
Abstract
BACKGROUND:
Cervical spinal instability often leads to neck pain and forward head posture (FHP). To improve neck pain and FHP, both the suboccipital muscle inhibition (SMI) technique and cranio-cervical flexion exercise (CCFE) have been used. However, little is known regarding the validity of hamstring flexibility in neck pain subjects after CCFE as a treatment index, and comparison between the SMI technique and CCFE for neck pain treatment.
OBJECTIVE:
This study aimed to determine the short-term effects of SMI technique and CCFE, which represent passive and active exercise programs, respectively, and whether these improve the straight leg raise (SLR) test results, popliteal angle (PA), cranio-vertebral angle (CVA), and cervical range of motion (CROM) and are equally effective in immediate enhancement of such measures in neck pain subjects.
METHODS:
Twenty subjects with neck pain were randomly allocated to the SMI and CCFE groups (
RESULTS:
SLR test results, PA, CVA (sitting and standing), and CROM (flexion, extension, lateral flexion, and right and left rotations) after both interventions were significantly higher than those before the interventions (
CONCLUSIONS:
Both the SMI technique and CCFE improve SLR test results, PA, CVA, and CROM and are equally effective in immediate enhancement of the hamstring flexibility, CVA, and CROM in subjects with neck pain.
Keywords
Introduction
One of the predominant mechanical events causing neck pain, is impaired stability of the cervical spine, which is often attributed to disturbances in motor control over the cervical spine [1]. The stability of the cervical spine is dependent on the deep neck flexor and neck extensor muscles. The longus colli and capitis are principal deep neck flexor muscles and support the lordotic curve of the cervical spine against the tendency towards fastening of the cervical spine induced by head weight and/or the contraction of the powerful neck extension muscles [2]. In contrast, the suboccipital muscles are principal neck extensors of the upper cervical spine and are composed of the rectus capitis posterior major (RCPM), rectus capitis posterior minor (RCPm), obliquus capitis superior (OCS), and obliquus capitis inferior (OCI) [3]; further, they play a crucial role in promoting and resisting head motions, such as flexion, extension, and rotation in the cervical spine [4]. To relieve neck pain, the suboccipital muscle inhibition (SMI) technique and cranio-cervical flexion exercise (CCFE) have been used. The SMI technique significantly restores the upright posture in the cervical spine, measured by the cranio-vertebral angle (CVA), in asymptomatic subjects [5]. Similarly, CCFE improves the ability to maintain the upright posture of the cervical and thoracic spines during prolonged sitting after 6 weeks of treatment [6] and is known to activate the deep neck flexor muscles [7].
One of the common symptoms of neck pain is forward head posture (FHP). FHP is an excessive anterior head position in relation to a vertical reference line, as manifested by a reduced CVA [8]; it is characterized by an increased cervical lordosis or hyperextension of the cervical spine [9]. Accumulating evidence has indicated that the presence of neck pain and FHP can lead to delayed or inhibited activation of the deep neck flexors in the cervical spine, which is often accompanied by shortening of the opposing suboccipital muscles in parallel [10]. Therefore, a greater FHP was associated with a greater deficit in the cervical range of motion (CROM) [11]. Interestingly, a previous study demonstrated that increased tension and shortening of the hamstring muscle can cause neck and shoulder pain [12]. This occurs because the superficial back line of the myofascial chain connects from the neck to the lower extremity, and the soft tissue in the cervical spine links the dura and suboccipital muscle fascia [13]. Therefore, it is probable that if the tone of the suboccipital muscles is decreased (passively, with a fascial treatment or with active movements), the tone of the knee flexors (hamstring muscles) is reduced and the amplitude of hip flexion is increased, thereby increasing the straight leg raise (SLR) test score.
To date, several studies have investigated the effects of the SMI technique and CCFE in patients with neck and shoulder pain or hamstring tightness [5, 14] and found that the SMI technique improves hamstring flexibility and CVA, and that CCFE only improves the CVA and reduces pain. However, whether CCFE improves the CROM and restores hamstring flexibility and whether the SMI technique and CCFE, which represent passive and active exercise programs, respectively, are equally effective in immediate enhancement of hamstring flexibility, CVA, and CROM in a similar magnitude remain unclear. To answer these questions, we compared the hamstring flexibility, CVA, and CROM in subjects with neck pain before and after SMI technique and CCFE.
Methods
Subjects
We recruited 20 subjects with neck pain (13 men and 7 women) for this study (Table 1) and performed a PASS software (PASS 11. NCSS, LLC. Kaysville, Utah, USA) [15] analysis on the right SLR test results of a pilot study with five subjects. A total sample size of 10 subjects was required to satisfy a significance level of 0.05 with a power of 0.90. A double-blinded randomized controlled trial (pre- and post-intervention) was performed, and randomization was conducted according to a website (
Baseline characteristics of each group (
20)
Baseline characteristics of each group (
SMI, suboccipital muscle inhibition; CCFE, cranio-cervical flexion exercise; NRS, numerical rating scale; NDI, neck disability index. Gender was statistically analyzed using the Fisher’s exact test, and other variables, such as age, height, weight, NRS score, and NDI, using the Mann-Whitney U-test.
SLR test
The SLR test determines specifically the tightness of the elastic component of the hamstring muscle [18]. It was performed in the supine position on an adjustable table, with the lower extremities extended and the feet relaxed. The first evaluator held the talus without rotating the hip joint. The subjects’ leg was raised gradually, with the knee extended until resistance in the hamstring muscles was felt or until the evaluator observed the contralateral extremity or pelvis beginning to rise [19]. Thereafter, the second evaluator assessed the range of hip flexion using the AcuAngle
PA test
This test started from the supine position, with the lower extremity measured at 90
CVA
The CVA was measured directly using a digital camera (Sony A55, Tokyo, Japan) and ImageJ analysis software (ImageJ 1.8.0, National Institutes of Health, USA). One of the most commonly used methods for assessing CVA was obtaining a photograph of the lateral view of subjects [24]. The base of the camera was set perpendicularly to the height of the subjects’ shoulders, and the center of the lens was placed 1 m from the subjects. The measuring evaluator attached two body markers, one on the tragus of the ear and the other on the seventh spinous process [25].
The CVA was assessed in two different positions: a relaxed sitting position on a high back chair with both feet on the floor and a position with the hips and knees maintained at 90
CROM
This study used a previously described method using the universal goniometer for each measurement; the intra- and inter-tester reliabilities of the universal goniometer have already been reported [27]. To avoid errors and compensation during the neck ROM test, we measured the CROM in the sitting position. The subjects were asked to assume a neutral sitting position on a high back chair, with both feet on the floor, and maintain the hips and knees at 90
(A) Cranio-cervical flexion exercise using a pressure biofeedback unit, (B) Suboccipital muscle inhibition technique.
A total of 20 subjects with neck pain from Korea University Hospital were recruited in this study. Although 30 subjects were initially recruited, six subjects were excluded because they did not meet the inclusion criteria of this study. In addition, four subjects withdrew because of missing SLR test results and CROM analysis data as a result of pain and discomfort. Consequently, the drop-out rate in our study was 16.67%. The experimental procedures are illustrated in Fig. 2.
CCFE
CCFE, as a low-load training, was used to assess and exercise the deep neck flexors of the upper cervical area (longus capitis and longus colli), rather than the superficial neck flexor muscles (SCM and AS) [29]. In the supine position, a pressure biofeedback unit (Stabilizer, Chattanooga, USA), such as an air-filled pressure sensor, was placed in the suboccipital area of the subjects’ posterior neck with head-nodding actions to target 2 mmHg from a baseline of 20 to 30 mmHg. Each stage was held for 10 s and repeated thrice; the subjects attempted to perform the exercise to the next pressure increment [22, 24, 26, 28, 30] with a 10-s rest between stages [29]. The subjects’ head and neck positions were checked by the investigator to ensure that the subjects’ level returned to the baseline 20 mmHg in the starting position without retraction and avoiding a rapid CCFE motion and dominance of the superficial neck flexors, such as the SCM and AS [30]. The validity and reliability of the method were established [31].
SMI technique
The SMI technique was also used as an intervention and performed in accordance with the literature [32, 33]. The subjects were placed in the supine position, with their eyes closed; the evaluator sat at the head of an adjustable table and placed both palms under the subjects’ head, contacting the evaluator’s index, middle, and ring fingertips of both hands with the metacarpophalangeal joints in 90
Data processing and statistical analysis
Statistical analysis was conducted using SPSS 22.0 (SPSS Inc, Chicago, IL, USA). The values in each group were expressed as mean
Results
General characteristics
The total study sample (
SLR and PA test
The SLR test results and PA in each group are summarized in Table 2. The two-tailed Wilcoxon signed rank test revealed that the SLR test results on the right and left sides after the SMI technique were
Comparison of the outcome measures for the two interventions (
20)
Comparison of the outcome measures for the two interventions (
Short-term effects of the SMI and CCFE on hamstring flexibility, CVA, and CROM within and between groups at pre- and post-intervention. The results are expressed as mean
The CVA in the sitting and standing positions of each group is listed in Table 2. The two-tailed Wilcoxon signed rank test revealed that the CVA in the sitting and standing positions after the SMI technique was
Experimental procedures used in the study (SMI, suboccipital muscle inhibition technique group; CCFE, cranio-cervical flexion exercise group; SLR, straight leg raise; PA, popliteal angle; CVA, cranio vertebral angle; CROM, cervical range of motion).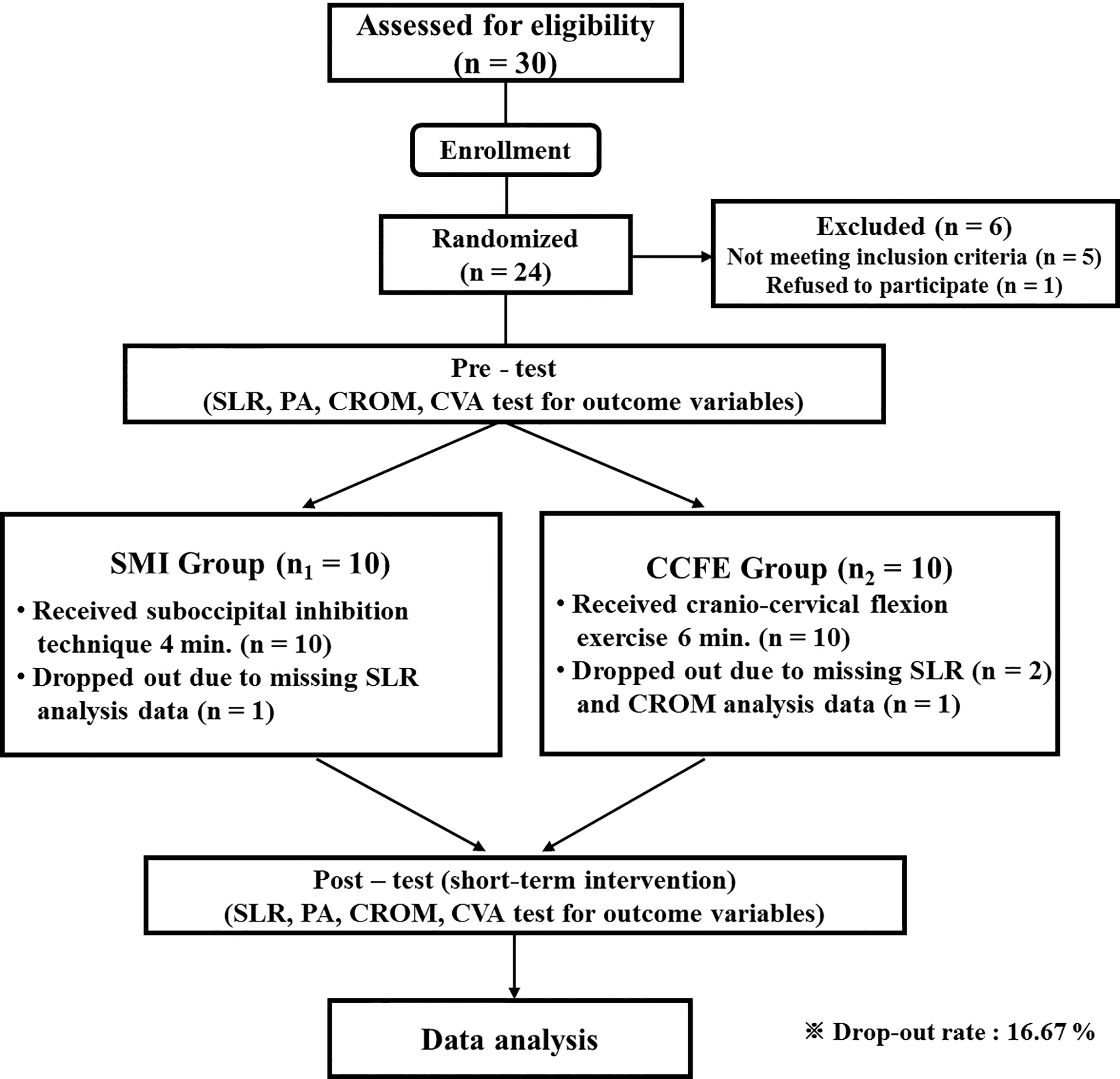
The CROMs in each group are listed in Table 2. The two-tailed Wilcoxon signed rank test revealed that the CROM in cervical flexion and extension after the SMI technique was
Discussion
The results of the present study demonstrate that both the SMI technique and CCFE, which represent passive and active exercise programs, respectively, improve SLR test results, PA, CVA, and CROM and are equally effective in the immediate enhancement of the hamstring flexibility, CVA, and CROM in subjects with neck pain.
The SLR test results and PA, after both the SMI technique and CCFE, were significantly higher than those before, and these results after the SMI technique improved to the levels similar to those observed after the CCFE. Although the mechanism of how the CCFE increases SLR test results and PA is not clear, it is possible that the CCFE induces selective stretching and eccentric contraction of the RCPm and RCPM muscles because the occipitoatlantal and atlantoaxial joints are slightly flexed [36, 37]. Interestingly, Pontell et al. [13] found that the OCI, RCPM, and RCPm of the suboccipital muscles are attached to the cervical dura mater via myodural bridge connection [13]. Based on this finding, it is also probable that the reduced tension in the myodural bridge after the SMI technique and CCFE may alleviate dural enfolding, thereby reducing the provocation of the nociceptive pain mechanism. Therefore, our results suggest that the direct release of the posterior neck area after the SMI technique and reciprocally eccentric lengthening of the suboccipital muscles after the CCFE facilitate greater stretching and reducing of the tone of the myodural bridge and hamstring muscles.
The CVAs in the sitting and standing positions after the SMI technique and in the standing position after the CCFE were significantly higher than those before the SMI technique and CCFE, respectively. The CVA in the standing position after the SMI technique improved to levels similar to those observed after the CCFE. A previous study reported that a common consequence of FHP is because of a prolonged hyperextension of the neck or increased cervical lordosis, and is closely associated with hypertonicity and shortening of the sternocleidomastoid muscle and the posterior neck extensors (suboccipital, semispinalis, splenii, and upper trapezius muscles) [38]. Interestingly, Watson and Trott [39] found that the upper and deep neck flexors have a higher content of Type 1 fibers than Type 2 fibers and provide a “holding mechanism” for stability and balance of the head and neck [39]. In support of these possibilities, reduced activation of the deep neck flexors, reduced ability to release the cervical muscles, and increased superficial neck flexor activities alter the feedforward control. As a result of these factors, delayed voluntary muscle activity could lead to pain and dysfunction in the control of the cervical spine [40]. Based on this finding, it is also possible that the SMI technique and CCFE reduce hypertonicity, especially in the suboccipital and superficial neck flexors, and resolve active trigger points. In addition, resolution of active pain by a reduced nociceptive input from the trigger points into the trigeminal nerve would influence the recovery of the neutral head posture [41]. According to this scheme, the mechanism of exercise-induced adaptations of the motor system depends on some factors, including muscular [42] and neuronal changes; the results of the present study are in agreement with those of previous studies [43].
The CROMs in all directions of the cervical movement after the SMI technique and in the cervical extension, lateral flexion, and rotation of the right side after the CCFE were significantly higher than those before the SMI technique and CCFE, respectively. The CROM in all directions of the cervical movement after the SMI technique improved to the levels similar to those observed after the CCFE. A previous study reported that reductions in the CROM can occur from structural changes in the soft tissue and inactivity of the muscles in the cervical spine and result in augmentation of connective tissue density and shortening and fibrosis of the muscle and collagen tissues [44]. To resolve these problems, Pilat [32] suggested that the SMI technique is of significance for the cranio-cervical area and is often used to decrease hyperactivity and tightness in the deep upper cervical tissue. Interestingly, bilateral suboccipital release and stretching of the fascia of the posterior neck decompress and relieve the vagus nerve, which runs through the jugular foramen [13, 45]. Based on this finding, it is also feasible that the SMI technique could help restore the normal flexibility of the cervical muscles, and normal autonomic function and cervical ROM are reestablished. In another study, Folland [46] stated that improved performance owing to the low-load nature of the intervention and the short duration of the CCFE likely reflects neural rather than peripheral adaptations. In support of this possibility, it could explain the several mechanisms that rapid improvements in task performances after active and repeated movements, including changes in the excitability of the motor cortex and neurons, increased motor function secondary to the pain-relief effect or improved activation of the motor neurons secondary to the activity of the descending pathway [47]. Based on the findings of these studies, our study confirmed that the movement of the cervical spine is increased owing to the relaxation of the soft tissue of the upper cervical region and improvement of the deep flexor muscle activity and motor control ability.
Although favorable outcomes of the SMI technique and CCFE were demonstrated by the intergroup and intragroup comparisons, there are some limitations of our study that can be corrected in future research. First, we used a cross-sectional design to investigate the short-term effects of the SMI technique and CCFE; however, we did not perform a long-term follow-up, and we do not know whether the level of activity of the subjects actually improved in the long run. Thus, the results of the present study cannot be recognized as the long-term effect of the SMI technique and CCFE on the SLR test results, PA, CVA, and CROM in subjects with neck pain. Second, the present study recruited subjects with 3 to 6 points in the NRS with hamstring restriction; there are limitations in the generalization of the subjects with other site problems or severe neck pain. Future studies are necessary to evaluate the limitation of the ROM in the cervical spine of patients with severe neck pain and FHP. Finally, in the present study, we did not measure biomechanical or kinematic parameters, such as relative joint moments, muscle activation, and proprioception of the cervical spine. Therefore, future studies that provide direct qualitative parameters measuring the biomechanical parameters and electromyography recordings from the cervical and hamstring muscles are also necessary.
Conclusion
In conclusion, these results suggest that both the SMI technique and CCFE improve the SLR test results, PA, CVA, and CROM, and are equally effective in immediate enhancement of the hamstring flexibility, CVA, and CROM in subjects with neck pain.
Footnotes
Acknowledgments
Authors are grateful to all subjects involved in this study, as well as authors/publishers/editors of all articles, journals, and books reviewed and discussed for this study. This research received no specific grant from any funding agency in the public, commercial, or profit sectors.
Conflict of interest
All authors were fully committed to absolute integrity and remained unbiased throughout the study. None of the authors had any conflicts of interest or carried any commitments that would influence their duties.