
Abstract
BACKGROUND:
Low back pain (LBP) is a common musculoskeletal problem, which commonly affects balance. Sustained natural apophyseal glide (SNAG) is a successful treatment approach for LPB. However, its influence on balance problems has not been studied before.
OBJECTIVE:
To investigate the immediate effect of SNAG on postural stability and pain in individuals with flexion-dominant chronic low back pain (FCLBP).
METHODS:
Randomized placebo-controlled trial in which 64 participants with FCLBP were randomly allocated into two groups (SNAG and sham). SNAG group (
RESULTS:
There were statistical significance and high effect size (ES) in favor of the SNAG group regarding OSI, APSI, and pain (
CONCLUSION:
Lumbar SNAG produces an immediate improvement in postural stability and pain in individuals with FCLBP.
Introduction
Low back pain (LBP) is the pain located between the last rib and the gluteal region which may refer to the posterior thigh [1]. LBP is a common musculoskeletal complaint worldwide. Approximately 80% of the population experiences pain at some point in life. This dysfunction has a major impact on patients’ lifestyle and socioeconomic status [2] as well as the health insurance systems [3].
Recently, different classifications have been presented for LBP. One of these classifications is called the Multi-Dimensional Classification System (MDCS) which has been presented in 2006 by O’Sullivan [4]. According to the MDCS, the condition has been sorted according to the direction of the most painful movement into flexion, extension, or global LBP. The recent trends toward the sub-classification of LBP address the variations in clinical presentations of the individuals and allow better and case-sensitive designation of rehabilitation program [5].
Experiencing pain in the low back has been associated with a decline in physiologic functions such as balance. The increased displacement of the center of pressure while standing upright, in addition to the greater medial-lateral postural sway were among the proposed causes of balance disturbances associated with LBP [6, 7].
Other studies found that LBP individuals using less hip strategy and more activity of calf muscle to maintain standing posture [8, 9]. Rosa and colleagues have reported a higher risk of falling in elderly individuals with chronic LBP. They found that the LBP group was associated with higher postural sway, longer reaction time, and lower quadriceps strength compared to the healthy group [8]. Similar results have been obtained earlier by Leveille et al. [10]. Using less hip strategy might be attributed to the disturbed proprioceptive input from the lumbar spine [11].
Balance can be assessed using clinical tests and laboratory devices. The laboratory devices have the advantage of the ability to assess different aspects of balance such as sensory integration, limits of stability, and postural stability. The Postural Stability Test assesses the subject’s ability to maintain the center of balance, measures how much the patient’s position deviates from the center and reports the average deviation (stability index). Therefore, a low score is more desirable than a high score [12].
Manual therapies such as sustained natural apophyseal glide (SNAG) are among the physical therapy interventions commonly used to relieve pain [13], increase mobility [14], and improve function [15] in LBP. SNAG was described first by Brian Mulligan [16] and performed by asking the recipient to assume a weight-bearing position then performing the painful movement while the therapist applying a mobilizing force parallel to the plane of the facet joint [17]. According to Mulligan, SNAG-related improvements were the result of the correction of the mechanical fault inside the facet joints. Despite the lack of adequate scientific research supporting this explanation, it has been adopted by many researchers [15, 16, 18, 19].
Due to the unclear mechanism of SNAG, few researchers tried to explore its various effects on body systems and functions; Moutzouri and colleagues applied lumbar SNAG to healthy individuals and compared its effects to sham treatment. The lower extremity skin conductance was measured as an indicator of sympathetic activity. This study failed to record any significant differences between SNAG and sham [20]. In 2015, Hidalgo investigated the immediate and short-term effects of SNAG on two kinematic algorithms for trunk movement during rest and flexion posture in individuals with Chronic LBP, this placebo-controlled trial reported improvement in one of the two algorithms in favor of the SNAG group [13]. A third study was conducted in 2017 by Hussien et al. to investigate the effect of adding lumbar SNAG to a standard LBP treatment on the lumbar repositioning error as an indicator of lumbar proprioception. This study demonstrated statistically significant improvement in lumbar proprioception in favor of the SNAG group [21].
The authors hypothesized that the application of lumbar SNAG may have immediate beneficial effects on balance in addition to pain in individuals with FCLBP. The purpose of this study is to investigate the immediate effect of lumbar SNAG on postural stability and pain in individuals presenting with FCLBP.
Methods and materials
SNAG for the lumbar spine from standing position.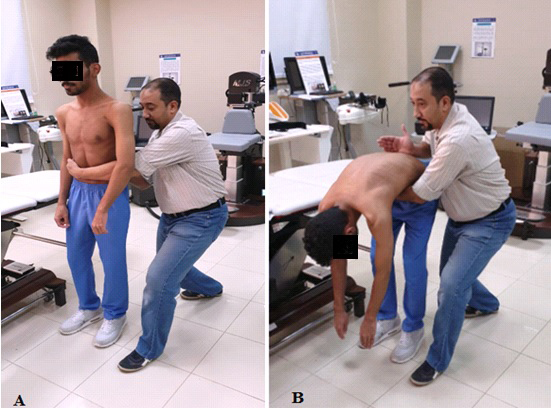
A randomized single-blinded placebo-controlled trial design was conducted. This trial followed the recommendations of the CONSORT 2010 (Consolidated Standards of Reporting Trials) statement [22], approved by the faculty of physical therapy ethical committee board (P.T.REC/ 012/001895), and was registered on the Pan-African Clinical Trial Registry (PACTR) under no. PACTR201811496048196.
Sixty-four individuals diagnosed with FCLBP were recruited from the newly-referred individuals with LBP at the outpatient clinic, MUST University, Giza, Egypt. The individuals were selected after clinical examination, which consisted of history taking, palpation of the painful lumbar spinous processes, and assessing pain with different postures. Inclusion criteria were (1) subjects from both genders; (2) aged between 19 and 45 years; (3) LBP that increases, more than 14 mm [23], with flexion postures; (4) Persistent or intermittent for 3 months or more [21].
Exclusive criteria were individuals who previously received manual therapy including SNAG techniques, radicular pain, disk lesions, spinal stenosis, arthritis, degenerative joint diseases, facet joint disease, and visual or vestibular impairments. Individuals who experienced an increase in pain or decreased ROM after the application of SNAG were considered ineligible and were excluded from the study [13, 21].
Sample size
The sample size was estimated using the G*power 3.0.10 software (Heinrich Heine University Düsseldorf, Düsseldorf, Germany) depending on the OSI scores. A pilot study, which included 10 participants (who did not participate in the main study), underwent a similar intervention protocol. The mean
Interventions
Both Mulligan lumbar SNAG and Sham techniques were performed by an experienced physical therapist. SNAG was applied over the symptomatic lumbar spinous processes. The subject was assuming a stride standing position while the therapist was standing behind and toward the left side of the treated subject. The therapist placed the ulnar side of his right hand just under the spinous process of the target lumbar level while the other hand was used to support the waist of the subject. The therapist applied the mobilizing force in a cephalic direction (parallel to the lumbar facet joint plane) and asked the subject to lean forward until the limit of pain. Upon reaching the end range, the flexed position was maintained for a few seconds then the subject was asked to return to the starting position (Fig. 1). The mobilizing force and its relative direction were maintained throughout the movement. Each symptomatic level received 4 sets of 6 repetitions per single session as recommended in guidelines [17].
Regarding sham SNAG, the subject and therapist positions, and the procedures were the same as performed with the real SNAG (Fig. 1). The exceptions were that the therapist’s hand was just touching the patient lumbar spine and did not provide the needed mobilizing force or its correct direction. The subject was instructed to perform 4 sets of 6 repetitions of trunk flexion to the pain limit per every symptomatic level [24].
Outcomes measures
Overall, anteroposterior, and mediolateral stability Indices (OSI, APSI, MLSI respectively) were the main outcome measures, while pain intensity score was the secondary outcome.
The assessor interviewed the recruited individuals; during this interview, an initial screening, demographic data recording (Table 1), a standardized clinical examination, which consisted of history taking, palpation, and assessing response during flexion and extension postures [13], and the eligibility test for SNAG were performed. Individuals who met the inclusion criteria signed a consent form and were given a code number referring to their group allocation.
Physical characteristics of patients in both groups
Physical characteristics of patients in both groups
SNAG, sustained natural apophyseal glide; SD, Standard deviation;
During the interview, the assessor asked the individuals to rate their current level of pain on a non-numerical visual analog scale (VAS). This non-numerical form of VAS was used to avoid the clustering of the scores around a preferred number [25]. After having the patient check the current pain on the VAS, a plastic-made ruler was used to measure the distance from the left end of the line (the zero point) to the mark placed by the patient. The cutoff points for the VAS were 0-4 mm for no pain, 5–44 mm for mild pain, 45–74 mm for moderate pain, and 75–100 mm for severe pain [26]. The VAS has been considered valid and reliable in reporting musculoskeletal pain [27].
The three postural stability indices were tested using the Biodex balance system (Biodex Medical Systems Inc., Shirley, New York, USA). This instrument consists of a movable balance foot platform. This platform contains sensors and allows up to 20
Initially, the assessor entered the individual’s demographics data and the detailed parameters of the tests. The following test details were used; two-leg stance, moderate difficulty (level 5), 30 s trial duration, 10 s rest between trials, and one familiarization trial was allowed before each actual test [12].
According to the individual’s characteristics, the Biodex software determined the appropriate feet and heels coordinates of the platform in which the individual’s feet should be placed. Individuals were instructed to remove footwear and stand on the platform according to the predetermined coordinates. The height of the Biodex screen and the handle were adjusted to allow easy access by the subject [12]. With eyes open, and upon releasing the platform, the individual was instructed to avoid grasping the handles and try to maintain his/her center of gravity (the cursor on the screen) in a centered position on the screen by minimizing postural sway as much as possible. Five seconds were provided to the subject to adjust and prepare before the test starts. If the subject lost his balance, a momentary touch of the handle was allowed to regain balance and continue. If the individual failed to regain balance quickly, the trial was deleted. OSI, APSI, and MLSI were calculated, recorded, and printed.
Assessment of stability indices using the Biodex device.
Permuted blocks with variable sizes [4, 6] were used to randomly allocate the participants into either the SNAG or Sham Group. The allocation ratio was 1:1. The order of randomization was generated using the online randomization service at
Mixed model ANOVA results for the main effect of time, intervention, and the interaction effect
Mixed model ANOVA results for the main effect of time, intervention, and the interaction effect
Flowchart of the study.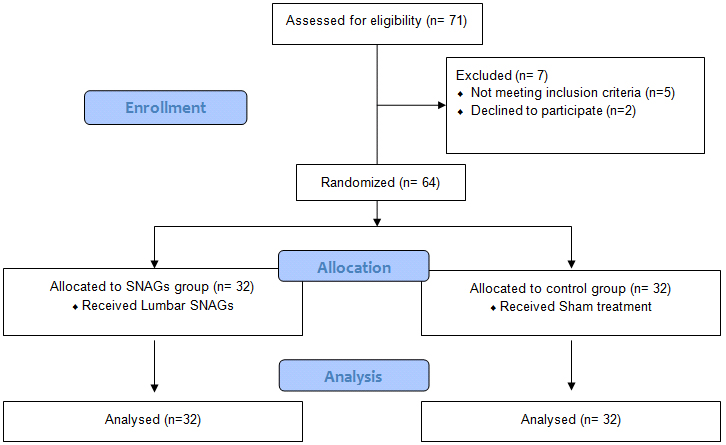
Each eligible subject was given a code number indicating the allocation sequence. The assessor received the code number, through a phone call with the senior author, and wrote it down on the subject’s sheet. Before starting the treatment session, the therapist received the interpretation of the code through another phone call to the senior author so that the appropriate intervention can be administered. This way the assessor and the individuals were kept blind throughout the study while the therapist was unaware of the allocation sequence but was not blind to the intervention arms.
Statistical methods
Statistical package of social science (SPSS) 20 was used to analyze all data. Normal distribution of data was performed using Shapiro-Wilk test. Mixed-model ANOVA was performed to study the main effect of each independent factor (interventions and time) as well as the main interaction effect (interventions* time). Post-hoc tests using the Bonferroni corrections were carried out for the subsequent multiple comparisons. Alfa level was set to (
Results
The participants’ flow is presented in Fig. 3. The characteristics of both groups were similar at baseline (Table 1). The recruitment process was conducted in the period between May and June 2018 and was terminated after the enrollment of the required sample size.
There was a significant main effect of time (
Between-groups comparison demonstrated statistically significant improvement with high effect size regarding OSI, APSI, and pain intensity in favor of the SNAG group. MLSI failed to reach a statistical significance value (
Means
SD and data for all outcome measurements for between SNAG and Sham groups
Means
VAS, visual analog scale; OSI, over-all stability index; APSI, anterioposterior stability index, MLSI, mediolateral stability index,
Means
SD, Standard deviation;
Cohen’s
The within-group comparison revealed that all outcome measures were improved after the intervention in the SNAG group (
Up to the authors’ knowledge, the present study is the first to study the effect of lumbar SNAG on postural stability in individuals with FCLBP. The majority of previous studies have adopted the mechanical explanation, which was originally described by Brian Mulligan where pain [15], range of motion [24, 32], and function [13, 15] were the main outcome measures.
The current results showed that the majority of the outcomes showed either high (OSI APSI, pain) or medium (MLSI) effect size in favor of the SNAG group. These findings suggest that SNAG might have a clinically important effect on balance and pain when applied to individuals with FCLBP.
The improvement in the postural stability indices demonstrated after using SNAG may be explained by the stimulation of facet joints and surrounding mechanoreceptors-rich structures which may improve proprioception and enhance sensory-motor control. Moreover, stimulation of these receptors can reduce pain, through the gate mechanism [33], and normalize the function of the spinal muscles, and consequently improves muscular participation in balance control.
Other mechanisms might explain the improvements demonstrated in both groups such as the controlled and skillful handling of an experienced therapist that may contribute to decreasing the patient fear to move and increase assurance. This psychological behavior may improve patient response. The multiple trunk flexion movements performed by the individuals in both groups might improve lumbar spine mobility, increase the extensibility of tight lumbar extensors, and enhance normal muscular participation in postural mechanisms.
Our observations regarding pain improvement were per previous studies [13, 15, 21]. On the other hand, Konstantinou et al. concluded that lumbar SNAG does not affect the intensity of pain. However, this finding might be affected by the nature of the adopted crossover design of this study. In the crossover design, the effect of the first intervention may remain and affect the results of the second intervention especially when both treatments were performed in the same session [18].
The results of the current study might be used in clinical practice. Individuals with FCLBP who demonstrate balance abnormalities might benefit from lumbar SNAG. However, caution should be implemented because of the small number of the studied sample.
The limitations of the current study can be summarized in the following points. First, the authors focused only on studying postural stability indices; to obtain a better view, future studies should include the other aspects of balance. Second, a single therapist conducted the intervention for both groups. This might affect the results yet, it eliminates the influence of interrater variability. Third, this study focused on the immediate effect of SNAG. This design was implemented not to deprive the individuals in the control group of receiving treatment. Future studies should implement a follow-up protocol.
Conclusion
Lumbar SNAG produces an immediate improvement in postural stability and pain scores in individuals with FCLBP.
Footnotes
Conflict of interest
None to report.