
Abstract
BACKGROUND:
Although the Pilates method has been reported to be effective in women with low back pain (LBP), the efficacy of Pilates exercises in pregnant women with LBP has not been evaluated widely.
OBJECTIVE:
The purpose of this study was to determine the effects of clinical Pilates exercises on lumbopelvic stabilization, pain, disability and quality of life in pregnant women with LBP.
METHODS:
Fourty pregnant women were randomized into either a Pilates exercise group (
RESULTS:
Pain and disability were significantly improved in the Pilates exercise group after intervention (
CONCLUSIONS:
Pilates exercises can be recommended as an effective and safe method for increasing lumbopelvic stabilization, reducing pain and disability, improving physical mobility and sleep problems in pregnant women with LBP.
Keywords
Introduction
Weight gain, postural changes and hormonal fluctuations in pregnancy may lead to musculoskeletal system problems [1]. Relaxin, a hormone secreted by the placenta particularly during late pregnancy relaxes pelvic ligaments and ligaments supporting the spine, however, the relaxed ligaments may trigger low back pain (LBP) in pregnant women [2]. LBP is the most common pregnancy-induced musculoskeletal problem. Many studies report that about 50% of women suffer from LBP during pregnancy [3, 4, 5, 6, 7, 8, 9, 10, 11]. This pain usually increases as the pregnancy progresses, and it can affect activities of daily life in pregnant women such as weight bearing, sitting and walking. It can also cause physical inactivity and insomnia in pregnant women [12]. Therefore, studies report that pregnancy-induced LBP negatively affects quality of life and leads to functional disability in pregnant women [13, 14].
It has been reported that non-pharmacological treatment methods include ergonomic modifications, frequent rest periods, hot and cold compresses, waist support belts, massage, acupuncture, yoga, manipulative practices and pregnancy-specific exercises improve pain, disability and sick leave with minor, transient adverse effects when compared to regular prenatal care [12]. Clinical Pilates is one type of exercise that is used to relieve LBP. The clinical Pilates method is a technique that focuses on increasing lumbopelvic stabilization and improving posture, breathing, flexibility, strength and muscle control [15]. The Pilates approach focuses on actively using body muscles to stabilize the lumbopelvic region [16]. There is evidence that Pilates is an effective approach to increasing strength of deep body core muscles [17]. Although the increasingly popular Pilates method has been recently reported to be more effective than other exercise methods in reducing LBP in women [18], only one study examines the effects of Pilates on LBP in pregnant women [19], which only focussed on pain in pregnant women and found that it was effective in reducing pain.
No studies were found that show the efficacy of clinical Pilates exercises on lumbopelvic stabilization strength, disability and quality of life in patients with pregnancy-related lumbar pain. The aim of this study was therefore to investigate the effectiveness of Pilates exercises on lumbopelvic stabilization, pain, disability and quality of life in the pregnant woman. We hypothesized that the Pilates exercise would result in a significant improvement in pain, disability, quality of life and lumbopelvic stabilization strength in pregnant women with LBP.
Materials and methods
Subjects
Forty pregnant women with LBP complaints registered at the Gynecology and Obstetrics Department Outpatient Clinic of Baskent University Medical Faculty for routine pre-natal care were allocated to this study over a period of 18 months. After a thorough evaluation of the pregnant women by an obstetrician in order to eliminate any systemic or obstetric causes that may mimic the same pain, the women were referred to a physiotherapist. The inclusion criteria for this study were: pregnant women in weeks 22–24 with pregnancy-induced lumbar pain; maternal age 20–35 years; parity
The exclusion criteria for this study were: multiple pregnancies; history of cardiovascular diseases, medical complications (hemorrhage, preeclampsia, placenta previa etc.) and/or cognitive disorders; contraindication for physical exercise (eg: having severe other musculoskeletal disease, high risk pregnancies, balance deficiencies); and taking part in other exercises or physiotherapy programs.
This study was approved by the University Medical Ethics Comitee. Prior to the study, patients were given information about the risks and benefits of the treatment protocol in order to decide whether or not they wish to undergo a treatment. The voluntary subjects provided written informed consent. The Declaration of Helsinki was strictly followed throughout the study.
Study design
A double blind, randomized controlled trial with 1:1 allocation was performed to examine the effectiveness of Pilates exercise on pregnancy-related LBP. The subjects were randomized by an independent person into either the Pilates exercise group (
Study flow diagram.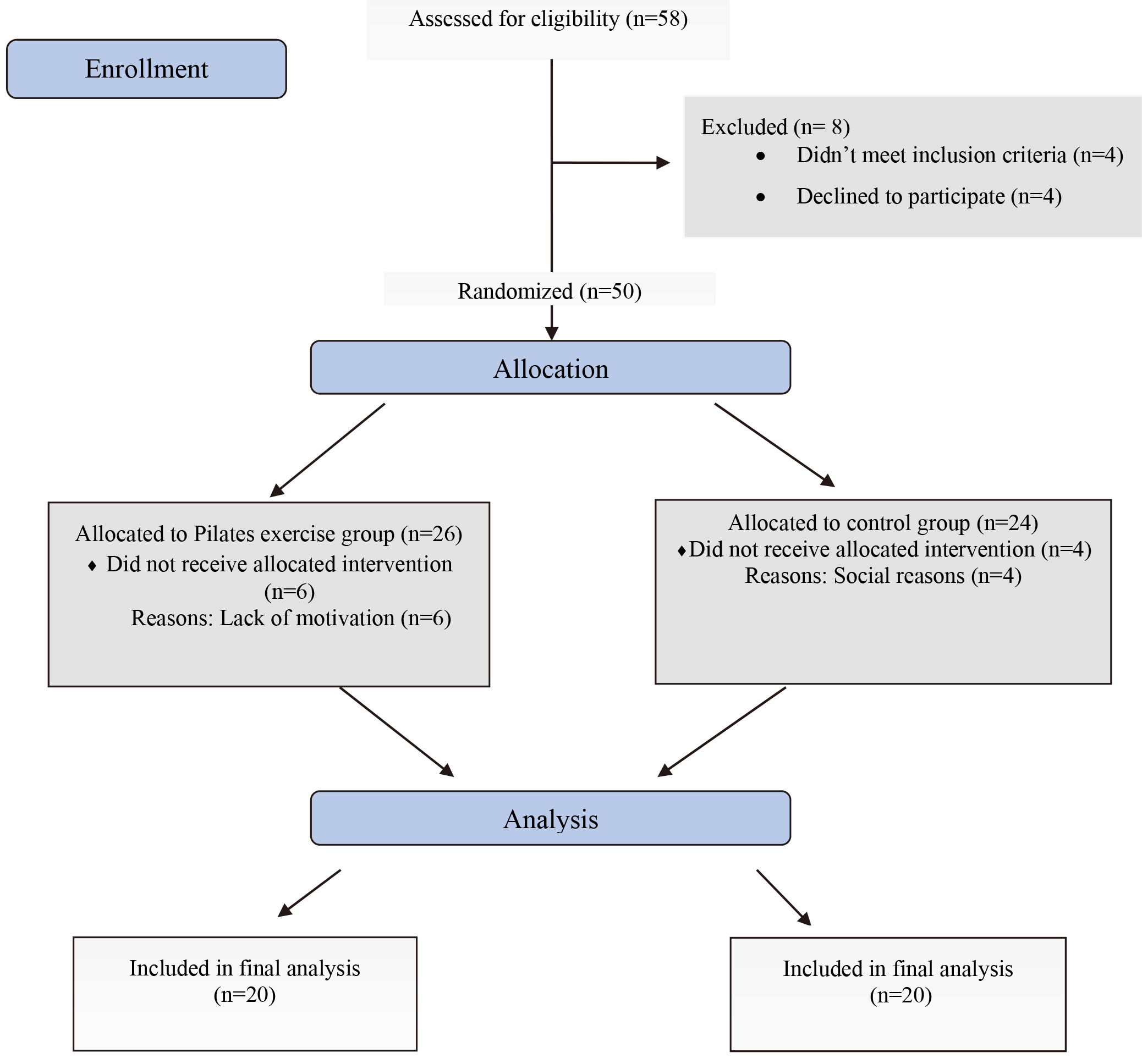
Clinical Pilates exercise program.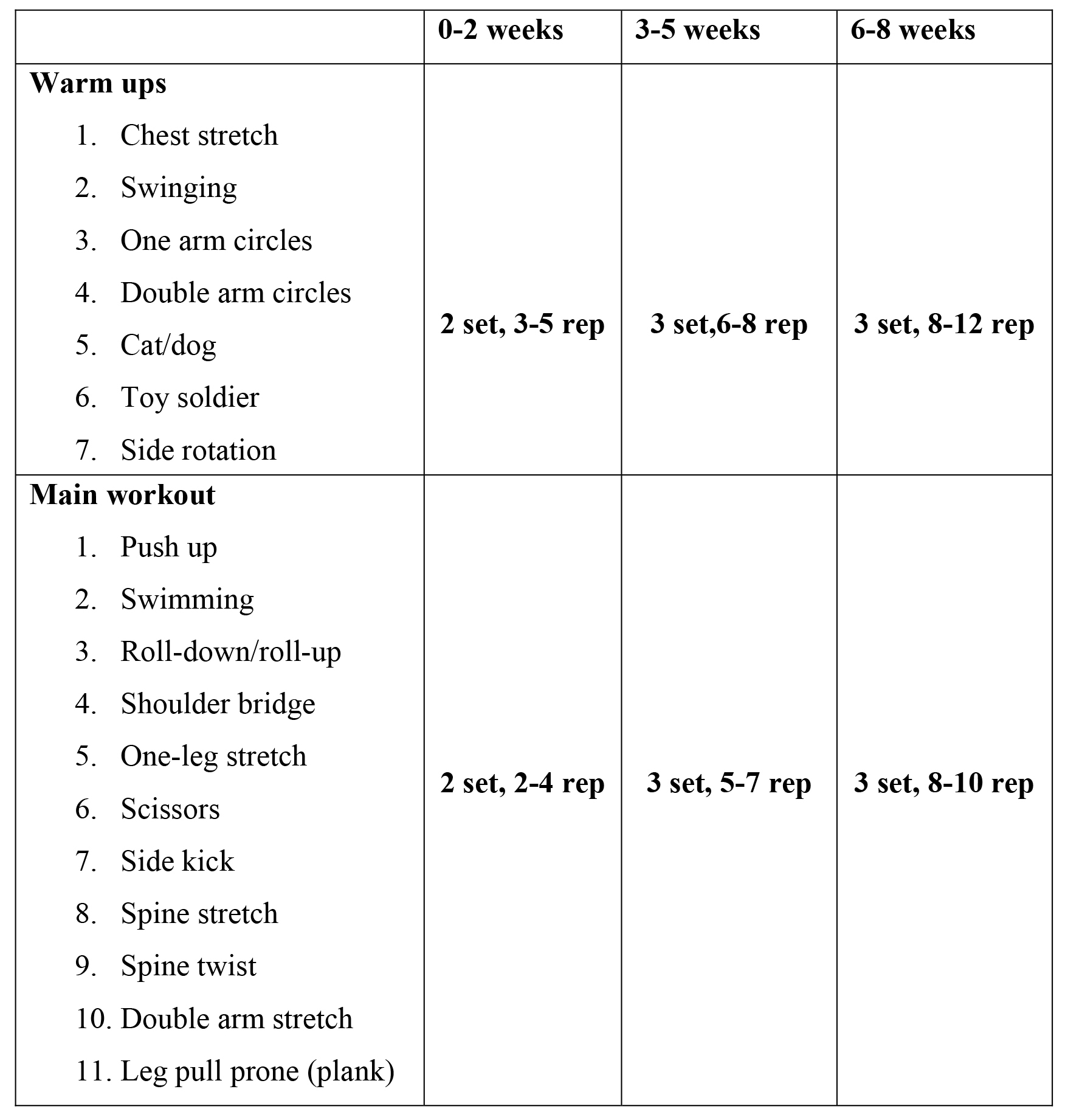
Participants in the control group followed regular prenatal care consisting of routine medical and nursing care and were given education consisting of ergonomic information about activities that exacerbate LBP during daily living and optimal lifting techniques, sitting, standing and sleeping postures. They were not given any exercise prescription.
Women in the Pilates group were additionally given clinical Pilates exercises. Clinical Pilates exercises were performed individually two times a week for eight weeks under the supervision of a physical therapist who was a certified Pilates instructor. Women started the clinical Pilates exercise program between weeks 22–24 of their pregnancy and terminated it between weeks 30–32. The pregnant women in the Pilates exercise group performed a program that included a warm-up and a main work out session. The total exercise program consisted of 18 different clinical Pilates exercises designed to stretch, strengthen and balance the body and lasted for 60–70 minute each session (Fig. 2). The exercises were taught with appropriate breathing techniques. Subjects were given information about adverse events including dyspnea, dizziness, headache, muscle soreness, weakness, calf pain or swelling. When they had any adverse events, they were asked to stop the exercise.
Baseline demographic and clinical characteristics was recorded at admission.
Baseline characteristics of the subjects
Baseline characteristics of the subjects
SD: Standard deviation. There were no statistical differences among the groups (
Disability
The present study used the valid and reliable Turkish version of the Oswestry Low Back Disability Questionnaire to determine functional disability due to back pain [20]. The questionnaire has 10 subgroups and is scored between 0 and 5. Subgroups of this questionnaire address the severity of pain, lifting and carrying, walking, sitting, standing, sleep, sexual life, traveling and social life. The total score of the questionnaire ranges between 0–50, with higher total scores indicating higher functional disability due to back pain [21].
Pain
Pain intensity was measured using the Visual Analog Scale (VAS). VAS is a single-item scale comprised of a horizontal line, 10 cm (100 mm) in length, anchored by two verbal descriptors extremes: “no pain at all” and “my pain is as bad as it could possibly be”. Using a ruler, the score was determined by measuring the distance (mm) on the 10 cm line between the “no pain” anchor and the patient’s mark, providing a range of scores from 0–100. A higher score indicates greater pain intensity [22].
Secondary outcomes
Health-related quality of life
The transcultural adaptation version of the Nottingham Health Profile (NHP) was used to assess health-related quality of life [23]. The NHP is a general quality of life questionnaire designed to measure perceived health problems and the extent to which these problems affect normal daily activities. The survey has a total of 38 questions consisting of six sub-sections: lack of energy (3 items), pain (8 items), emotional reaction (9 items), sleep disturbance (5 items), social isolation (5 items), and physical mobility (8 items). The questions are answered as “yes” or “no” and the best score taken in the sub-sections is 0 and the worst score is 100 [23].
Lumbopelvic stabilization assessment
Lumbopelvic stabilization was evaluated by a pressure biofeedback unit (Stabilizer Pressure Biofeedback Unit, Chattanooga Group Inc., Hixson, TN, USA). The pregnant women were positioned in crook lying position and the pressure cell was placed under the lumbar spine and inflated to the baseline pressure of 40 mm Hg. The women were instructed to perform abdominal hollowing without moving their spine or pelvis, and to hold the contraction for 10 seconds monitored by using a digital watch. The change in pressure during abdominal hollowing was repeated three times and the mean of all the measurements were recorded [24, 25, 26].
Statistical analysis
Data was analyzed with the SPSS package (version 17.0). Mean and standard deviations of the values were calculated for each variable. A normal distribution of data was assessed by means of the Kolmogorov-Smirnov test, and normal distribution was not detected. Baseline features were compared between groups using the Mann-Whitney U test. Within-group differences were assessed with the Wilcoxon test. The statistical analysis was conducted at a 95% confidence level. A
Baseline values of outcome measurements
Baseline values of outcome measurements
SD: Standard deviation, ES: Effect Size. There were no statistical differences among the groups (
The disability level, quality of life and lumbopelvic stabilization scores between the groups
LBDQ: Low Back Disability Questionnaire, VAS: Visual Analog Scale. SD: Standard deviation,
This study was reported using CONSORT guidelines. Fifty-eight pregnant women were screened. Four women did not meet the inclusion criteria and four women were declined to participate. In total, 50 subjects (median of maternal age: 23 week) were randomly assigned to one of the two groups. Six women in the Pilates group and four women in the control group did not recieve allocated intervention. Twenty subjects in the Pilates exercise group and 20 subjects in the control group participated in the final measurements. There were no differences in the baseline demographic and clinical characteristics (Table 1). Outcome measures were also similar between the groups at baseline (Table 2).
Primary outcomes
Disability
The Oswestry Low Back Disability Questionnaire scores were significantly improved in the Pilates exercise groups after the eight week training period (
Pain
The VAS score was significantly improved in the Pilates exercises group at the end of the training period (
Secondary outcomes
Quality of life
Based on the quality of life measures using the NHP, sleep (
Change in lumbopelvic stabilization
The change in pressure during abdominal hollowing increased significantly in the Pilates exercises group after the eight week experimental period (
Discussion
The present study results demonstrated that clinical Pilates exercises are effective in reducing pain and functional disability, improving lumbopelvic stabilization strength and increasing the quality of life in pregnant women with LBP. To the best of our knowledge, this is the first study that shows the effectiveness of clinical Pilates exercise on disability, quality of life and lumbopelvic stabilization in women with pregnancy-related LBP.
Postural changes and hormonal fluctuations in pregnancy negatively affect muscle activation and strength by inducing biomechanical changes in the muscles that provide lumbopelvic stability. Previous studies demonstrated that subjects with LBP have an impaired ability to sustain the lumbopelvic stabilisation [26, 27, 28]. Therefore the accurate assesment of lumbopelvic stabilization is important not only to detect the vulnaribility to lumbar pain but also to select the appropriate exercise programme.
It has been reported that Pilates exercises increase the activation of transversus abdominis, diaphragm, multifidus and pelvic floor muscles that affect the local stability system, thus reducing joint laxity [17, 19, 29]. Similarly, the present study results also shows that clinical Pilates exercises specific to pregnancy increase the strength of lumbopelvic stabilization in pregnant women when compared to regular care.
Disability due to LBP is a major problem in pregnancy and can be treated through controversial non-pharmacological interventions such as use of exercise methods, ergonomic modifications and manual therapy methods due to the limited use of pharmacological agents in pregnancy [12]. Oktaviani et al. reported that Pilates is effective in reducing LBP in pregnant women [19]. Similarly, the present study also showed that an eight week clinical Pilates exercise program is more effective than regular prenatal care with ergonomic education in reducing LBP and disability in pregnant women. Previous studies showed that weak muscle function in the lumbar and pelvic region is associated with severe pain and disability in pregnancy [30]. Therefore, Pilates exercises may ensure biomechanical healing resulting from increased lumbopelvic stabilization.
Although the use of Pilates-based stabilization exercises for reducing lumbar-pelvic pain has become widespread, no study was found that investigated the effects of this program on pregnancy-induced pain and quality of life in pregnant women. The present study examined the effects of an eight week Pilates exercise program on the quality of life in pregnant women. Study findings show that the program improved sub-parameters of quality of life such as physical mobility and sleep pattern in the experimental group, but did not generate similar results in the control group. Progression of pregnancy leads to significant limitations in physical activity. However, these activities can be limited pathologically in pregnant women with LBP [31, 32]. Pregnant women often avoid doing these activities or develop abnormal movement patterns to relieve or prevent the pain. Both decrease in physical activity and abnormal movement patterns result in a vicious cycle leading to muscle dysfunction causing more pain and disability [33]. An increase in motor control achieved by increasing the stability of the lumbopelvic region eliminates this cycle by reducing muscle dysfunction [26]. The present study results indicate an improvement in physical mobility via Pilates exercises and suggests that Pilates exercises reduce pain and disability, increasing mobility and decreasing activity limitations.
Studies report that pain particularly during the later weeks of pregnancy usually increases overnight and causes sleep problems [12]. The present study shows that Pilates exercises with ergonomic education performed by pregnant women with pregnancy-induced LBP is more effective than regular prenatal care with ergonomic training, on the sleep sub-parameter of the quality of life. Altough, according to the statistical analysis, the
The absence of long-term follow-up is a limitation of this study. However, changes in the bodies of pregnant women in transition from the second to third trimester affects their pain, functional disability levels, muscle strength and quality of life. Therefore, both the exercises and the follow-up period in this study were terminated before the trimester transition. Thus, the differences that may occur when the pregnancy progresses were minimized. Due to the challenges of obtaining approval from the pregnant women for repeating the assessment during the last trimester is the another appropriate reason for this limitation. We had problems in continuing the Pilates program because pregnant women had a higher tendency to to be sedentary. This adherence problem is another limitation of the study.
No side effect was observed during and after the exercise sessions in the study. This indicates that Pilates exercises can be used safely without putting mothers and their babies at risk during the pregnancy.
Conclusion
In conclusion, Pilates exercises are considered effective in increasing the strength of lumbopelvic stabilization, reducing pain and disability, improving physical mobility and solving sleep problems in pregnant women with LBP. This program can improve musculoskeletal problems related to pregnancy and provide a more active and comfortable pregnancy. Clinical Pilates exercises are recommended as an effective and safe method for the management of pregnancy-induced LBP.
Footnotes
Conflict of interest
The authors have no conflicts of interest to declare.