
Abstract
BACKGROUND:
Many studies report a relationship between poor static posture (SP) and low back pain (LBP). This study examined the effects of a biofeedback postural training program on pre-existing LBP, changes to level of physical activity and workability in participants.
OBJECTIVE:
To determine if static posture training with biofeedback alleviates LBP.
METHODS:
The control group wore a pedometer to track level of physical activity and the experimental group wore the postural training device, Lumo Lift, for three weeks. Participants completed the Cornell Musculoskeletal Discomfort Questionnaire (CMDQ) and completed pre- and post-intervention side-view pictures to evaluate changes in posture. Participants were predominately-sedentary work environment (
RESULTS:
LBP discomfort was statistically significant when comparing pretest and posttest CMDQ mean score in all subjects [F(1, 18)
CONCLUSIONS:
Postural training with biofeedback application helps with LBP management by decreasing level of LBP discomfort. People with LBP should be aware of their static posture and develop good muscle strength and endurance in order to maintain performance at work, school, or sports.
Introduction
Low back pain (LBP) is a leading health problem in many industrialized countries with lifetime occurrence rates of idiopathic LBP from 60% to 70% [1]. Several studies have linked increased LBP with prolonged sitting along with faulty back posture, lack of mobility, low muscular strength, or excessive body weight [1, 2, 3, 4]. Prolonged poor static posture causes LBP which limits activity, interferes with work, increases absenteeism, and reduces work productivity [4]. LBP is also becoming one of the major health risks in adolescents as this age group is registering sixty hours or more per week on electronic devices [5]. Poor static posture causes muscle imbalance by using more muscles on the preferred side of the spine and leads to ischemia, muscle fatigue, and chronic LBP [6]. Therefore, spinal health education in static postures is key to overcoming one of the world’s current health risks.
Maintaining neutral spine in static posture supports circulatory, musculoskeletal, and respiratory system function [7]. Neutral spine includes normal curvature of the spinal column: cervical lordosis, thoracic kyphosis, lumbar lordosis, sacral kyphosis, and coccyx lordosis. Each spinal region requires neutral curves to absorb external force and protect the spine from activities of daily living without damaging intervertebral discs [8]. To educate an individual on good sitting or standing posture, it is necessary to understand static posture patterns of the living environment during activities [10]. The education of good posture provides appropriate compensatory influence, such as postural training with feedback, to achieve optimal spinal function [10].
Biofeedback technology is commonly used as a training device for sensory, motion, symmetry, or weight distribution [10]. Lumo Lift (Lumo Bodytech, Mountain View, CA, USA) is a postural training device that uses a triaxial accelerometer to set target posture and monitors body position to provide a vibration stimulus alert when good body posture is not being maintained [11, 12]. The device provides feedback on the user’s posture by keeping track of the number of good posture hours and the number of steps taken while worn [13]. Posture training of the thoracic region with biofeedback by a motion sensor may reduce pain, decrease excessive thoracic curve in standing positions, and increase physical activity [12, 13].
Experts on LBP treatment recommend maintaining a physically active lifestyle as an essential component in LBP management for a sedentary population that maintains static posture for a long period of time [13]. A major health benefit of regular physical activity or exercise is improving the quality of life and reducing musculoskeletal pain [13, 14]. For example, walking is a fundamental activity that is a simple, low cost, and maintainable activity for establishing good health on daily basis [8, 14, 15]. Increasing the number of steps and the duration of exercises each day may relieve LBP due to changing activity habits, creating a better mood, increasing the level of performance by achieving better pain tolerance and reducing musculoskeletal pain [8, 9, 15, 16].
There is limited evidence of LBP alleviation using postural training with biofeedback, and even less evidence of new postural feedback technology. Based on current research [2, 3, 4, 5], there are plentiful examples of prior evidence which has demonstrated that increasing level of physical activities and maintaining regular exercise routine may alleviate LBP. Thus, the primary purpose of this study is to determine the effects of postural training with vibrational biofeedback on pre-existing LBP. A secondary purpose is to gain an understanding the spinal health benefits of using a postural training device for improving the level of physical activity and reducing musculoskeletal pain.
Participant demographic data
Participant demographic data
Work environment data
A total of 31 participants with pre-existing LBP (13 men, 18 women; age
Description of Cornell Musculoskeletal Discomfort Questionnaire relative to low back pain
Description of Cornell Musculoskeletal Discomfort Questionnaire relative to low back pain
The inclusion criteria were individuals between 18–69 years of age in a sedentary work setting with self-reported pre-existing LBP. The exclusion criteria were people with no pre-existing LBP. In addition, all participants completed the Physical Activity Readiness Questionnaire to identify any health issues, recent injuries, and previous cardiovascular conditions prior to participating postural training. The university Institutional Review Board approved the study and all participants signed informed consent forms.
For experimental group, Lumo Lift was placed on the undershirt directly 2.54 cm below the center of left clavicle.
The control group used a pedometer on the left side of waist line.
Each participant completed a demographic survey and a Cornell Musculoskeletal Discomfort Questionnaire (CMDQ). The demographic survey consisted of anthropometric measurements and questions about work environment. Descriptive statistics for age, sex, height, and bodyweight are provided in Table 1. Work environment data including average hours of daily employment, requirements for sitting or standing, hours of sitting or standing, and required use of electronic devices on the job are shown in Table 2.
Participants answered the CMDQ based on their LBP at work the prior week. The CMDQ asks participants to rate frequency of LBP (never, 1–2 times last week, 3–4 times last week, once every day, or several times every day), the severity of discomfort (slightly uncomfortable, moderately uncomfortable, or very uncomfortable), and how pain affected their ability to work (not at all, slightly interfered, or substantially interfered). The LBP categories, description, and score scale of CMDQ are shown in Table 3. Kappa coefficient was 0.63 for testing validity of CMDQ on three LBP categories with
The experimental group utilized their smartphones to operate the postural training device and access data during work hours. Participants were instructed to place the device with the magnetic clasp onto the undershirt 2.54 cm directly below the center of the left clavicle (Fig. 1) and set their target posture with the device by sitting up straight before starting their work. Participants removed the device when they finished their work for the day. The device recorded good posture hours when a user maintained and met the target posture. The control group participants were instructed to place a pedometer on the left side of their waistline and use the device only during working hours (Fig. 2). Participants recorded their total steps at the end of each work day.
Pre and posttest side-view posture pictures with a plumb line.
The researchers took a side-view picture of each participant to observe and record their standing posture (Fig. 3) for pre and posttest measurement comparison. A plumb line was used as a reference of alignment for posture. Criteria of ideal spine alignment is through the external auditory meatus, midway through the shoulder, through the greater trochanter, midway through the knee joint, and through calcaneocuboid joint [9]. Participants stood in standard anatomical position: upright posture, facing forward, feet flat together, upper limbs at the sides, and palms facing forward [9].
The postural training device recorded and saved the data on each user’s smartphone via Lumo Lift smartphone application. The primary investigator collected good posture hours and daily steps from each participant weekly and transferred the data to an electronic spreadsheet. The control group’s daily steps data sheets were collected after twenty-one days of the experiment. Each participant in the control group received a sheet to fill out their daily steps at the end of each work day. The primary investigator collected the datasheets and transferred the data to an electronic spreadsheet. After finalizing the data collection, all data was transferred to SPSS for statistical analysis. The length of experiment for both groups was twenty-one days, and each participant wore a postural training device or a pedometer during work hours only.
At the completion of the intervention, all participants completed a posttest CMDQ, an experience feedback survey, and had a side-view picture taken (Fig. 3). The experience feedback survey was performed to evaluate each participant’s compliance, postural training experience, and consistency of data registration.
A mixed ANOVA was used for determining any change in LBP as a result of the interaction between the posture training device and the pedometer. A linear regression was used for predicting a relationship between the CMDQ pre and posttest mean score differences and the number of good posture hours in the experimental group. Appropriate sample size for both mixed ANOVA (42 participants) and linear regression (59 participants) were calculated via G*Power (Heinrich-Heine-Universität Düsseldorf, Germany).
An independent
Cornell Musculoskeletal Discomfort Questionnaire mean scores comparison
Average steps between the control and experimental groups
Calculated probability of pretest and posttest Cornell Musculoskeletal Discomfort Questionnaire scores
Comparison between postural training and pedometer groups in difference mean CMDQ scores from pre to posttest of experience (A), discomfort (B), and interference (C).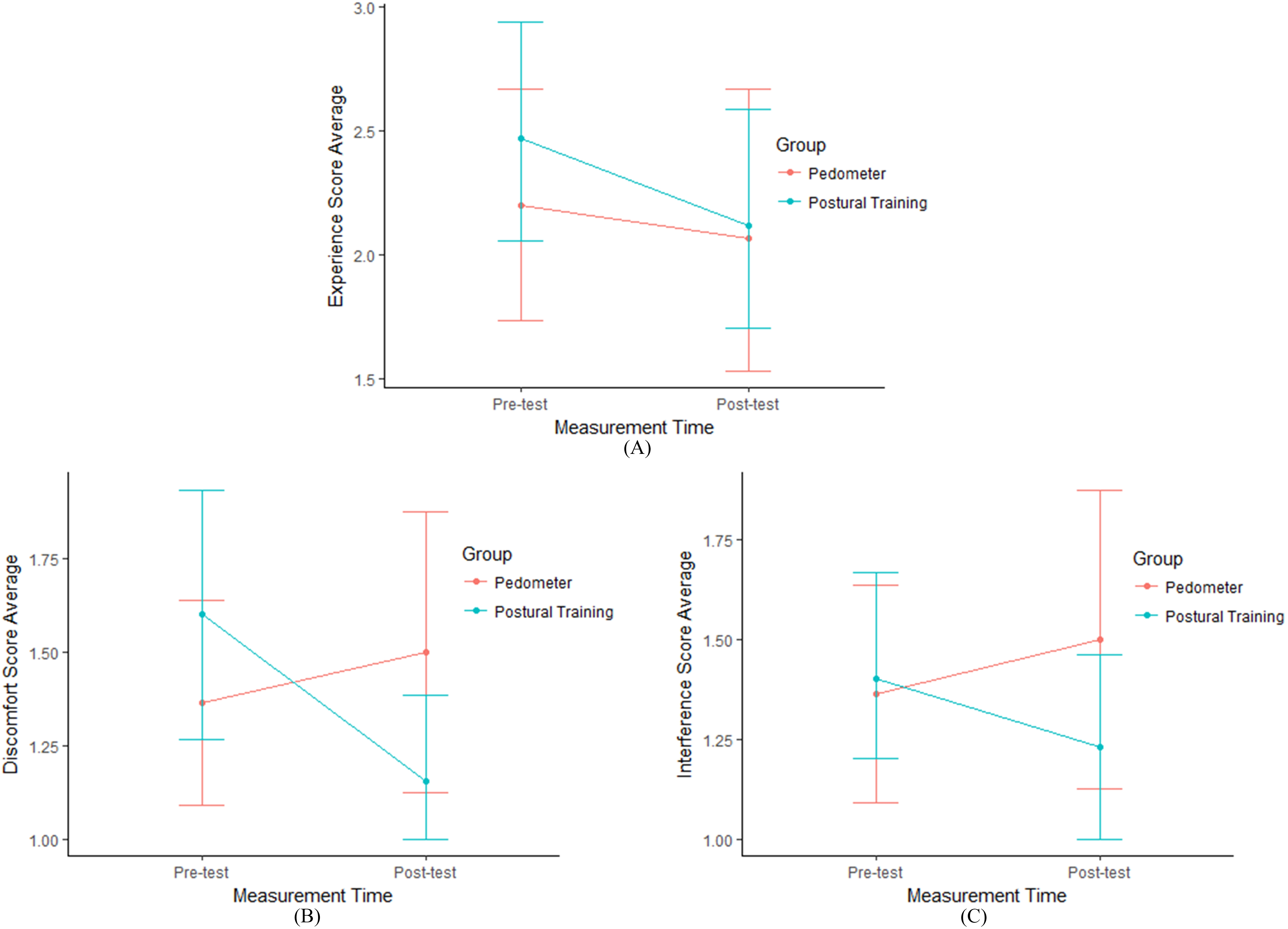
Mean and standard deviation of pre and posttest CMDQ mean score differences between the experimental and control groups are provided in Table 4. In the experimental group, each LBP category of experience, discomfort, and interference mean score decreased from pre to posttest. For the control group, there was a slight increase on LBP discomfort and interference of the CMDQ mean scores. The level of LBP related discomfort was significantly reduced with the postural training compare to the other LBP categories (Fig. 4B). However, the control group’s CMDQ scores on LBP discomfort (Fig. 4B) and interference (Fig. 4C) increased from pre and posttest measurements.
As the control group focused on daily steps by increasing their level of physical activity, the control group registered more daily steps than the experimental group. However, there was no significant difference on the level of physical activity between the two groups by observing the average number of steps between the two groups (95% CI
Calculated statistical significance of pre and posttest CMDQ mean scores are shown in Table 6. Between the experimental and the control groups, there was no statistical significance on LBP experience (
Statistical analysis between three LBP categories score difference from posttest to pretest and average good posture hours in the experimental group
Statistical analysis between three LBP categories score difference from posttest to pretest and average good posture hours in the experimental group
Relationship between the CMDQ difference scores of LBP experience (A), discomfort (B), and interference (C), to mean good posture hours in the experimental group.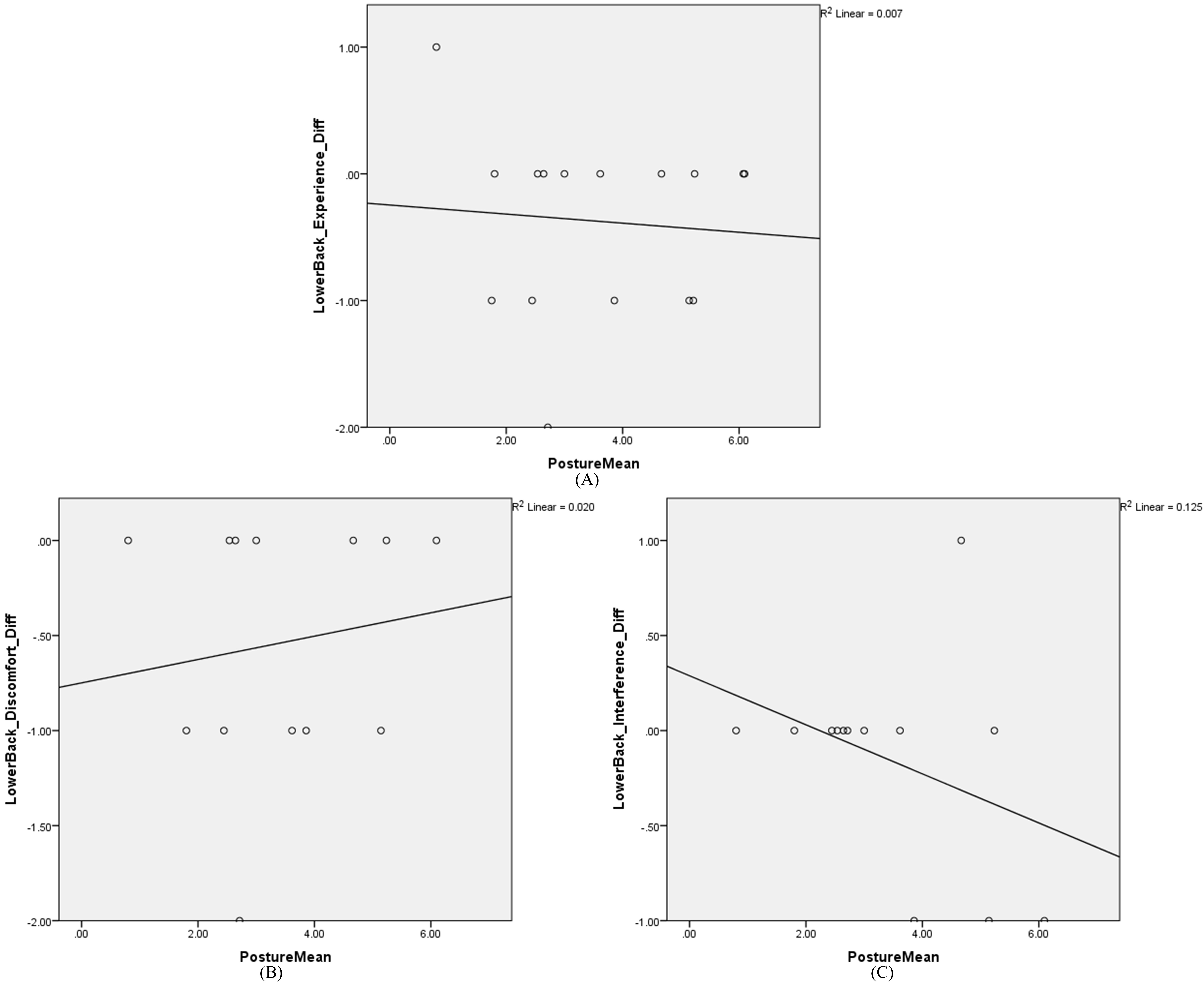
There was no relationship between the number of good posture hours and the CMDQ score changes on LBP experience (
The Pearson correlation coefficients for investigating the possible relationship between good posture hours and the CMDQ mean score differences explained that LBP experience (
Based on the results of this study, postural training with vibrational biofeedback reduced pain perception on the experience of LBP, discomfort level of LBP, and LBP-related work interference rates as participants in the experimental group received more feedback on their static posture from the postural training device. Figure 4 indicates substantial decrements in LBP experience (Fig. 4A), the rate of pain discomfort (Fig. 4B), and LBP-related work inabilities (Fig. 4C) in the experimental group. Many participants had spinal posture abnormalities such as forward head, hyperlordosis, or hyperkyphosis at the beginning of the experiment but the experimental group may have a refined proprioceptive awareness of upright spinal posture and experienced more neutral spinal posture at the posttest measurement as a result of wearing the Lumo Lift.
Postural training with biofeedback helps reduce stress, fatigue, and psychological disorders that are associated with faulty spinal posture [11, 18]. Using the Lumo Lift reduced the rate in experience, discomfort, and interference of LBP at work. Our findings from this study support previous findings [18]. Registering good posture hours and correcting faulty static posture for 3 weeks improved spinal posture by decreasing the time spent in poor static posture [19].
The CMDQ score on LBP discomfort was increased in the experimental group (Fig. 5B) as more participants obtained good posture hours. For example, it was difficult to tolerate corrected body posture and worsen their LBP by maintaining good static posture at work which some participants in the experimental group reported during the posttest measurement. In order to acquire good posture, sedentary individuals need to build up the proper muscle balance, strength, and endurance to stabilize the spine [21, 22].
Changing body posture may have led to muscle ache, muscle fatigue, or mental stress [22]. Therefore, the participants may have experienced psychological and physiological discomfort, such as mental irritation, muscle ache, and muscle soreness as their body adapted to a new working environment with the postural training device [18, 19, 20, 21, 22]. Increasing the level of exercise or physical activity such as jogging, walking, and running may be effective in reducing pain experienced by achieving a better quality of life at home, work, or school [23], or jogging can be beneficial to alleviate LBP [22, 23].
The level of discomfort from LBP (Fig. 4B) and LBP-related work interference (Fig. 4C) increased in the control group. Premature development of postural muscles such as multifidus, transverse abdominis, and diaphragm [6, 19, 20, 21, 22, 23, 24, 25, 26] and prolonged physical activity with low integrity, less stabilization, and incorrect spinal posture can result in inadequate static and dynamic spinal movement in everyday life [23, 24, 25, 26].
The American College of Sports Medicine recommends sedentary individuals should gradually increase the duration and intensity of physical activities to avoid any injuries or illnesses [24]. Additionally, the rapid increase of physical activities, like registering a high volume of daily steps taken each day, can cause muscle damage or body homeostasis disruption by rapid energy consumption and overused musculoskeletal system which may have led to a higher score on LBP discomfort and interference of the CMDQ in the control group [25].
Recent studies suggest that the brain can develop new paths by rewiring neurons to change an old habit, and the Lumo Lift may help the brain to recognize new patterns, perspectives, or movements [27, 28]. After conducting preliminary evaluations between the pre and posttest side-view picture for participants in the study, the control group had no significant changes in standing posture. However, the experimental group had several positive postural changes in the upper body region such as neck and shoulder. The cervical spine moved to a neutral position from flexed cervical spine with a normal lordotic curve. The shoulders appeared to open up more with increased thoracic spine extension from protracted to retracted positioning at posttest.
Individuals who receive feedback on posture can correct their static posture in sitting or standing and reeducate the neurologic system to adjust spinal alignment [14, 24, 25]. However, intensive postural training might be detrimental for a sedentary population by creating rapid changes in their body system [25, 26, 27, 28]. Moderate duration and intensity of postural training benefits people with pre-existing LBP and provides a positive work environment by reducing pain perception, level of discomfort, and lost work time [25, 26, 27].
Limitations
Compliance for utilizing the postural training device as requested may have led to inconsistent tracking during each individual’s work day. Some participants forgot to wear the postural training device when they switched clothes each day; therefore, there is a possibility of insufficient data to generalize claims for use of a postural training device. Unforeseen variables such as losing the device, forgetting to reattach the device after taking a shower, or dropping the device unintentionally could have led to inconsistency or inaccuracy of registered measurements.
The posture tracking device uses wireless technology that monitors sitting or standing posture which can result in inconsistent recording when there is a wireless connection problem. Some participants reported that their smartphone could not register good posture hours when the Bluetooth connection to their phone was not stable.
Reliability and validity of the Lumo Lift were not evaluated prior to the research study. However, the device was used in a recent study for evaluating posture tracking and correction. The device registered instantaneous static posture tracking and provided accurate static posture in prior research [30].
Conclusion
Maintaining good posture may support healthy behaviors and reduce lost work time due to LBP. Also, improving levels of physical activity can provide a positive effect for managing frequency of LBP in everyday life. People with LBP should be aware of their static posture and develop good muscle strength and endurance so they have a better chance of increasing performance at work, school, or sports where dynamic positions are needed.
When people can manage their spinal health by implementing a simple healthy lifestyle of maintaining good static posture or increasing level of physical activity with low cost effective strategies, people are less likely to spend excessive time and money on health care for LBP. In the United States, the cost of musculoskeletal-related treatments increases every year and the estimated cost for LBP health care could be anywhere from 77 to 240 billion dollars per year [31]. In order to reduce the average cost of health care in the United States, it is essential to increase awareness of spinal health so that people may prevent poor posture related disorders like migraine, osteoporosis, cardiovascular diseases, type II diabetes, obesity, and respiratory system disease [7].
In future studies, researchers should implement posture analyzing tools such as motion capture and electromyography to evaluate positional angle and muscular activation on each spinal region such as cervical, thoracic, lumbar, and sacral spines. Furthermore, 3 to 6 months of postural training and follow-up may increase reliability and validity of measuring postural changes between pre and post postural training. More investigation of the value of postural training using wearable biofeedback technology in the management of LBP is needed.
Footnotes
Acknowledgments
We would like to acknowledge everyone who played a role in our academic and career accomplishments. We are very appreciative of the many people in the Springfield area including Missouri State University Sports Medicine and Athletic Training Department, MSU MSAT Class of 2017, Mercy Sports Medicine, and Springfield Public School System. Lastly, we would not have finished this research study without help from Dr. Erin Buchanan, Dr. Todd Daniel, and Emily Klug at Missouri State University Psychology Department and the Rstats Institute.
Conflict of interest
None to report.