
Abstract
BACKGROUND:
The unilateral biportal endoscopic (UBE) technique has been widely used in spine surgery. At present, a traditional rigid working channel is available for the UBE system. A metal semicircular canal is located in the working channel. However, due to the metal material of the working channel, arthroscopy and instruments are constrained from moving in UBE surgery. Additionally, an assistant is needed during the procedure to hold the traditional working channel.
OBJECTIVE:
For simplicity of operation and convenient movement of the arthroscopy and instrument, we describe a new method for establishing operative channels in UBE surgery.
METHODS:
We retrospectively reviewed 50 patients who underwent unilateral biportal endoscopic discectomy (UBED) from February 2020 to August 2020 via our new method. The Oswestry Disability Index (ODI) and visual analogue scale (VAS) score were measured preoperatively and 1 month, 3 months, 6 months and 12 months postoperatively. Statistical comparisons were made using analysis of covariance and paired t tests.
RESULTS:
The VAS scores for back pain at the five time points were 5.20
CONCLUSION:
This study demonstrates the technical feasibility, safety, and efficacy of modified channel establishment in UBE surgery.
Keywords
Introduction
Unilateral biportal endoscopic (UBE) surgery has undergone rapid development in recent years because of its unique advantages. Compared with UBE surgery, conventional open spinal fusion surgery and minimally invasive transforaminal interbody fusion increase the risk of spinal structures injury, such as paraspinal muscles, bone, and ligaments [1, 2, 3, 4, 5]. Different from the single-channel endoscopic spine surgery system, UBE surgery allows direct central and foraminal neural decompression to be achieved, similar to conventional open decompression discectomy, through sufficiently safe procedures involving a magnified clear view and free handling of instruments [6, 7, 8]. However, certain limitations, such as a steep learning curve, orientation under endoscopic vision, and capability to sufficiently decompress the spinal canal, limit the use of fully endoscopic techniques [9]. The surgical anatomy in biportal endoscopic spinal surgery is similar to that in conventional lumbar microdiscectomy, which is familiar to spinal surgeons converting from microsurgery to biportal surgery. The magnification of pathologic lesions via a 4-mm biportal endoscope and the provision of a clean operative field through continuous saline irrigation allow visualization of anatomical details during surgery. Nearly all microsurgical instruments, such as high-speed drills, pituitary forceps, and Kerrison punches, can also be utilized in biportal endoscopic surgery. Therefore, biportal endoscopic surgery is considered a minimally invasive technique with a shorter learning curve than any other minimally invasive spinal surgery technique, including fully endoscopic surgery.
At present, a traditional rigid working channel is available for the biportal endoscopic system. A metal semicircular canal was located in the working channel. However, due to the metal material of the working channel, the scope is constrained from moving. At the same time, an assistant is used for stabilizing the working channel. For convenient movement of the scope and instrument, minimally invasive surgery needs to be performed in a cavity filled with irrigated saline between the lamina, flavum and paraspinal muscles. The clarity of visualization under the endoscope is affected by the size of the cavity and the water flow rate [6].
Here, we attempted to establish a modified working channel to easily expand and clarify the operational field in UBE surgery. The purpose of this study was to introduce UBE decompression surgery for degenerative disc disease using the modified working channel technique and to present preliminary clinical results.
Materials and methods
Ethical consideration
This retrospective study was approved by the research ethics committee of the Second Affiliated Hospital of Soochow University (JD-HG-2021-07). The study was conducted in accordance with the Declaration of Helsinki.
Patient selection
A total of 50 patients underwent UBED from February 2020 to August 2020. One patient was excluded due to a history of spinal surgery, and one was lost to follow-up. Finally, 50 patients were included in this study. For an accurate diagnosis, X-ray, CT, and MRI were performed in all patients. Every patient underwent single-segment UBED. All patients were treated by single experienced orthopaedic surgeons. The inclusion criteria were as follows: (1) single-level lumbar disc herniation or lumbar spinal stenosis; (2) preoperative symptoms of lower extremity radiating pain or LBP (VAS
Procedures for modified channel establishment. (A) Localization of needles. (B) Insertion of the infusion strap through the cranial incision (viewing portal) and exit of the strap from the caudal incision (working portal) below the muscle layer. (C) Fixation of a Y-shaped drainage device to the patient’s skin with sutures to form a stable water flow channel at the caudal incision. (D) Blurring of the surgical field of view when the water flow ceased, followed by clearance of the surgical field of view upon the assistant tightening the infusion strap to expand the interstitial space.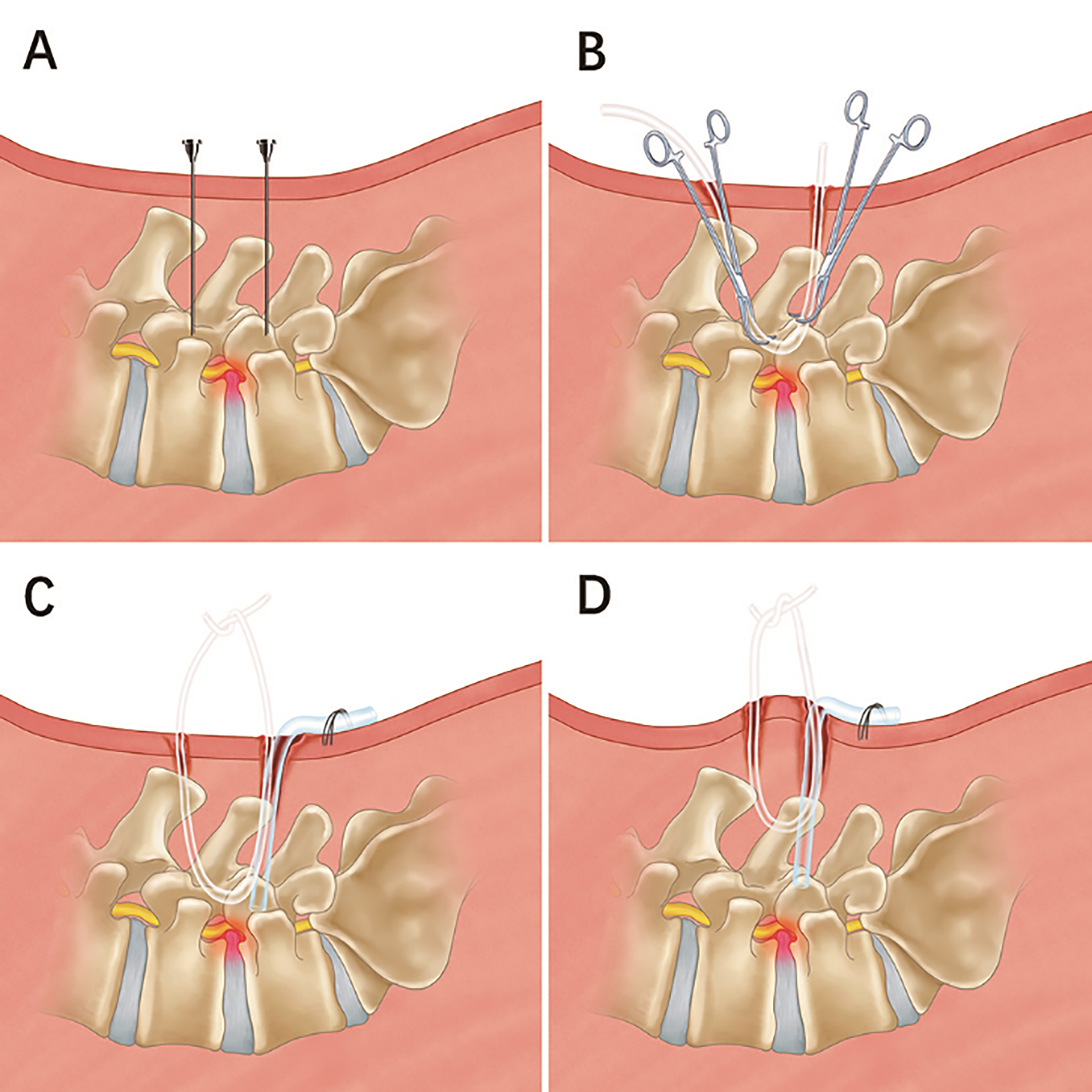
Raw materials and physical graph of the modified channel. (A) Infusion tube. (B) Infusion strap made by infusion tube. (C) Suction apparatus tube. (D) Y-shaped drainage device made of suction apparatus tube. (E) Physical graph of the modified channel. ❳ Fixation of a Y-shaped drainage device to the patient’s skin with sutures. ❬ Infusion strap was knotted above the skin.
The process of water flow pressure measurement. (A) Measurement when the water flow is open. ❬ Pressure measurement devices. (B) Measurement when the water flow is closed with 5 mm forceps. ❬ Pressure measurement devices. ❳ 5-mm forceps. (C) Measurement when we tightened the infusion strap to make the outflow open again. ❬ Pressure measurement devices. ❳ 5-mm forceps. ❮ Vascular clamp tightened the infusion strap. (D) The needle tip has reached the epidural space. ❬ The needle tip. (E) The position of the zero point. (F) Pressure signals were displayed on the monitor.
The process of modified channel establishment is shown on the example of L4–5 lumbar disc herniation. A patient was placed in the prone position over the radiolucent chest frame in a flexed position. The surgeon stood on the left side of the patient. Two standard entry points were marked 1 cm above and below the disc space on an anteroposterior view. The cranial mark was assigned to the viewing portal, while the caudal mark was assigned to the working portal. The surgeon inserted the needles at two incision marks. Then, C-arm fluoroscopy was performed to ensure that the tips of the needles were in the ideal position (Fig. 1A). After withdrawing the needles, the skin and lumbodorsal fascia were incised in turn according to the incision marks. Two periosteal strippers were inserted into the incision vertically until they reached the surface of the lamina. To preliminarily prepare the surgical field, the two periosteal strippers were used to strip soft tissue from the laminar surface until they met. Two vascular forceps were then used: one was inserted from the cranial incision (viewing portal), and the other was inserted from the caudal incision (working portal). The infusion strap was inserted through the cranial incision, passed below the muscle layer and exited from the caudal incision (Fig. 1B). A Y-shaped drainage device, which was made of suction apparatus tube and infusion tube, was fixed to the patient’s skin with sutures to form a stable water flow channel at the caudal incision (Fig. 1C). In the case of water flow stoppage or bleeding in the surgical field, the assistant tightened the infusion strap to expand the space between the lamina and paraspinal muscles (Fig. 1D). Raw materials and a physical graph of the modified channel are illustrated and described in Fig. 2. The other procedures for UBED were the same as described by Choi et al. [10]. The same surgical team performed all operations. The surgical team included 3 surgeons, anaesthesiologists, nurses and other observers.
Water flow pressure evaluation
We performed pressure measurementsafter the discectomy. In the modified channel group, water flow pressure was performed with outflow open (Fig. 3A), outflow closed with 5 mm forceps (Fig. 3B) and tightening of the infusion strap to make outflow open again (Fig. 3C). In the traditional channel group, water flow pressure was only performed with the outflow open. Water flow pressure was measured by a disposable pressure transducer and showed a similar tendency to the method of invasive measurement of arterial pressure. The epidural needle was connected to a disposable pressure transducer. Under endoscopic vision, we confirmed that the needle tip had reached the epidural space (Fig. 3D). A disposable pressure transducer had its transducers zeroed at the external auditory meatus, which is in the same horizontal plane as the eye and occipital prominence (Fig. 3E). Pressure signals were displayed on the monitor (Fig. 3F).
Data collection and complication evaluation
After the operation and before discharge from the hospital, all patients were re-examined with MRI and CT scans. The images after surgery showed sufficient decompression of the spinal cord and excluded acute complications. Clinical data were obtained for evaluation, including demographic data, operative data, and clinical outcome data. The operative data included the modified channel establishment time, biportal endoscopic time, postoperative hospital stay and incidence of complications. The modified channel establishment time was estimated from the moment of skin incision to the time of Y-shaped drainage device fixation to the patient’s skin. The biportal endoscopic time was calculated from the first entry of the endoscope to the last extraction. Clinical outcomes were assessed using VAS scores for back pain and leg pain, as well as the ODI. The ODI and VAS score were measured preoperatively and 1 month, 3 months, 6 months and 12 months postoperatively. Evaluation of postoperative complications included revision, dura tear, symptomatic epidural haematoma and infection.
Statistical analysis
All statistical analyses were performed using SPSS version 20.0 (SPSS, Inc., Chicago, IL, USA). The Shapiro-Wilk test was used to evaluate the distribution of the collected data. Normally distributed continuous variables are presented as the mean and standard deviation (SD), whereas nonnormally distributed variables are presented as the median and interquartile range (IQR). Categorical variables are presented as numbers and percentages (%). Repeated measures one-way analysis of variance (RM-ANOVA) was performed to compare the pre- and postoperative VAS scores and ODIs. Post hoc pairwise comparisons (paired
Characteristics and demographic data
Characteristics and demographic data
BMI: body mass index.
Characteristics and demographic data
A total of 50 patients were included in this study, consisting of 34 males (68.00%) and 16 females (32.00%). The average age of the patients included in this study was 34.48
Operative data and complications
The mean channel establishment time was 4.56
Operative data and complications
Operative data and complications
Clinical outcomes data
ODI, Oswestry Disability Index; BP-VAS, visual analogue scale for back pain; LP-VAS, visual analogue scale for leg pain.
Water flow pressure data. (A) Comparison of water flow pressure in the 2 groups. (B) Water flow pressure of the modified channel in different states.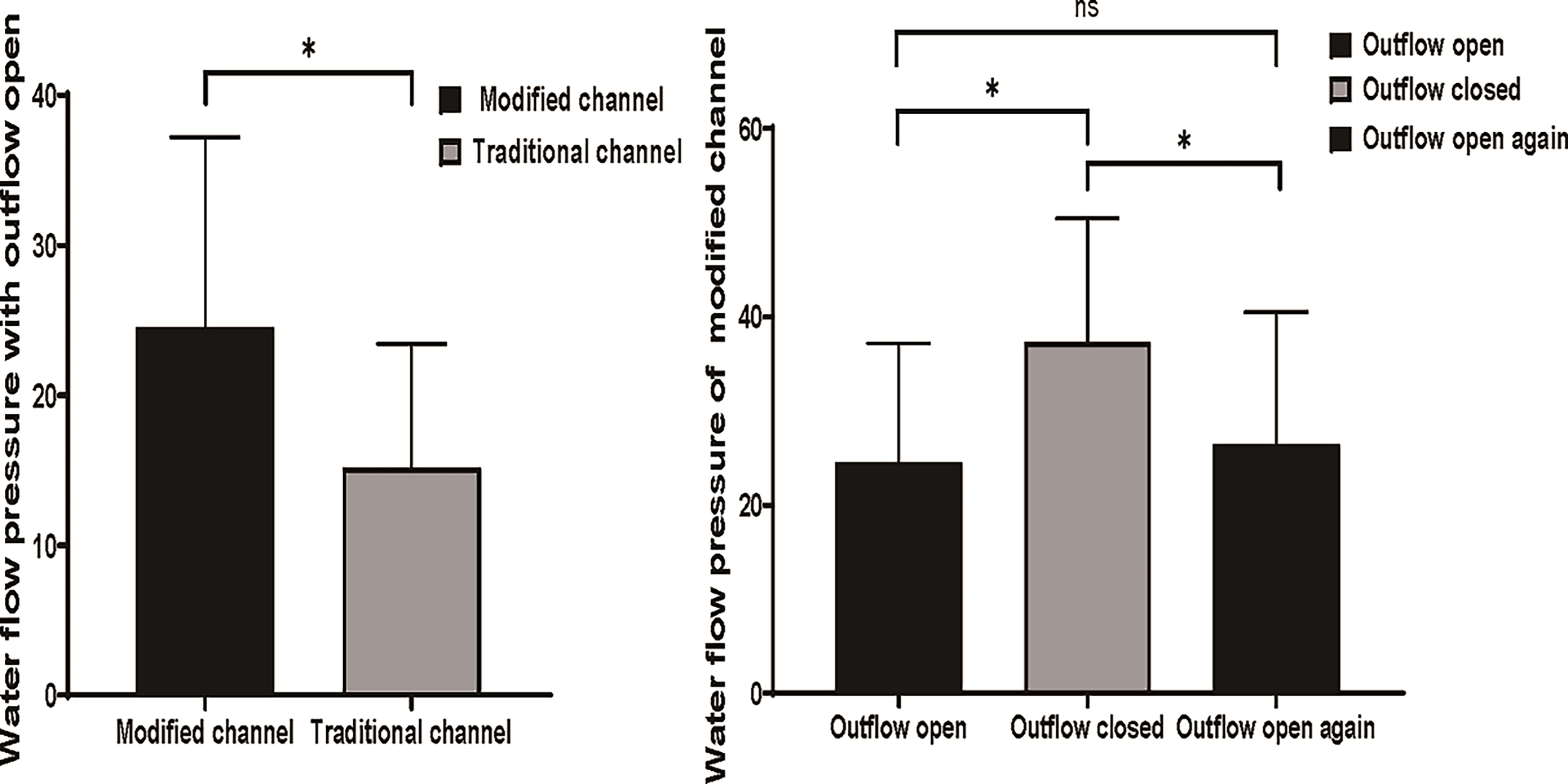
Compared to the traditional channel, the water flow pressure was significantly higher in the modified channel (24.55
Clinical outcomes
The VAS scores for back pain improved from 5.20
Endoscopic view changes. (A, C) The endoscopic view was blurred due to the blockage of water flow. (B, D) After tightening the infusion strap, the endoscopic view again became clear. Ca indicates caudal sides; Cr, cranial sides; L, lateral; M, medial.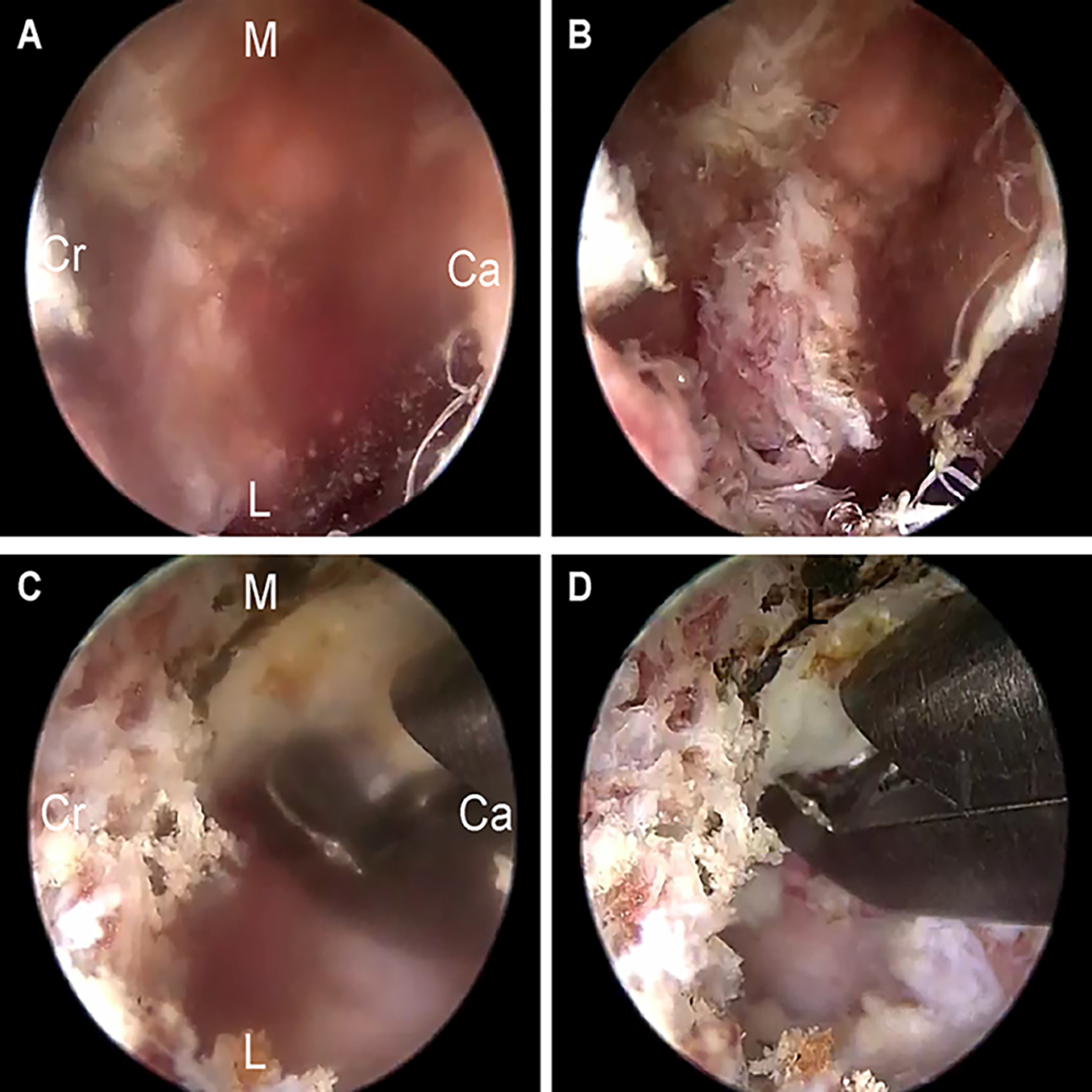
UBE surgery is a widely performed minimally invasive spinal surgery with satisfactory clinical outcomes, such as reduced pain and rapid recovery [11]. Generally, specific instruments are required during conventional percutaneous endoscopic lumbar discectomy surgery, as well as a shallow learning curve and a high rate of complications when applied for the treatment of lumbar spinal stenosis [12]. The endoscopic instruments used in UBE could also be used in other surgeries, such as knee arthroscopy [3], greatly reducing medical expenses. Furthermore, the use of two channels, the viewing portal and the working portal, which are similar to those used in an interlaminar approach, is more in line with the surgical habits of spinal surgeons and allows full exposure of the area requiring decompression. However, there are still some shortcomings of UBE under certain conditions. On the one hand, it requires muscle splitting and shaving of the working space, which may cause bleeding affecting the surgical field and prolong the operative duration. However, laminotomy and foraminoplasty are usually performed in UBE by piezosurgery, and the high-frequency ultrasonication of piezosurgery causes the surgical field to become turbid, increasing the difficulty of the procedure for the surgeon.
Considering these disadvantages of UBE surgery, we designed a simple device for establishing the surgical portals. This device is versatile, allows a sufficient range of motion for surgical instruments and continuous irrigation and is both readily available and relatively inexpensive. Such a device could be easily regulated by assistants, enabling prompt changes in the water flow volume and operating space. Obviously, the convenience of this design is that the surgical space can be temporarily regulated without excessive muscle tissue ablation and the consequent minor damage. Meanwhile, the Y-shaped drainage device applied in our method provides a temporary fulcrum for the working portal, which is conducive to stable operation by the spinal surgeon and reduces the risks associated with equipment slippage.
Our modified channel has the following advantages over previous rigid channels. First, because the arthroscope was made of metal and the view channel was of limited size, the previous rigid channel occupied so much space that there remained no room to allow the arthroscope to function adequately to permit accommodation. Unlike stainless steel or titanium alloy, our drainage device is made from a soft plastic suction tube, which can yield to the moving instruments while providing the stiff support required during surgery, thus increasing the convenience of the operation (Fig. 2). Second, our modified channel is made of an inexpensive material without requiring the purchase of additional equipment. More importantly, such a device could be temporarily fixed to the skin by silk thread without requiring long-term support from a surgical assistant. Finally, in the modified channel, if the water flow ceased, the surgical field of view became blurred (Fig. 5A; Fig. 5C). After tightening the infusion strap to expand the space between the paraspinal muscles and lamina, the surgical field of vision again became clear (Fig. 5B; Fig. 5D). In contrast, rigid channels cannot increase the working space under paraspinal muscles and lamina.
Additionally, we analysed the local water dynamics in UBED surgery. We demonstrated that the pressure of the closed outflow was significantly higher than that of the open outflow. However, after we tightened the infusion strap to make the outflow open again, the pressure returned to that of the outflow open. Therefore, tightening the strap helps to maintain a clear visual field that may be explained at the local water dynamics. Compared with the traditional channel, the modified channel has higher water pressure. This should be because of different materials. Traditional channels are usually made of metallic materials, and modified channels are made of plastic. The hardness of plastic did not perform as well as metal. However, the hardness of the metal was not conducive to intraoperative manipulations. The modified channel can ensure a certain hardness and some plasticity, which facilitates surgical manipulation.
Our study demonstrated that this modified portal design for UBE surgery was a feasible and effective technique for use in the treatment of single-level lumbar degenerative disease, including stenosis and disc herniation. The clinical outcomes of biportal endoscopic decompression at 12 months after surgery confirmed the advantages of UBE. As mentioned above, there were significant improvements in the mean VAS scores for leg pain and back pain, as well as in the ODIs during the follow-up period compared with preoperatively (Table 3). Furthermore, the reported operative time for single-level UBED in the literature ranged from 62.8 to 101.1 min [13, 14, 15]. In our study, the endoscopic operative duration was 71.04 minutes per level, with an average channel establishment time of only 5.20 minutes (Table 2). In fact, the time for establishing a surgical portal notably decreased as experience was gained. This result also means that surgeons could quickly grasp the essentials of channel establishment with short-term training and avoid excessive increases in the operative duration, thereby reducing unnecessary damage to patients.
In addition, compared with the control group, the arthroscope was directly inserted into the viewing portal without any channel. UBE surgery with the modified portal technique also showed less postoperative drainage (data not shown). The drainage tube was once routinely inserted into the operative cavity in the first few patients. However, we found that the amount of postoperative drainage was very small, and the extubation time was only one day after the operation. Therefore, whether the drainage tube needed to be placed was only dependent on the situation during our surgery. This result is not consistent with that of a previous study, which claimed that saline used for irrigation during the operation would infiltrate into the surrounding muscle and leak into the drain after surgery, which might be the reason for the greater drainage volume [16]. This difference may be due to our shorter operative duration, the use of high-definition imaging, and the application of a radiofrequency probe and piezosurgery during the operation, all of which minimized the risk of bleeding in small vessels and cancellous bone. More importantly, the Y-shaped drainage device was conducive to the discharge of saline, thus greatly decreasing the remaining irrigation fluid. We also believe that reducing the need for drainage tube placement would support patient activity in the early postoperative period and the concept of rapid recovery from minimally invasive surgery.
Despite the potential superiority of UBE surgery, signs of muscle oedema were still detected on postoperative magnetic resonance imaging. Nevertheless, the complications were limited to one case of dural tear (2.0%), one case of revision surgery (2.0%), and there were no cases of symptomatic haematoma or infection (Table 2).
Several limitations of the current study should be addressed. First, the retrospective nature of this study produced limitations. Second, the study lacked a control group. Moreover, all surgeries were performed by a single surgeon. The relatively small sample size is another limitation. Moreover, to facilitate a standardized operation, more hydromechanical tests should be performed to confirm the specific changes in the surgical area during use of the modified operative channel. Furthermore, the effect of the irrigation fluid volume on muscle or nerve roots, especially via shear stress, needs to be further studied in detail.
Conclusion
This study demonstrates the technical safety and efficacy of modified channel establishment in UBE surgery. Therefore, for patients who are candidates for UBE surgery, our convenient method for establishing surgical portals is a feasible option.
Funding
This study is sponsored by the National Natural Science Foundation of China (81971036, 82002345, 81902239), the Natural Science Foundation of Jiangsu Province (BK20191169), the Science and Technology Project of Suzhou (KJXW2019011) and the Preliminary Research Project of the Second Affiliated Hospital of Soochow University (SDFEYBS1905).
Supplementary materials
The supplementary figures are available from
Footnotes
Acknowledgments
The authors thank all participants at the Second Affiliated Hospital of Soochow University and acknowledge the support of patients.
Conflict of interest
None of the authors have any conflicts of interest to report.