPADI is thus greatly recommended for use in patients with SIS [32]. The SPADI scores ranges from 0–130, with 130 indicating the worst level of pain and disability.
Shoulder internal and external rotation ROM were measured in the supine position with the arm abducted to 90
Statistical analysis
The sample-size calculation was performed using the free statistical package G*Power 3. Calculation was based on our pilot test because no study investigated the effect of intervention on the shoulder strength in PASIS. Eight participants (four participants from each group) took part in the pilot test used to determine the number of participants needed for this study (mean difference, 6.9%; standard deviation, 2.15%; effect size, 1.43). The result of the pilot test indicated that at least twelve participants per group would be required to detect a difference in peak torque/bodyweight 60
The statistical analysis was performed using SPSS version 20.0 for Window (SPSS Software, Chicago, IL, USA). Muscular strength in Nm was normalized and expressed in Nm/kgbw. A two-way repeated measurement analysis of variance (ANOVA) was used to determine the main effects and interactions for the VAS and SPADI score, ROM, and isokinetic strength. The within-group factor was time (pre-intervention vs. post-intervention) and group (group N vs. group MT). A
Results
Figure 4 presents the CONSORT flowchart of the study. Thirty-six potential participants contacted the assessor. Following the screening tests, 10 participants were excluded because they did not meet the inclusion criteria. There were no adverse effects reported or observed during or following intervention.
General characteristics of the subjects (mean
SD)
General characteristics of the subjects (mean
ER, external rotation; IR, internal rotation; VAS, visual analog scale; SPADI, Shoulder Pain and Disability Index; ROM, range of motion.
Changes in shoulder rotator strength, pre- vs. post-intervention
Changes in pain, function, and ROM, pre- vs. post-intervention
CONSORT flowchart of the study.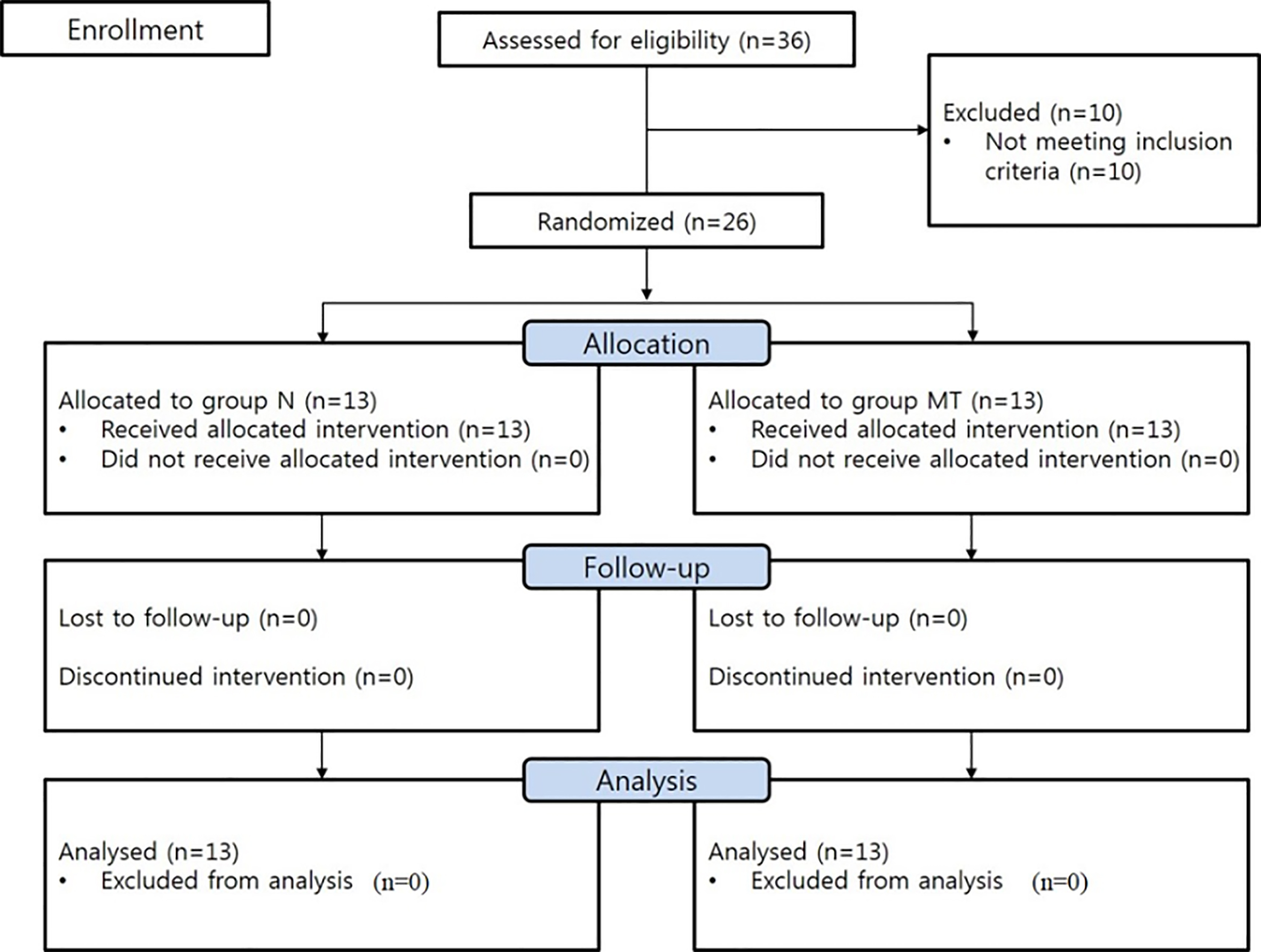
There were no significant inter-group differences found regarding any of the demographic or outcome parameters (Table 3). The experimental protocol was well tolerated by all participants and there were no complaints of pain or discomfort.
A significant time-by-group interaction was observed for Nm/kgbw at 60
No significant time-by-group interaction was indicated for VAS, SPADI, and ROM. However, significant improvements took place in both group in these outcome measures: VAS and SPADI scores significantly decreased post- vs. pre-intervention in both groups (
The main findings of this study are twofold. First, the Neurac modality and MT are an effective intervention in PASIS in terms of decreasing pain, elevating function, increasing ROM. Second, Naurac modality is also an effective intervention for rotational strength, and its beneficial effect in enhancing rotational strength, compared with the employment of MT which does bring about a similar effect, renders N a more effective treatment modality than the latter for this particular cohort.
The significant improvements in shoulder pain, function and rotational ROM demonstrated by PASIS following Neurac technique is consistent with other studies which have demonstrated that intervention of strength exercises resulted in a similar effect [9, 34]. These improvements might potentially be attributed to an increase in the subacromial space which in turn could be due to the strengthening of the serratus anterior and the lower trapezius, both of which are known to be involved in scapular upward rotation and posterior tilting [6, 9]. However, this contention is speculative since in this study the strength of these muscles was not quantitatively assessed. On the other hand, strengthening of the rotator cuff, which did take place, could maintain the humeral head in the glenoid fossa and produce inferior gliding of the humeral head during arm elevation [35], which could have a positive effect on these three outcome parameters. Furthermore, shoulder muscle strength and ROM are strongly correlated [36] and therefore the increased strength may have resulted in a wider ROM in group N. This aspect is supported by the nearly significant inter-group difference (
Pain, function, and ROM were also significantly improved in the MT group. Our results are consistent with other reports [12, 14]. The reduction of pain might be explained via the neurophysiologic pain reduction phenomenon [12]. GHJ mobilization may be stimulated type I and type II afferents articular mechanoreceptor and this would have reduced the awareness of pain reflexively [12, 22]. Conroy and Hayes [12] reported GHJ mobilization was significantly decreased 24-hour pain compared with the control group and other researchers reported an increased ROM after applying manual therapy compared to self-training in patients with SIS [14]. Also, GHJ mobilization may be stretched joint capsule [12], and scapula mobilization may increase scapula movement such as posterior tilting [15]. These may act to increase the subacromial space and improve pain, function, and ROM. Shoulder function as portrayed by the SPADI test is hampered by pain and therefore pain reduction is instrumental in bringing upon improvement in SPADI scores [1]. Thus, we propose that both the Neurac technique and manual therapy contributed to improved pain, function, and ROM in patients with acute-phase SIS.
Beyond the adaptive response to the progressive increase in load intensity enabled by removing the elastic cord used initially to unload body weight (BW) [20, 21, 23], there are other possible reasons for the observed increase in muscle strength in group N patients. First, it is possible that this variation was secondary to pain relief. Yang et al. [15] described the effect of Neurac technique using vibration on reducing pain in patients with cervical radiculopathy. Pain inhibits agonist activity [37] while pain relief increases muscle strength in patients with shoulder impingement syndrome [9]. Indeed the present findings demonstrate that following training with Neurac apparatus, pain significantly decreased. Second, applying vibration may have facilitated the primary endings of muscle spindle [38]. Increased excitatory entry to the alpha motor neuron pool through Ia afferents may facilitate muscle activation and maximal force [39]. Muceli et al. [27] reported that vibration during a short time period increased deep muscle strength in chronic pain patient. We chose to use 50 Hz as the vibration frequency during Neurac technique based on previous studies reported that the frequency 50 Hz is effective in muscle activity [26, 27]. Moreover, using this technique, it was possible to exercise to the end range under pain-free conditions using unloading of BW and vibration [20]. Exercise under these conditions may increase muscle activity leading to increased muscle strength. Third, some studies have demonstrated that an unstable condition can generate greater muscular demand for postural stability during exercise and could therefore lead to increased muscle strength [40].
The prescription of muscle strengthening exercise for PASIS is motivated by the need to prevent muscle atrophy and recurrence of symptoms as well as for restoring muscle balance. Hides et al. [41] have indicated that the recurrence rate was significantly lower when medication was coupled with specific exercise than medication and advice in patients undergoing the first episode of acute low back pain. By analogy, given the singular role of strength preservation in SIS we recommend that patients in the acute phase of this disorder perform well-guarded strength exercises, which improve shoulder rotators muscle strength in a pain-free manner. Notwithstanding, further research is needed to investigate the long-term effects of the Neurac technique on the recurrence rate after 1 year in PASIS.
The present study had several limitations. First, sample size was small and only women enrolled in this study. Thus, our results may not be generalizable to a wider population. Second, the duration of intervention was relatively short accounting possibly for the lack of significant inter-group differences in pain, motion and function. Third, one physiotherapist applied two intervention methods. Finally, this study focused on the rotator cuff but there is definitely a good reason to include muscles operating at the scapulothoracic level.
Conclusion
Comparison of the effects of the Neurac technique and manual therapy on pain, function, ROM, and muscle strength in patients in the acute-phase of subacrominal impingement syndrome revealed that both methods induced pain relief, improved function, and increased ROM. However, the Neurac intervention also resulted in a significant enhancement of shoulder muscle strength indicating its superiority as an effective therapeutic modality for this particular patient group.
Footnotes
Acknowledgments
This research was supported by a research fund of Pusan National University Yangsan Hospital.
Conflict of interest
The authors have no conflict of interest to report.