
Abstract
BACKROUND:
The effect of different exercise modalities on the vascular structure has been the subject of clinical trials but there is not enough data about wrestlers.
OBJECTIVE:
This study aimed to compare the arterial stiffness parameters in adolescent wrestlers with those of age-matched sedentary controls to show the effects of long and heavy training.
METHODS:
This study was carried out as a case-control study. Thirty three (
RESULTS:
The mean age range was 15.9
CONCLUSION:
Bradycardia is an expected condition for athletes. SBP and DWS were found to be high in wrestlers, suggesting that arterial tissue is more susceptible to stress. The low IMT indicates the protective effect of regular exercise against atherosclerosis. It is known that regular exercise is good for the vascular structure while heavy exercise puts a load on the vascular structure. The fact that the elastic modulus, compliance, and distensibility do not differ between the groups suggests that structural changes in the adolescents have no effect on the vascular wall.
Introduction
Wrestling is an ancient Roman Olympic game and one of the oldest martial arts. An optimal cardiorespiratory fitness level is required during the game, regardless of sex and wrestling style, to provide motivation during the resting period [1]. For this reason, wrestlers undergo a long and heavy training program.
Overall, to achieve high-level wrestling perform-ance, training should be directed to developing anaerobic power and capacity, aerobic power, maximal dynamic and isometric strength, explosive strength, and strength endurance [2]. With regard to the anaerobic power and capacity, the available studies were in agreement about their critical importance toward reaching high-level wrestling success since these variables have discriminated well between successful and less-successful wrestlers regardless of age, weight classes, and wrestling styles [2, 3].
According to the current literature, low grade systemic inflammation increased late into the season, and a correlation was found with poor sleep quality in wrestlers. It is furthermore suggested that individual variability in oxidative stress status and lipid profile in wrestlers may modulate biochemical response to training. Based on this data, wrestlers may benefit from additional recovery time early into the season to prevent muscle fatigue and damage [4, 5].
Many ways of defining the biomechanical properties of the arterial wall exist. The most commonly used definition to express the viscoelastic property is stiffness, which expresses the relationship between change in pressure (
Methods
This study was designed as a case-control study. Thirty three (
The carotid artery was evaluated using a high-resolution Doppler ultrasound system (Aplio 400 Platinum; Toshiba Medical Systems Corporation, Tochigi, Japan) attached to a broadband linear transducer (PLT-704SBT) by an experienced radiologist. The transducer was placed 2 cm anterior to the bifurcation of the right carotid artery. The measurements included IMT and lumen diameters (diastolic diameter (DP) and sistolik diameter (DP)) of the artery during the end-diastolic and end-systolic phases of the cardiac cycle. Simultaneously, the pulse rate and pressures (systolic pressure (SP) and diastolic pressure (DP)) were measured using an automatic sphygmomanometer (OCR Vitagnost 2015; MARS, Taiwan) attached to the left arm.
The measurements from sonography and sphygmomanometer were pooled together to calculate the quantitative parameters reflecting arterial stiffness using the following formulas [8, 9]:
and
Elastic modulus
The descriptive and analytic data of the groups
The descriptive and analytic data of the groups
Abbreviations: DWS: diastolic wall stress, TAD: tension diastolic, TAS: tension systolic, IMT: intima media thickness, ELAS: elastic modulus, DIST: distensibility, COMP: compliance; BMI: Body Mass Index.
The approval for this study was granted by the Institutional Ethics Committee (protocol number: 200; 2016). After providing informed consent, volunteers were recruited from healthy individuals who had sedentary lifestyles, as assessed by the International Physical Activity Questionnaire (first category, inactive:
Distribution of the intima media thickness (IMT) of carotid arteries according to the groups.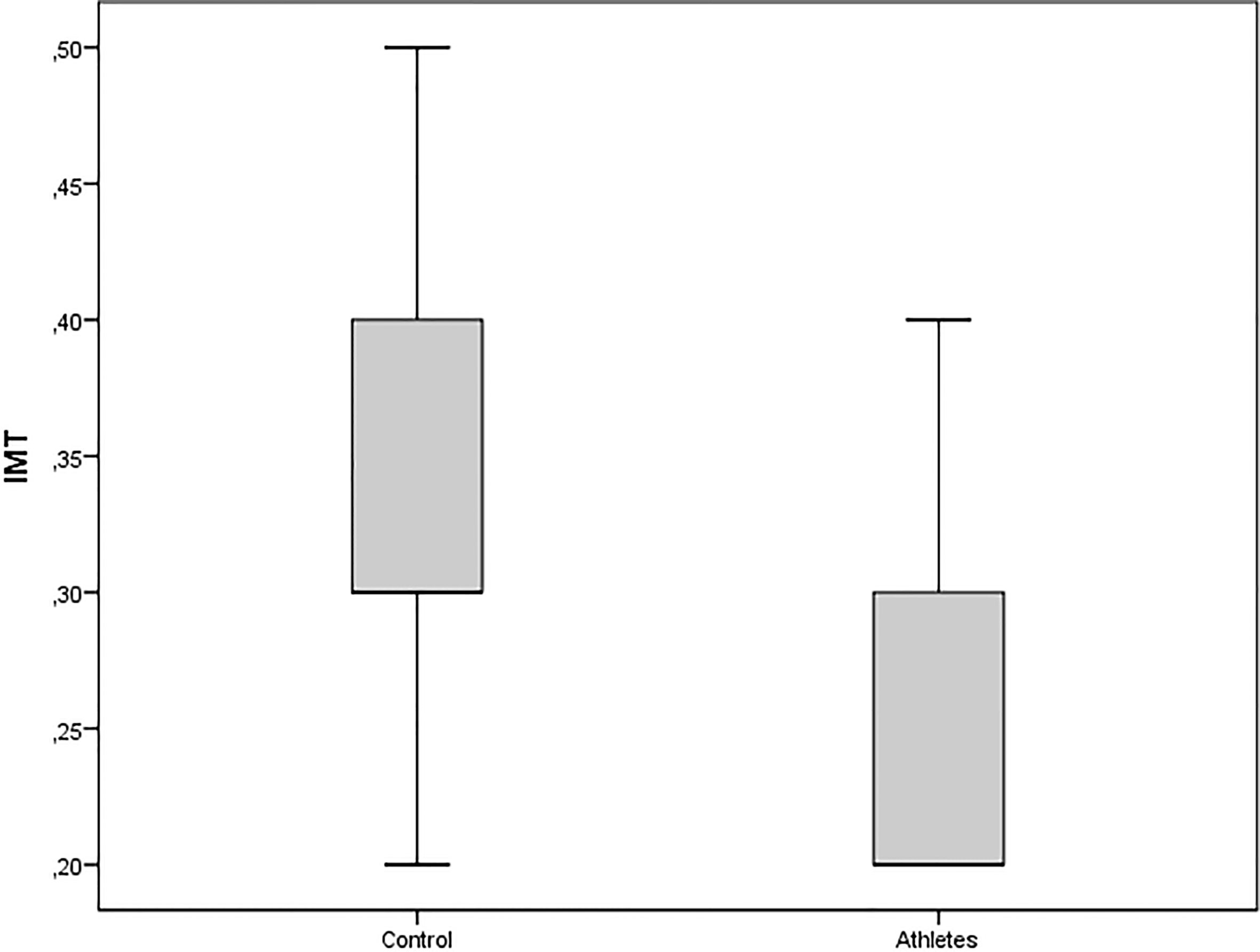
Measurements and calculations derived from sonography and sphygmomanometer were expressed as mean
Results
The mean age was 15.9
Distribution of the diastolic wall stress (DWS, mmHg) of carotid arteries according to the groups.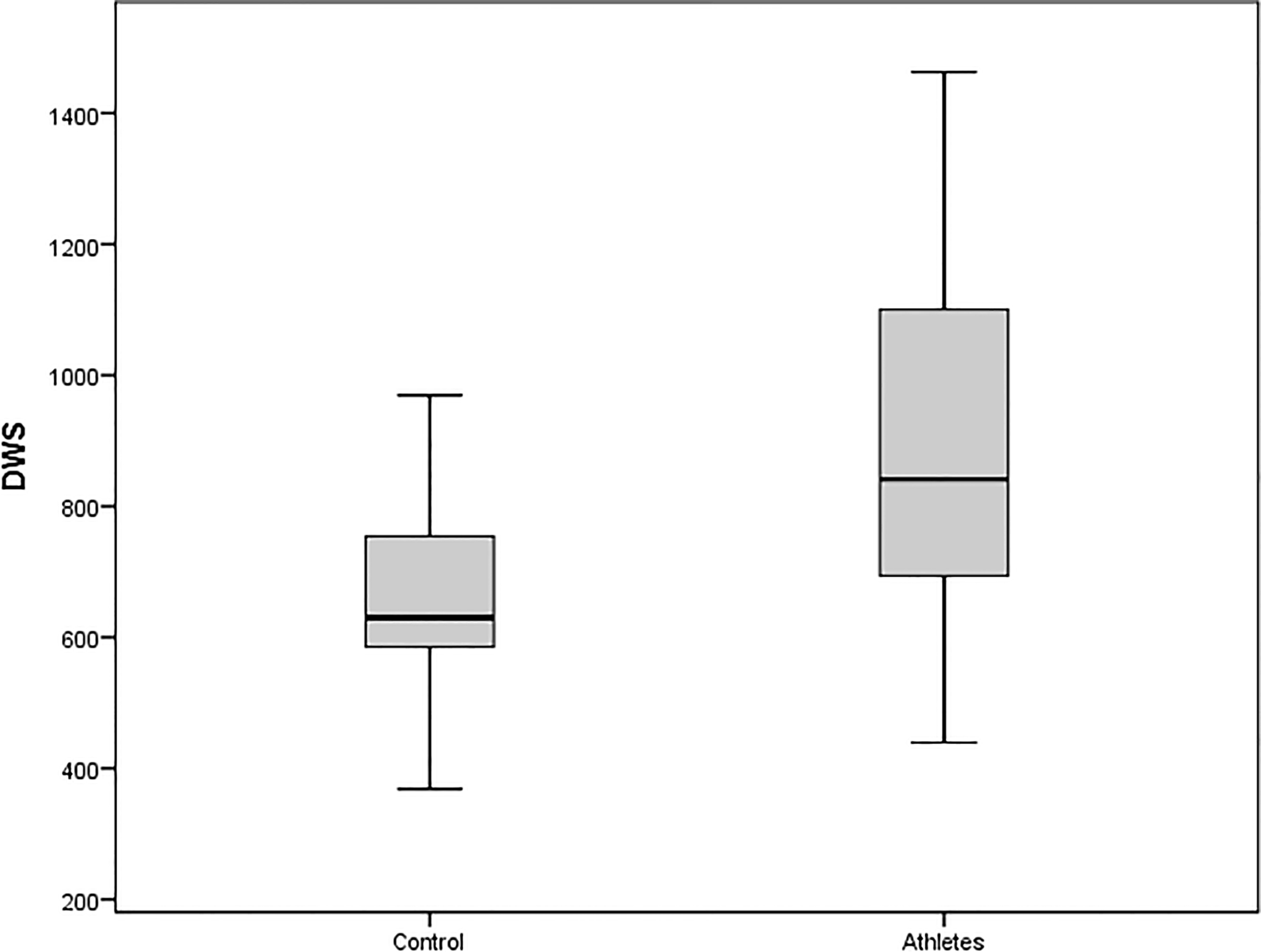
No significant differences were found in the elastic modulus (
Physical fitness parameters such as maximal dynamic strength, isometric strength, explosive strength, and strength endurance are closely related to high-level wrestling performance [2, 3]. Physical fitness has positive effects on vascularization in humans. Acute exercise causes rapid changes in arterial function, while recurrent exercise episodes cause chronic functional adaptation and structural arterial remodeling. These changes depend on the characteristic of the load [11].
Cardiovascular structures are constantly exposed to physical, chemical, and biological stresses during lifetime and subsequently develop vascular muscular hypertrophy and increased cross-linking of connective tissue, resulting in increased collagen deposition and marked distortion in elastin structures [12].
These events collectively accelerate with physical inactivity, subsequently leading to alterations in the biomechanical properties of the arterial wall and the development of increased stiffness or decreased distensibility [13]. The reduced elastic capabilities of the arteries are also associated with numerous diseases. Increased arterial stiffness serves as not only an indicator of vascular aging but also a predictor of end-stage organ damage. Therefore, arterial stiffness is often used as a clinical sign of mortality and morbidity, regardless of other risk factors [14].
Exercise modifies blood flow, luminal wall stress, arterial pressure, and tangential wall stress, resulting in changes in arterial diameter, wall thickness, and function. Some emerging adaptations resulting from hemodynamic stimulation after exercise training have significant clinical effects such as reduction of atherosclerotic risk in arteries, blood pressure control in veins, oxygen distribution and diffusion, and maintenance of microvascular health [15, 16, 17].
The effect of different exercise modalities on the vascular structure has been investigated in the literature. It has not been yet determined which exercise types (aerobic, resistance, or combination) are effective in cardiovascular health. There is no definitive answer to which is more effective on vascular health. Combination exercises are recommended in current practice. The fact that central arterial stiffness after maximal exercise was found to be higher in obese subjects than in healthy individuals suggests that arterial stiffness can be used as a tool to detect subclinical vascular dysfunction [18]. Large elastic arteries were found to harden with age, thereby increasing the risk of cardiovascular diseases. It has been observed that lower extremity interval exercise reduces central arterial stiffness in elderly individuals independently of aerobic exercise and systemic disease [19].
Resistant exercise training (RET) has different effects on arterial stiffness. Au et al. [20] found that RETs caused a decrease in central arterial stiffness in young healthy males regardless of the load weight and inactivity in local carotid artery distensibility or left ventricule mass [14]. RET has a positive effect on the vascular function. It is known that doing regular exercise is good for the vascular structure while heavy exercise creates a vasculature load. Resistance training (RT) has been widely recognized as an effective stimulus for increasing skeletal muscle size and strength. Resistance training is thought to stimulate muscle hypertrophy by increasing muscle activation and muscle swelling [21, 22].
Another study found that short-term aerobic exercise in sedentary individuals has some long-term effects on DWS and elastic module, but has no effects on arterial stiffness and distensibility. Short-term regular exercise also affects arterial stiffness parameters [22, 23]. Nishiwaki et al. [24] observed that 1-h stepwise exercise per week (8 weeks) in elderly women had a small but significant effect on the arterial stiffness [24]. They also observed that arterial stiffness was lower in young swimmers than in sedentary coevals [25]. Chung et al. [26] observed low arterial stiffness in middle-aged men with high cardiorespiratory endur-ance, muscle strength, and flexibility. Arterial stiffness was inversely correlated with fitness in healthy men. Regular exercise is recommended for middle-aged men to avoid arterial stiffness.
A BMI difference in adolescent males with no difference in height and weight was an indicator of having relatively higher muscle mass than fat mass in wrestlers in the present study. Bradycardia was also expected for all athletes. Long term endurance training, as done by elite athletes, is associated with cardiac neural remodeling in favor of cardioprotective vagal mechanisms, resulting in resting bradycardia and augmented contribution of cardiac parasympathetic nerve activity [27]. Systolic BP and DWS were high in wrestlers, suggesting that the arterial tissues of these individuals were more susceptible to stress. Ventricular wall stress is fundamentally involved in cardiac function. Increased ventricular wall stress is known to exhibit unfavorable consequences e.g. an adverse remodeling and imbalance between oxygen consumption and supply. It is hypothesized whether end-diastolic and end-systolic ventricular wall stress is associated with ventricular ejection and diastolic filling [28]. Wrestlers should be followed in terms of cardiac function regularly.
Intima-media thickness (IMT), also called intimal medial thickness, is the measure of the thickness of the innermost two layers of the arterial wall called tunica intima and tunica media. It is usually used for detecting atherosclerotic diseases. It was first described by Paolo Pignoli [29] in 1984. IMT became a useful tool to monitor the noninvasive changes on the artery wall [29]. IMT depends on several factors such as local hemodynamics, blood pressure, and stress. This measurement is usually done by external ultrasonography (US) and rarely by the internal invasive US catheters [30]. Exercise-related vascular health improvements can be evaluated by a number of clinical modalities: flow-mediated dilatation, carotid artery intima-media thickness and arterial stiffness measured by pulse pressure and augmentation index, etc. [31]. The low IMT values of adolescent wrestlers indicated the protective effect of regular exercise against atherosclerosis.
The study by Mangine et al. [32] suggests that following a short-duration training program (8-weeks), baseline size and strength have little impact on performance gains in resistance-trained individuals who possess similar years of experience [32]. Vascular smooth muscle cells are essential components that keep the tonus of the arterial network, which is the channel used to conduct the blood from the heart to the peripheral areas of the body. It is known that mechanical and architectural changes may lead to functional modifications in the cardiovascular system [33]. The cardioprotective effects of exercise training, including direct effects on vascular function and lumen dimension, have been consistently reported in asymptomatic subjects and those with cardiovascular risk factors and diseases [34].
Arterial distensibility is a measure of arterial ability to expand and contract with cardiac pulsation and relaxation. Low distensibility (increased arterial wall stiffness) has been introduced as a risk factor for cardiovascular disease [35, 36, 37]. In our study, an increase in distensibility due to regular exercise was expected in wrestlers. But no difference was found in elastic modulus, compliance, and distensibility parameters between the two groups. It could be concluded that the structural changes in the vascular wall of adolescents were not affected by the exercise training.
Conclusion
Physical fitness is essential for vascular health. Exercise-related studies have shown that exercise exerts a direct hemodynamic effect on the arterial wall. High-resolution sonography techniques can accurately measure the arterial wall motion and thus detect vascular pathological changes. Exercise reduces arterial stiffness. Sonography is a cost-effective method that assesses training performance by measuring arterial stiffness.
According to this study, the sonography results revealed that adolescent wrestlers have high BMI, systolic BP, DWS and low IMT and pulse in comparison to healthy controls. No significant structural changes were observed in the vascular wall of wrestlers.
Footnotes
Conflict of interest
None to report.