
Abstract
BACKGROUND:
Various cupping sizes of cupping therapy have been used in managing musculoskeletal conditions; however, the effect of cupping sizes on skin blood flow (SBF) responses is largely unknown.
OBJECTIVE:
The objective of this study was to compare the effect of three cupping sizes of cupping therapy on SBF responses.
METHODS:
Laser Doppler flowmetry (LDF) was used to measure SBF on the triceps in 12 healthy participants in this repeated measures study. Three cup sizes (35, 40 and 45 mm in diameter) were blinded to the participants and were tested at
RESULTS:
All three sizes of cupping cups resulted in a significant increase in peak SBF (
CONCLUSIONS:
Our results show that all three cup sizes can significantly increase SBF. The 45 mm cup is more effective in increasing SBF compared to the 35 mm cup.
Introduction
Cupping therapy refers to a technique that uses a cup to suck on the skin with localized negative pressure, and is a popular therapy in Asia, Central Europe, and Africa [1]. Cupping therapy has been used in the management of pain, fatigue, respiratory and gastroenterological disorders [1]. Cupping therapy can be applied using either a plastic, bamboo, or glass cup to create suction using a mechanical or electrical pump on the skin over an acupoint, painful area, or reflex zone [2]. Despite its popularity, the effectiveness of cupping therapy remains inconclusive. More research is needed to establish the clinical effectiveness and comparative efficacy of cupping therapy [3, 4].
Various theories have been proposed to explain the potential mechanisms of cupping therapy, including restoration of sympathovagal balances by stimulating the peripheral nervous system, modulation of the immune system by regulating immunoglobulins and hemoglobin, and improvement of blood flow to the skin, muscle and underlying tissues [5, 6]. Regarding the benefit of cupping therapy on improving musculoskeletal conditions, the increase of blood flow to the skin and muscle may be a major factor. Cupping therapy could dilate local blood vessels of the skin by stimulating the endothelial cells to release vasodilators, including nitric oxide [5, 6, 7]. Although previous studies have demonstrated that cupping therapy could increase skin blood flow (SBF) [5, 6, 7], there is insufficient evidence to establish the dose-response relationship of cupping therapy on SBF responses.
The effectiveness of cupping therapy is dependent on several factors, including cupping pressure, cupping duration and cupping size [6]. Among these factors, the effect of cupping size of cupping therapy is least studied. Clinically, the diameter of the cup used in cupping therapy may range from 35 to 50 mm [8]. Clinicians usually select the cup size based on a principle that a smaller cup should be used when the disease is deeper; and a larger cup should be used when the disease is close to the skin. However, there is no scientific evidence to support this principle [8, 9]. Tham et al. used a finite element model to demonstrate that a cup of 65 mm diameter could cause a higher stress at the interface between the fat and muscle layers than the 35 mm and 50 mm cups [10]. They recommended that the cup should be as large as the anatomical area can accommodate where cupping therapy is applied. Hendriks et al. used a suction device with different sizes of suction cups to measure the mechanical response (i.e. elasticity and stiffness) of the skin using the optical coherence tomography and ultrasound [11]. Their results showed that a larger cup could lead to a larger displacement inside the cup of the skin [11]. In the literature [8, 9, 10, 11], these conflicting results may contribute to the inconclusive evidence of cupping therapy on managing musculoskeletal conditions.
The skin microcirculation has emerged as a representative vascular network to examine the microcirculatory regulations [12, 13, 14], and may provide insight of the effect of cupping sizes of cupping therapy on SBF responses. Various noninvasive, optical devices have been used to assess skin microcirculation, including laser Doppler flowmetry (LDF) and laser speckle contrast imaging (LSCI). LDF is a noninvasive technology that allows continuous, real-time assessments of SBF. This technology could be useful to study the effect of cupping therapy on SBF responses. Up to date, only a few studies investigated the effect of cupping therapy on SBF responses, and no studies investigated the effect of cup sizes of cupping therapy on SBF responses [15, 16, 17]. Huang et al. compared the efficacy of traditional fire cupping and modern standardized negative pressure devices on SBF responses [16]. Wei et al. observed the effect of cupping therapy on SBF at different locations of back in healthy people [15]. Yang et al. compared the effect of pulsating and static cupping therapy on SBF [17]. These studies have improved the understanding of the effect of cupping therapy on SBF responses. However, the effect of cupping size of cupping therapy on SBF responses remains largely unknown.
The objective of this study was to investigate the effect of cupping sizes of cupping therapy on the magnitude of SBF responses. We hypothesized that a larger cup could result in a larger SBF response compared to a smaller cup when cupping therapy is applied. To the best of our knowledge, this is the first study that investigates the effect of cupping sizes of cupping therapy on SBF responses.
Methods
A repeated measures design was used in this study. The order of three cup sizes (i.e. 35, 40, 45 mm in inner diameter) was randomly assigned to the research participant and the counterbalanced design was implemented to minimize the carry-over effect. The randomization method was implemented through the pre-determined order of cupping sizes for the first six research participants (i.e. 35-40-45, 35-45-40, 40-35-45, 40-45-35, 45-35-40, and 45-40-35) and was then repeated for the next six research participants.
Participants
The inclusion criteria included the age between 18 and 35 years. The participant was informed that there would be red marks on the triceps after cupping therapy and was presented pictures of athletes with cupping marks on the shoulders. The participant needed to acknowledge that he/she was aware of cupping marks after cupping therapy. The exclusion criteria included cardiovascular, neurological, metabolic or musculoskeletal diseases or taking any medication that may affect previously mentioned systems. The sample size was estimated to be at least 9 research participants based on the assumption of a large effect size, alpha level at 0.05, power at 0.8 and 3 repeated measurements. In this study, we used a counterbalanced study design for 3 repeated measures (35, 40, and 45 mm); thus, a sample size needs to be a multiple of 6. Based on the sample size estimation (i.e. at least nine participants) and counterbalanced design (a multiple of 6 participants), the sample size of 12 participants was chosen. Each research participant signed the informed consent approved by the Institutional Review Board of the University of Illinois at Urbana-Champaign (#20334).
Instrumentation
Laser Doppler flowmetry (PeriFlux 5000 and Probe 455, Perimed, Las Vegas, NV, USA) was used to measure SBF. The LDF device delivered a low-power beam (2 mW) of laser light (780 nm wavelength) to the skin over the triceps of the dominant side. The negative pressure was applied by a standard electric cupping device (Powerpress Pro, Neomedic, Chatsworth, CA, USA). The negative pressure device was able to apply the negative pressure at the specific pressure between 0 and
Cupping parameters
Three sizes of cupping cups were tested in this study, including: 35, 40 and 45 mm in inner diameter. The rim width of the cup was 8 mm that was sufficient not causing discomfort to the skin. Thus, the outer diameter of three cups were 43, 48, and 53 mm, respectively. These cup sizes was selected based on the common cup sizes of clinical practice [8]. According to Tham et al., the cupping size should be as large as the anatomical area can accommodate [10]. In this study, the triceps muscle was the interested area and the largest cup size could be used was about 45 mm in inner diameter (in this case, 53 mm in outer diameter).
The negative pressure was selected at 300 mmHg. The negative pressures between 225 and 375 mmHg are commonly used in cupping therapy [18]. The middle range of the preferred negative pressure was selected. The cupping duration was selected at 5 minutes. It is usually recommended that the duration of cupping therapy is between 5 and 20 minutes [19]. Among these durations, 5 minutes of cupping therapy was most commonly used.
Experimental procedures
Room temperature was maintained at 24
Data analysis
SBF response after cupping therapy was characterized by the reactive hyperemic response. Three parameters, including peak hyperemia (peak SBF in perfusion unit), total hyperemia (total SBF in perfusion unit), and recovery time (in seconds) were calculated [21, 22]. These hyperemic responses could be used to quantify the effect of cupping size of cupping therapy on SBF responses. Peak SBF was defined as the maximum blood flow after cupping therapy and was recommended as an indicator of shear stress in the vascular wall [21, 23]. Total SBF was defined as the total blood flow integrated over the response period. Recovery time was defined as the time needed for blood flow to return to the baseline [21]. The SBF values after cupping therapy were expressed as a ratio (times) of the mean of 10 minutes SBF before cupping therapy in each participant (normalization method) [24, 25]. The normality (normal distribution of collected data) was examined using the Shapiro-Wilk test. The one-way Analysis of variance (ANOVA) with repeated measures was used to compare the SBF response between the 3 sizes (35, 40 and 45 mm). The significance level was set at
Results
Twelve healthy, young individuals (2 males and 10 females) were recruited for this study. The demographic data were: age 25.3
Illustration of skin blood flow before (blue lines showing a relatively steady line around 10 perfusion units) and after (grey lines showing a hyperemic response) cupping therapy with three cupping sizes in a research participant. The figure also shows peak skin blood flow and recovery time. (A) Skin blood flow before and after cupping therapy with the 45 mm cup. Skin blood flow exhibits a reactive hyperemic response after cupping therapy. (B) Skin blood flow before and after cupping therapy with the 40 mm cup. (C) Skin blood flow before and after cupping therapy with the 35 mm cup. 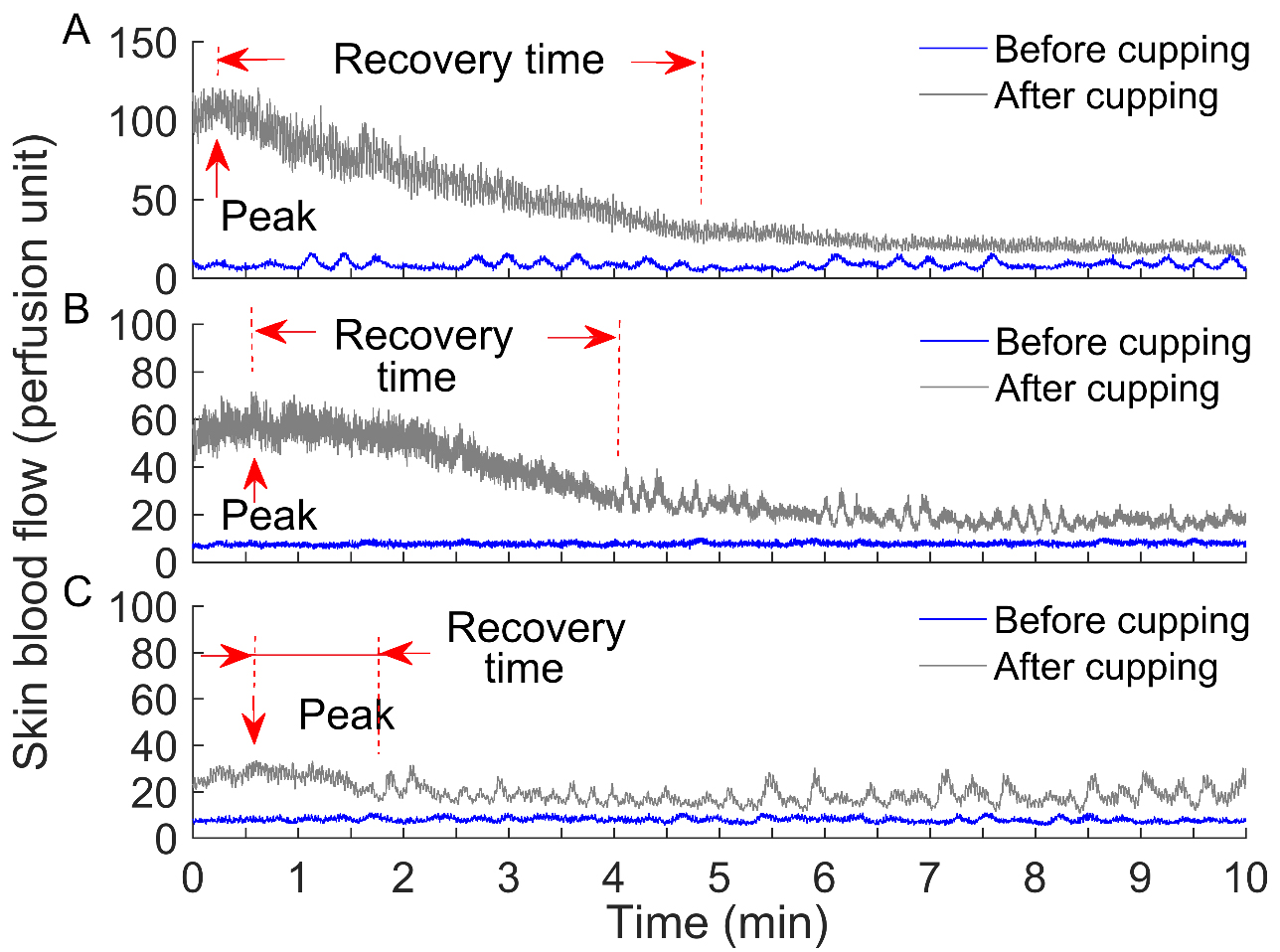
Typical examples of SBF in response to three cupping sizes of cupping therapy of tan individual are shown in Fig. 1. Cupping therapy with the 45 mm and 40 mm cups causes a significant increase in SBF. Cupping therapy with the 30 mm cup also significantly increases SBF but at a much smaller degree compared to the 45 mm cup (Fig. 1).
The normality tests showed that all data were normal distributed (
Peak SBF of all three cupping cups of cupping therapy resulted in a significant increase compared to baseline SBF (
Comparison of different cupping sizes (45, 40, and 35 mm) of cupping therapy on (A) peak skin blood flow, (B) total skin blood flow and (C) recovery time of reactive hyperemic response to cupping therapy. Data are presented as mean 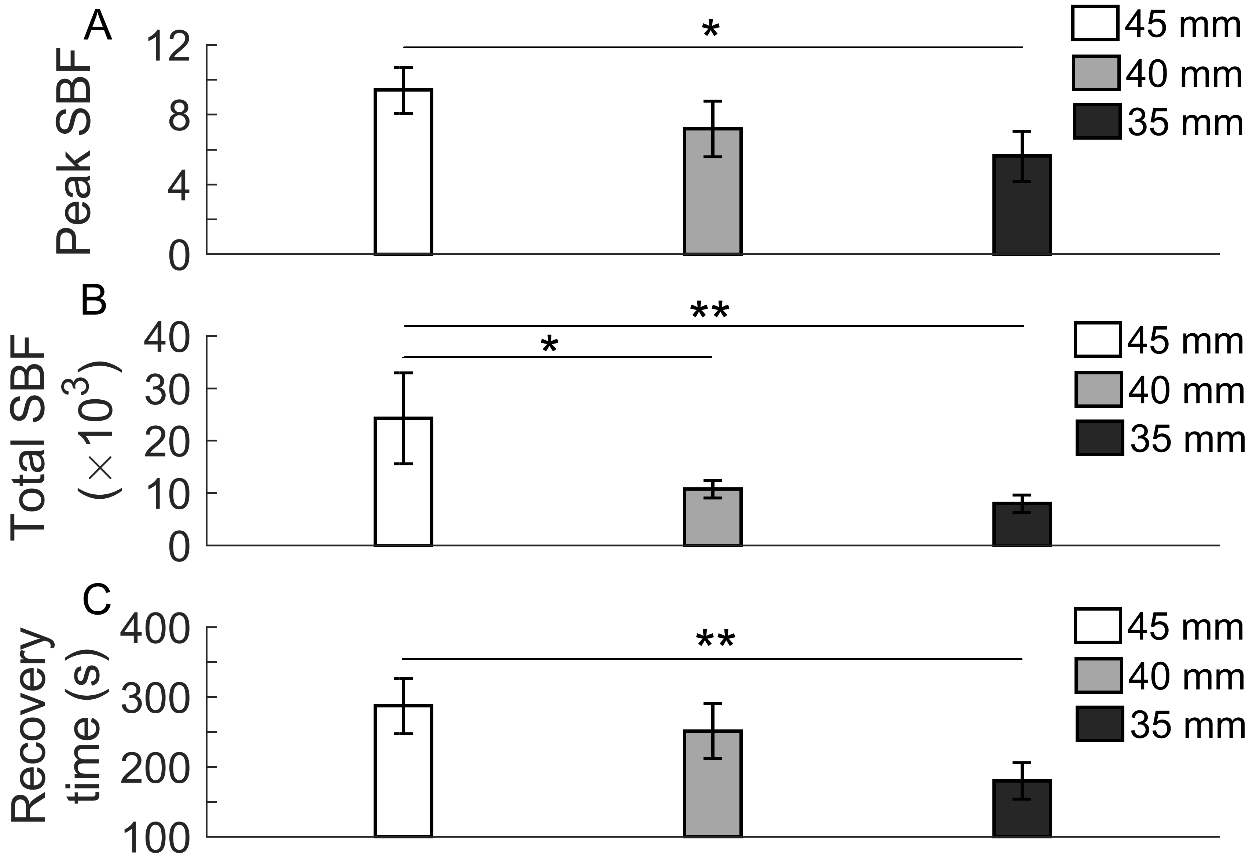
Total SBF of all three cupping cups of cupping therapy resulted in a significant increase compared to the baseline SBF (
Recovery time after cupping therapy with the 45 mm cup (287.46
This study demonstrates that cupping therapy with three cupping sizes resulted in a significant increase in peak SBF, total SBF, and recovery time of reactive hyperemia on the triceps area; and cupping therapy with the 45 mm cup was more effective on increasing SBF compared to the 35 mm cup. The current finding supports the concept that the largest cup where the treated area can accommodate should be used for improving SBF. To the best of our knowledge, this is the first study investigating the effect of different cupping sizes of cupping therapy on SBF responses. Our finding may contribute to the guideline of selection of cupping sizes to manage musculoskeletal conditions in clinical practice of cupping therapy.
Previous studies have demonstrated an increase in SBF after cupping therapy [5, 6, 15, 17]. The method used in these previous studies was the average of SBF responses [5, 6, 15, 17] that may not fully characterize time-series SBF changes [21, 23]. In this study, we further demonstrated that such an increase in SBF after cupping therapy follows the pattern of a reactive hyperemic response. Reactive hyperemia occurs after the occlusion of blood vessels and shows a transient increase in SBF followed with a slow decrease in SBF [21, 23, 26]. Typical reactive hyperemia responses are reported after the removal of compressive force (e.g. blood pressure cuff). However, reactive hyperemia has not been used to describe SBF changes after cupping therapy (i.e. tensile force caused by negative pressure) [2, 27]. To the best of our knowledge, this is the first study using reactive hyperemia to investigate the effect of cupping therapy on SBF responses. Our results demonstrated that peak SBF, total SBF and recovery time of reactive hyperemia vary according to the applied “intensity” of cupping therapy, in our case, different sizes of cupping cups. The use of reactive hyperemia may overcome the temporal variations of SBF measured at different time points.
Reactive hyperemia is a complex hemodynamic response of the vasculature. The physiological benefit of reactive hyperemia is to accelerate the delivery of oxygen to tissues as well as the removal of metabolic byproducts after a period of ischemia (i.e. cupping induced ischemia of the skin) [22]. According to the principle of reactive hyperemia, a larger hyperemic response of the same person indicates a larger ischemic stress imposing on the skin and underlying soft tissue [21, 28]. Thus, if a 45 mm cup caused a larger reactive hyperemic response, it may imply that the 45 mm cup caused a larger ischemia to the skin inside the cupping cup. According to the Pressure
Our study demonstrated that cupping therapy with the 45 mm cup increased more than 9 folds compared to its baseline SBF, and cupping therapy with the 35 mm cup increased more than 5 folds compared to its baseline SBF. Our results showed that cupping therapy with the 45 mm cup is more effective on increasing SBF compared to the 35 mm cup. Although the difference between the 45 mm and 35 mm cups may seem small, the effects on increasing SBF are significantly different (9 folds vs 5 folds). The cupping therapy applied in this study was a low-intensity cupping dose (
As previously discussed, there are no previous studies comparing the effect of cup sizes on SBF responses. The degree of an increase in SBF after different cupping sizes of cupping therapy could only be compared to other stimuli. Our result is consistent with the study conducted by Moore et al. who demonstrated that a wider blood pressure cuff is more effective on occluding blood flow [30]. Crenshaw et al. suggested that blood pressure cuff wider than the traditional cuff would be more effective over a wider range of limb circumference. They recommended using a wider cuff as possible for extremity surgery to minimize soft tissue damage [31].
The establishment of relative efficacy of cupping therapy remains a clinical priority [3, 4]. In this study, we attempted to use reactive hyperemic responses to compare the effect of cupping sizes of cupping therapy and confirmed that reactive hyperemia could be a promising assessment to optimize the dose-response relationship of cupping sizes on SBF responses. Traditionally, researchers would average the SBF values to determine clinical efficacy. However, reactive hyperemia responses (peak SBF, total SBF and recovery time) provide more information that would be especially important in patients with various vascular diseases. With more studies using our methods, the selection of cupping sizes and cupping pressure and duration could be optimized for improving clinical efficacy. The use of a 30-minute washout period in this study was sufficient because the baseline skin blood flow of three conditions in all research participants was not significantly different. The research participant was in a supine position during cupping therapy. The response of SBF in this position may be different from the upright position, especially the sympathovagal balance issue. Also, the sample size was sufficient due to relatively homogeneous and significant responses in SBF response to various cupping sizes.
Our study has limitations. First, we measured SBF and did not measure muscle blood flow. Although muscle blood flow seems more relevant, the technology used to measure muscle blood flow may limit its use in this study due to longer measuring time. Laser Doppler technology is particularly useful in measuring reactive hyperemic responses. The laser Doppler device used in this study provides a sampling frequency at 32 Hz. Future studies may use advanced technologies to measure muscle blood flow responses under different cupping sizes of cupping therapy. Second, we recruited healthy participants for this study. Future studies need to validate our study in patients with musculoskeletal impairments to determine the effectiveness of cupping therapy.
Conclusion
Our results showed that the cupping size of cupping therapy at the same negative pressure (
Footnotes
Conflict of interest
None of the authors have any conflicts of interest to declare.