
Abstract
BACKGROUND:
For treatment of chronic musculoskeletal disorders pains to be successful, drug interventions are required.
OBJECTIVE:
In this study, we aimed to evaluate the Rational Drug Use Knowledge Level (RDUKL) in patients with musculoskeletal disorders and some relevant factors.
METHOD:
The study was carried out in October 2017 on patients treated in the Physical Therapy Rehabilitation Hospital in Turkey. The prepared questionnaire and RDUKL scale were administered to 239 patients by face-to-face interviews. The ANOVA test, chi-squared test and logistic regression model were used for the statistical evaluation.
RESULTS:
Forty-three percent of the study group was found to have Rational Drug Use Knowledge (RDUK). The patients who used medicines under family supervision had twice as much RDUK as those who did not use medicines under family supervision, and those who were university graduates had six times as much RDUK as those who had primary education or below. Scale score was found to be low in patients with fibromyalgia and high in patients with rheumatoid arthritis (
CONCLUSION:
RDUKL was found to be low in the group with chronic diseases and high average age. Besides training, it is important to provide patients with family support about their illness and its treatment. Thus, positive contributions can be made to the increase of the RDUKL.
Introduction
Medicinal treatments constitute for a significant part of initiatives for health services. For the treatment to be successful, it is expected that the patient’s awareness or compliance is high and the medicine is used wisely [1]. The concept of Rational Drug Use (RDU) is defined as individuals’ providing themselves and the society with appropriate medication according to clinical findings and individual characteristics for appropriate duration and at appropriate dosage at the lowest cost [2, 3].
The inability to provide any component of this definition is called Non-Rational Drug Use (NRDU). NRDU is a serious condition that harms both patient and health economics. Due to its importance, NRDU causes an increase in the cost of treatment, decrease in patient compliance, development of resistance to drugs, recurrence of illnesses and prolonged hospitalization, frequent adverse effects and increase in drug interactions. Despite the fact that the studies related to RDU have continued to increase for the last 30 years, NRDU continues to be an important public health problem for Turkey and the world alike. According to WHO estimates, more than 50% of medicines are prescribed, supplied or sold inappropriately [4, 5, 6].
In Turkey, 34% of general health expenditures are used for drugs. Among them, the musculoskeletal drugs are taking place the 5th order. Antibiotic and analgesic groups are among the most commonly used drugs. The majority of people who use these drugs can be said to be those with chronic disease, musculoskeletal system and joint pain [7, 8]. Especially in our region, existence of a 3rd stage hospital where diagnosis and treatment of musculoskeletal diseases are made and application of many patients have led us to conduct a study on this population. Assessment of RDU information of these patients with musculoskeletal complaints will be useful in determining compliance and awareness of drug treatment. Thus, interventions can be identified by health care providers and practitioners to ensure that patients receive more effective, safe and appropriate treatment.
In this study, we aimed to determine the RDUKL of the patients who were treated in the hospital due to musculoskeletal system complaints or diseases and some related factors.
Methods
Study group
This study was conducted in the city of Kütahya, located in the West Anatolia Region in Turkey. Kütahya is among the more developed provinces. Based on the register, as of 2016 the population of Kütahya totals 573,642. The city has one privately run hospital and one university hospital which includes two public hospitals and one Physical Therapy Hospital.
The study is a descriptive study on the patients who were treated at the Physical Therapy Hospital of Kütahya Evliya Çelebi Education Research Hospital in October 2017. Administrative permissions were acquired for the implementation of the study and approval of the local Ethics Committee was given (No. 2017-11/10). The study was conducted in accordance with the principles of the Declaration of Helsinki. Permission for using the scale was verbally obtained from Demirtas during an interview.
Without any sampling calculation, all of the approximately 250 patients who had physical inpatient and outpatient treatment in the hospital in October were included in this study. The study was completed with 239 patients (95% of the patients) who wanted to participate in the study. The data of the questionnaire prepared by the researchers were collected by face-to-face interviews with the patients.
The questionnaire
The questionnaire used in the study consisted of questions about their socio-demographic profile (i.e. age, sex, education, income level), drug use information and the questions of the “RDUKL” scale.
The RDUKL scale was developed by Demirtas et al. with choices of ‘Yes’, ‘No’ and ‘Don’t know’ for 21 questions. Each correct answer (‘Yes’) is scored as 2 points, while a wrong answer (‘No’) is scored as 0 points and ‘Don’t know’ as 1 point. Eleven negative expressions on the scale are scored in reverse. The minimum score that can be taken from the scale is 0, while the maximum score is 42. Cronbach’s alpha value of the scale is 0.789 and the cut-off score is 34 points. Patients who received 35 points and above were considered to have rational drug use [9].
Statistical analysis
SPSS package program was used in the evaluation of the data and the Kolmogorov Smirnov test was used for the normality test. Variables were normally distributed. Chi-squared test was used for analysis of percentages and descriptive data and the ANOVA test (The Games-Howell post-hoc test was preferred because the variances were not homogeneous) was used for analysis of mean multiple variables. In univariate analysis, variables with
RDUK logistic modeling according to some characteristics of the study group
RDUK logistic modeling according to some characteristics of the study group
OR: Odds ratio. CI: Confidence intervals. RDUK: Rational Drug Use Knowledge.
The study was completed with 239 patients of which the mean age was 58.83
67.6% of the study group had a physician-diagnosed chronic disease. According to the patients’ medical history, 17.6% had no daily medication, 24.3% had to use multiple medicines every day and 50.6% had medication under family supervision. 57.7% of the patients were treated as inpatients (Table 1).
Forty-three percent of the participants were found to have RDUK. Chi-squared analysis showed no statistically significant difference (
Multivariate logistic regression analysis with these variables (chi-squared analysis result
Distribution of patients’ diagnosis.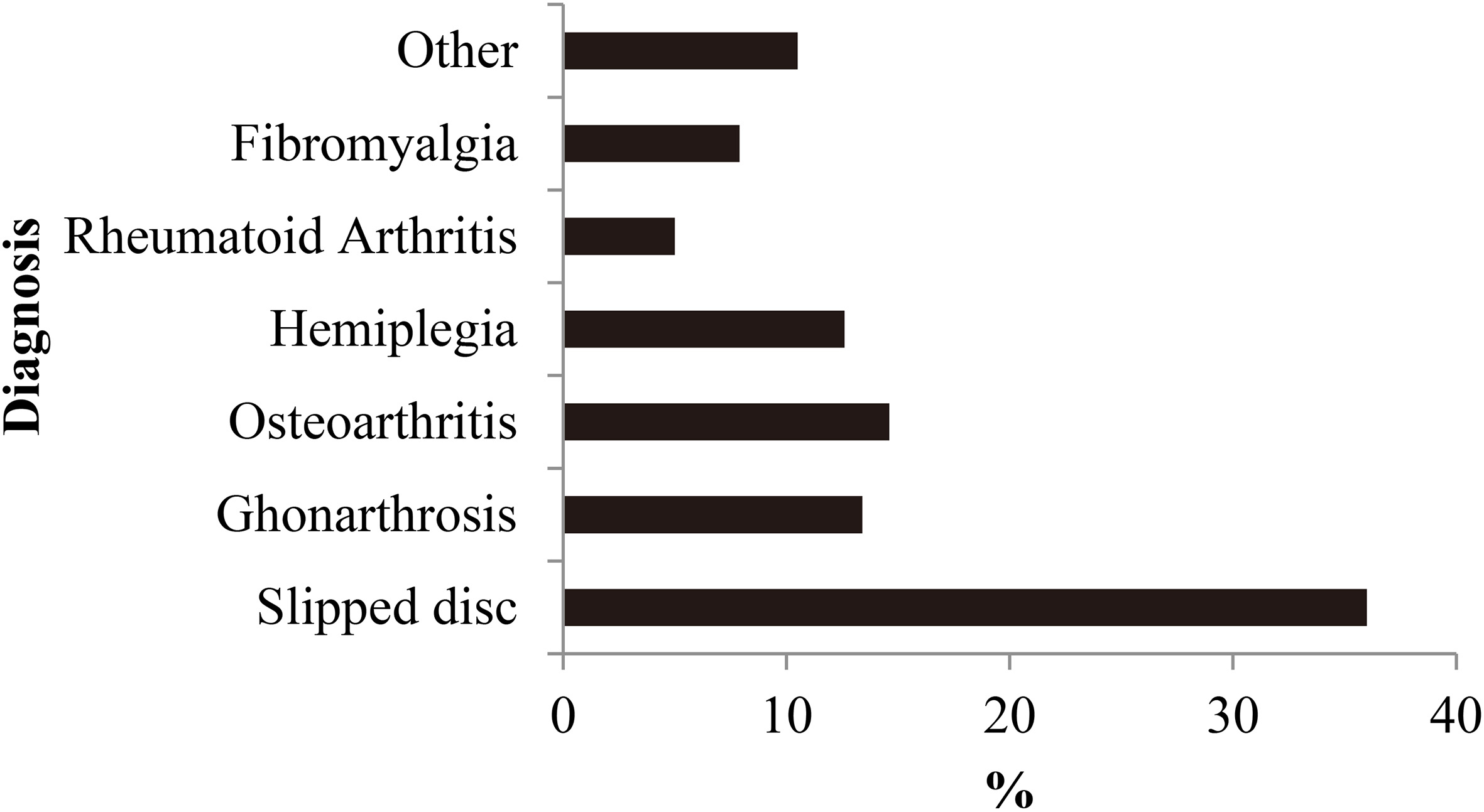
RDUKL scale score average according to patients’ diagnosis
SD: Standard deviation.
Figure 1 shows the diagnosis and prevalence of the disease for which the participants were treated. The mean of the scale scores according to the diagnosis of the patients were presented in Table 2. The mean score of the participants from the scale was 32.47
In the RDU, patients, doctors, health workers, relatives, the pharmaceutical industry and official authorities are all same parties. Awareness of the parties about their responsibilities ensures the healthy functioning of the RDU. It is very important for the physician to correctly identify the problem related to the patient and to give the correct diagnosis. Care should be taken to ensure safe, effective, affordable, cost-effective choices when treatment is planned. This provides positive contributions to treatment success and patient compliance. Other factors like age, gender, education, socio-demographic factors such as income, family support and drug use that may be associated with RDU were examined in our study.
Studies have shown that RDUKL’s less than 50% of patients generally in Turkey and the world [1, 3, 7, 8, 9]. In accordance with the literature, 43% of the participants with different chronic diseases were found to have RDUKL.
It is common knowledge reported in literature that RDUKL and attitudes towards it in people increase with the level of education [10]. Therefore, the fact that our study showed that the university graduate patients had 6 times more RDUK than the others was an expected result.
As the number of drugs used by patients increases, studies have reported that the rate of misuse of drugs and the incidence of adverse reactions increases as well [11, 12]. That is, they had polypharmacy and 24.3% of them had to use multiple drugs every day. It was found in our study that as the number of medications used increased, the frequency of having an RDUK increased too. The drug use behavior of patients using a large number of drugs was found to be more positive. This was a surprising result for us. This result may indicate that our study group had a high awareness of the drugs they used. However, the fact that 50% of our group used medicines under family supervision and this group had RDUK should be considered as a confounding factor. As a matter of fact, regression modeling confirmed this result. Presence of regular reminders in drug use is reported as an effective strategy to improve patient compliance [13]. Although the number of medicines used increases, the use of these medicines under family supervision shows that RDUK is has been supported positively.
The increased use of medicines with increasing age increases the frequency of mortality and morbidity and also brings problems with drug use in elderly. One of these problems is unreasonable multiple drug use [14, 15, 16]. RDUKL was found to be low in this group with chronic diseases and high average age. It is important to provide family support to patients besides training in their illness and treatment for it. Thus, positive contributions can be made to the increase of the RDUKL.
There are also studies showing that RDU awareness is high in patients with a chronic illness [17]. In our study, 67.6% of the individuals had one or more chronic diseases diagnosed by the physician besides diseases they were treated for. The RDUK of this group is higher than the non-chronic group, which supports the literature.
Studies indicate that treatment compliance in Rheumatoid arthritis is variable by 30–90%, and compliance for treatment is more common in the elderly population [18, 19, 20]. Especially in patients with Rheumatoid arthritis, the average scale score is in consistency with the literature.
In our study, patients with fibromyalgia were found to have low RDUK scores. Fibromyalgia is characterized by tender points in the body and proceeds with extra-articular, chronic and widespread musculoskeletal pain. Various analgesics are used in the treatment of these patients. Although sometimes too much and a variety of medications are used, full recovery may not be seen [21]. This situation can lead patients to NRDU. However, this may be the reason why Fibromyalgia patients have a low RDUKL.
The response rates of scale questions in the study by Demirtas et al. are similar to those in our study [9]. The highest level correctly answered items were ‘only physicians can offer medication’ and ‘we should consult our doctor when we have any adverse effects when taking medication’. These responses reflected participants’ positive attitude towards RDU and that their awareness was good. However, the answer was mostly ‘I do not know’ to the item ‘All drugs cause the same side effects’. This response suggests that our group had a significant lack of knowledge about side effects of drugs. The highest level wrongly answered item was ‘we can stop using medication when we feel good during treatment’. This response can be taken as one of the concepts that can be corrected with education in the context of NRDU.
In recent years, a wide variety of herbal medicines, nutritional supplements, vitamins and minerals have been used extensively in all over the world in addition to known medicinal products. In studies conducted in Turkey, the methods frequently used by patients are revealed to be herbal products. It is believed that herbal medicines, which are thought to be safe by the patients because they are natural, do not carry the risk of side effects and toxicity, and so are often used without doctor advice [22]. In our study, the majority of participants stated that herbal products could be used as a substitute for medicines and 9.6% of the participants applied herbal cures. Also important in terms of NRDU, putting herbal products on par with medication indicates the need for education in this regard.
Our study population was the patients who were treated in the Physical Therapy and Rehabilitation hospital. In the treatment process of these patients, rehabilitation services and spa treatment are applied besides drug treatment. In addition, patients are expected to benefit from alternative treatment methods. The actual problem is uncontrolled and unconscious use. 34.3% (18.8% bloodletting, 5.4% leech therapy, 4.6% acupuncture) of our patients stated that they had already used alternative treatment methods. In this group, the percentage of RDUK was lower than the group without alternative treatment methods and these methods were not doctor-controlled. Taking this into consideration, we believe it is necessary carrying out case-finding studies and organizing training on alternative-traditional treatment methods for raising awareness in the RDU issue.
One of the limitations of this work is that it is only performed on the selected instance because of time constraints. Another limitation is that because of it being a questionnaire study, memory factors can affect answers of patients. Lastly, the patients’ answers may have been partially affected due to hospitalization.
Conclusion
RDU is a concept that applies to all ages and treatments. Planning treatment especially in elderly patients requires a serious approach. It should be remembered that our study group had musculoskeletal disorders and was an elderly group. With aging, as well as the increase in the incidence of chronic diseases, the use of multiple drugs also increases.
In Turkey, elderly patients often go to different doctors, insist on getting a prescription and even take a large number of prescriptions. Many factors such as symptomatic drug prescription in elderly patients and the tendency of elderly patients to use drugs may be attributed to multiple drug use. We believe that the use of a low dose, which is effective in this process, can make a positive contribution to the success of the treatment if the dose increase is made slowly if necessary. At the same time, we advocate that alternative treatment methods that can be used besides drug therapy should also be proposed under physician control taking into account the profit-loss ratio.
Footnotes
Conflict of interest
None to report.