
Abstract
BACKGROUND:
Due to the influence of spinal and respiratory movements, it is difficult to accurately measure the range of motion of each joint.
OBJECTIVE:
To conduct a three-dimensional (3D) measurement of each joint in the shoulder complex in different postures in the sagittal plane of the upper extremity.
METHODS:
Thirteen healthy adults with no history of shoulder surgery for trauma or chronic pain were enrolled in the present study. The computed tomography (CT) imaging data of the shoulder complex were acquired in four postures via the reconstruction and alignment of 3D images. The angles of the postural changes were measured, and rotation vectors were used for descriptions and statistical analyses.
RESULTS:
There was a statistical difference in the rotation angles between the dominant and non-dominant sides of the sternoclavicular joint when the posture changed from a resting position to a posterior inferior position. During the postural change from a resting position to a horizontal position, the regression coefficient (
CONCLUSION:
The application of the image alignment technique enabled the direct and accurate measurement of the bony structures of the shoulder joint. The helical approach accurately described the scapulohumeral rhythm during 3D motion. There was a scapulohumeral rhythm of the shoulder complex during 3D composite sagittal movement, with different ratios for different joints and postures.
Introduction
The shoulder complex includes the sternum, clavicle, scapula, and humerus; jointly, they form the sternoclavicular joint, acromioclavicular joint, glenohumeral joint, and humeral axillary joint, respectively. The movement of the shoulder is characterized by three-dimensional (3D) rotation and multi-joint composite movement [1, 2, 3, 4]. During the movement of the upper limb, the movement pattern of the above four bones and joints is called the scapulohumeral rhythm. However, since the composite motion of the four joints in the 3D space is influenced by both spinal and respiratory movements, the accurate measurement of the range of motion of each joint is difficult. Technological progress has led to continuous improvements in the techniques available for measuring the rotation angle of the shoulder joint, including X-ray stereogrammetry, non-invasive electromagnetic tracking devices, optical tracking systems, and in vivo bone needle measurements.
In an earlier study, Inman [5] divided the abduction of the upper limb into two phases based on the results of two-dimensional (2D) planimetric measurements from X-ray imaging at 0
The most classical and popular method of describing the 3D rotation of an object is the Euler angle [6]. In 2005, the ISB recommended [7] the application of the Euler angle to describe the 3D rotation of the sternoclavicular, acromioclavicular, humeral glenoid, and humeral axillary joints as well as the order of rotation of the Euler angles and the reference coordinate system of the upper limb joints. However, there are three current problems with this. First, there is no ideal method for measuring the 3D rotation angles of the joints in the shoulder complex accurately, directly, and non-invasively without interference from the movements of respiration and the thoracic spine. Second, during the sagittal movements of the upper limb, the 3D scapulohumeral rhythm needs to be validated. Third, there is no ideal method for accurately representing the 3D rotation of the joints in the shoulder complex that can produce a simple visual representation of the scapulohumeral rhythm.
Van der Helm [8] proposed a standardized plan for recording shoulder motion, stressing that although 3D video recording of the chest and humerus is commonplace, the extensive displacement of bone and skin means there is no effective external marker for clavicular or scapular motion. Anglin [9] also reported that the rotation of the scapula and clavicle is difficult to track using external markers due to extensive movement under the skin. In contrast to skin surface markers, the most realistic and accurate results are obtained by the direct measurement in vivo of the angle between bones.
The hypothesis of the present study is as follows: The use of computed tomography (CT) image alignment facilitates the direct and accurate 3D measurement of each joint in the shoulder complex in different postures in the sagittal plane of the upper limb. Using the rotation vector to describe the 3D motion, the rotation angle can be determined, and the scapulohumeral rhythm in the 3D motion can be evaluated.
The results of this study’s regression analysis indicated that the glenohumeral joint is very important in the motion of each joint of the scapular belt. In the three postural changes, there was a corresponding relationship between the glenohumeral joint and the coronal plane of the upper extremity (
Methods
Study subjects
A total of 13 healthy adults (7 males and 6 females) who were examined in the medical imaging department of Beijing Shijingshan Hospital from April 28, 2019, to May 20, 2019, were included in the present study. Among them were 5 college students, 6 in-service nurses, and 2 in-service doctors. None of the patients had a history of shoulder surgery for trauma or chronic pain. The subjects’ ages ranged from 22 to 42 years, with an average age of 26.5 years. There was no history of trauma. If the visual analog scale score for shoulder pain was 0 within 1 year, it was considered that chronic pain was not present. The patients’ body mass indexes ranged from 18.9 to 39.2, with an average of 24.2. In 2 subjects, the left shoulder was dominant, while in 11 subjects, the right shoulder was dominant.
The inclusion criteria were as follows: 1. healthy adults older than 18 years and younger than 60 years, 2. those who signed an informed consent form for participation in research projects, 3. those who were able to cooperate in completing the actions required in the study, and 4. those who accepted the possible radiation exposure dosages in the present study.
The exclusion criteria were individuals 1. with a history of shoulder trauma or surgery, 2. with a history of chronic pain of the shoulder, 3. who were unable to cooperate in completing the designated actions, 4. who did not accept the possible radiation exposure dosages in the present study, and 5. who did not undergo examinations related to the present study due to personal privacy.
The present study was approved by the Ethics Committee of Beijing Shijingshan Hospital, and all volunteers signed the study’s informed consent form after being fully advised of the study’s procedures, risks, and protocols. In this experiment, healthy volunteers underwent four CT examinations, with the following cumulative radiation dose: minimum value
Image acquisition
The CT scans were conducted using a GE Discovery CT750 HD (General Electric Co, Cincinnati, OH, USA) scanner. The CT scanning parameters were a slicing thickness of 0.625 mm and layer spacing of 0.625 mm. The range of the image was as follows: the lower part was at 2 cm below the plane of the sternal angle, and the upper part was at the end of the acromion of the clavicle, including the part of the proximal humerus above the deltoid ramus, as shown in Fig. 1.
The four posture positions during the CT projection photography. A: The supine resting position. B: The supine position with the upper arm forward extension horizontal position. C: The prone position with the upper arm back and hyperextension position. D: The prone position with the upper arm back and lower overextension position.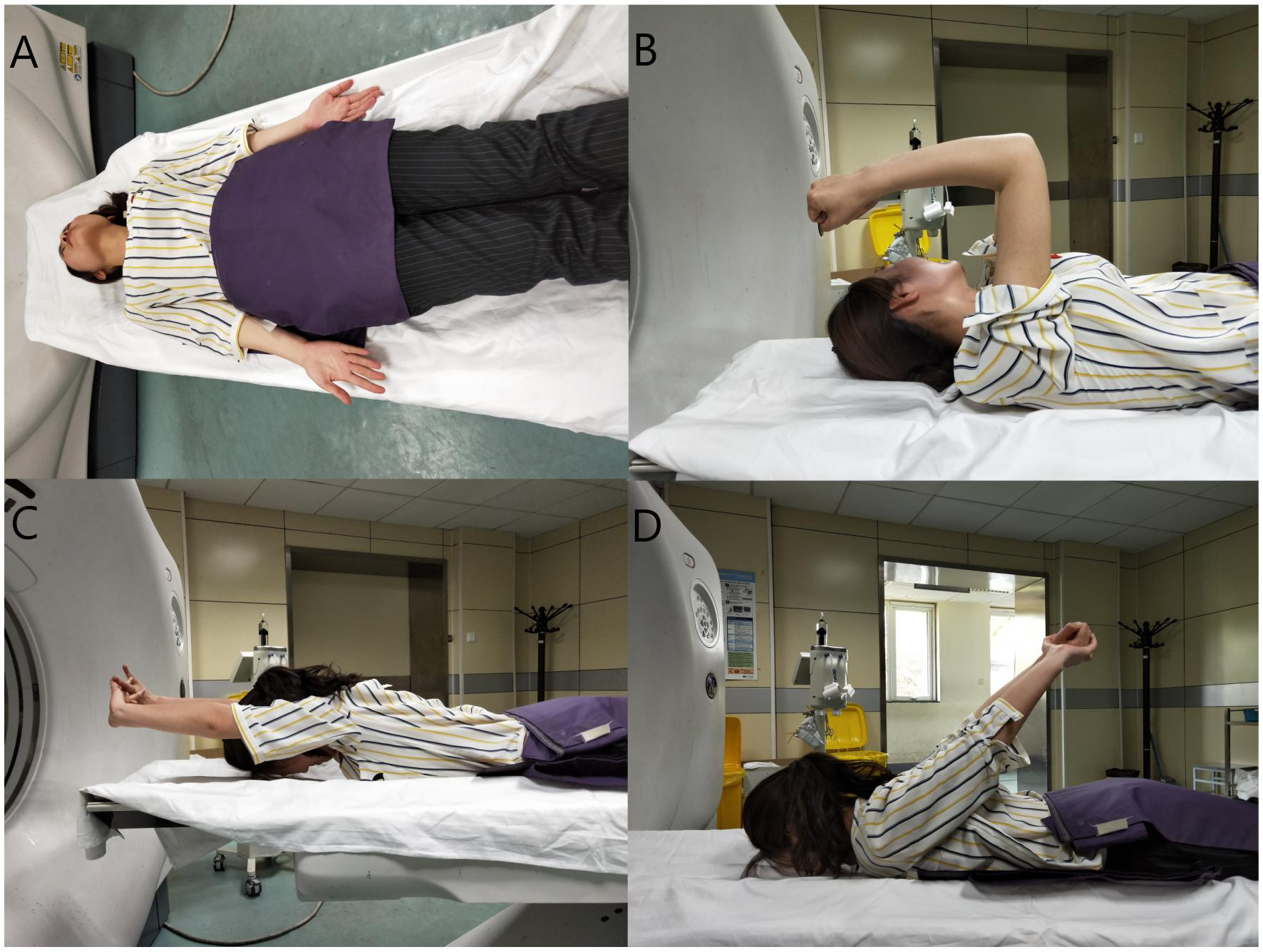
The patients were positioned as follows: A: supine resting position: The palms faced upward on both sides of the body, with the shoulder and elbow joints in a neutral position. B: supine upper limb horizontal position: The shoulder joint was at 90
The image shooting range was from 2 cm below the sternal angle plane to the end of the acromion of the clavicle, including the part above the trochanteric of the deltoid proximal to the humerus.
The following image registration process was followed. First, a 3D complex image was established. The manubrium sternum-clavicle is a 3D complex, and the sternoclavicular joint was studied from four postural perspectives (i.e., the resting, forward horizontal, posterior upper hyperextension, and posterior lower hyperextension positions). The acromioclavicular and glenohumeral joints were also studied in four different postures (the clavicle-scapula and the scapula-humerus are 3D complexes). Finally, humeral movement was studied in four postures (the manubrium sternum-humerus is also a 3D complex).
Second, the reference object and the coordinate system for registration were selected. During the rotation of the sternoclavicular joint, the sternoclavicular complex in the resting position was taken as the reference object, and the virtual space coordinate system of CT 3D reconstruction in this position was taken as the reference coordinate system. During the rotatory motion of the acromioclavicular joint, the 3D image complex of the clavicular bone and scapula in the resting position was taken as the reference object, and the 3D virtual space coordinate system of the CT scan in this position was taken as the reference coordinate system. During the rotation of the glenohumeral joint, the scapulohumeral 3D image complex in the resting position was taken as the reference object, and the virtual space coordinate system of the CT 3D reconstruction in this position was taken as the reference coordinate system. When studying the motion angle of the sagittal plane of the humerus, the glenohumeral 3D image complex in the resting position was taken as the reference object, and the virtual space coordinate system of the CT 3D reconstruction in this position was taken as the reference coordinate system.
Next, the 3D image complex was extracted and exported. The 3D image complexes obtained under three positions of the upper limb (i.e., the forward horizontal, posterior upper, and posterior lower hyperextension positions) were derived separately as independent skins in STL using Mimics Innovation Suite 20.0 (Materialise, Plymouth, MI, USA) software. The registration reference file in the resting position was opened. Registration object: STL format file (In the same virtual 3D space, four postures: i.e., the resting, forward horizontal, posterior upper hyperextension, and posterior lower hyperextension positions).
Finally, the image was registered. In this study, the sternum in the sternoclavicular 3D image complex in the resting position was taken as the registration target during the rotation of the sternoclavicular joint. The virtual space coordinate system of the CT 3D reconstruction was used as the reference coordinate system. Via the visual image registration process, the 3D post-registration images of sternum overlap and different clavicle positions were generated. During the rotational motion of the acromioclavicular joint, the clavicle in the 3D image complex of the clavicle and scapula in the resting position was taken as the registration target, and 3D post-registration images of clavicle overlap and different scapula positions were generated via the visual image registration process. In the 3D image complex of the scapula and humerus in the resting position, the scapula was taken as the registration target during the rotational motion of the glenohumeral joint, and 3D post-registration images of scapula overlap and the different positions of the humerus were generated via visual image registration. In the 3D image complex of the sternum and humerus in the resting position, the sternum was used as the registration target during the sagittal plane movement of the humerus, and 3D post-registration images of sternum overlap and different positions of the humerus were generated using visual image registration.
The raw image data were imported into Mimics 20.0 software to form a 3D image of the four postures and included the sternal stem, clavicle, scapula, and humerus. The bony reference points of the sternum, clavicle, scapula, and humerus recommended by the ISB [7] were used to mark the corresponding positions in the 3D images.
The sternoclavicular joint: Composite 3D images of the sternal stem-clavicle in different postures were acquired and constructed using the sternal stem as the registration object. In the composite 3D image, the sternal stem image in different positions was aligned with the sternal stem image in the supine resting position to form 3D images of different clavicle positions with overlapping sternal images.
The acromioclavicular joint: Composite 3D images of the clavicle-scapula in different postures were acquired and constructed using the clavicle as the registration object. In the composite 3D image, the images of the clavicle in different positions were aligned with the image of the clavicle in the supine resting position to create 3D images of different scapula positions with overlapping clavicle images.
The glenohumeral joint: Composite 3D images of the scapula-humerus in different postures were acquired and constructed using the humerus as the registration object. In the 3D composite image, the image of the scapula in different positions was aligned with the image of the scapula in the supine resting position to form 3D images of different humerus positions with the overlapping scapula images.
The humeral axillary joint: Composite 3D images of the sternal stem-humerus in different postures were acquired and constructed using the sternal stem as the registration object. In the composite 3D image, sternal stem images in different positions were aligned with the sternal stem image in the supine resting position to form 3D images of different humerus positions with the overlapping sternal stem images.
Measurements were obtained of the rotation angles of the position of the 3D images when changing from the resting position to the horizontal position, from the horizontal position to the posterior superior position, and from the resting position to the posterior inferior position relative to the 3D image position of the clavicle in the supine resting position. The results were described in terms of a helical approach, as shown in Fig. 2.
The 3D image composite of the four postures after image alignment. A: The 3D image composite of the sternal stem-clavicle. The sternum is the registration object. B: The 3D image composite of the clavicle-scapula. The clavicle is the registration object. C: The 3D image composite of the scapula-humerus. The scapula is the registration object. D: The 3D image composite of the sternal stem-humerus. The sternal stem is the registration object.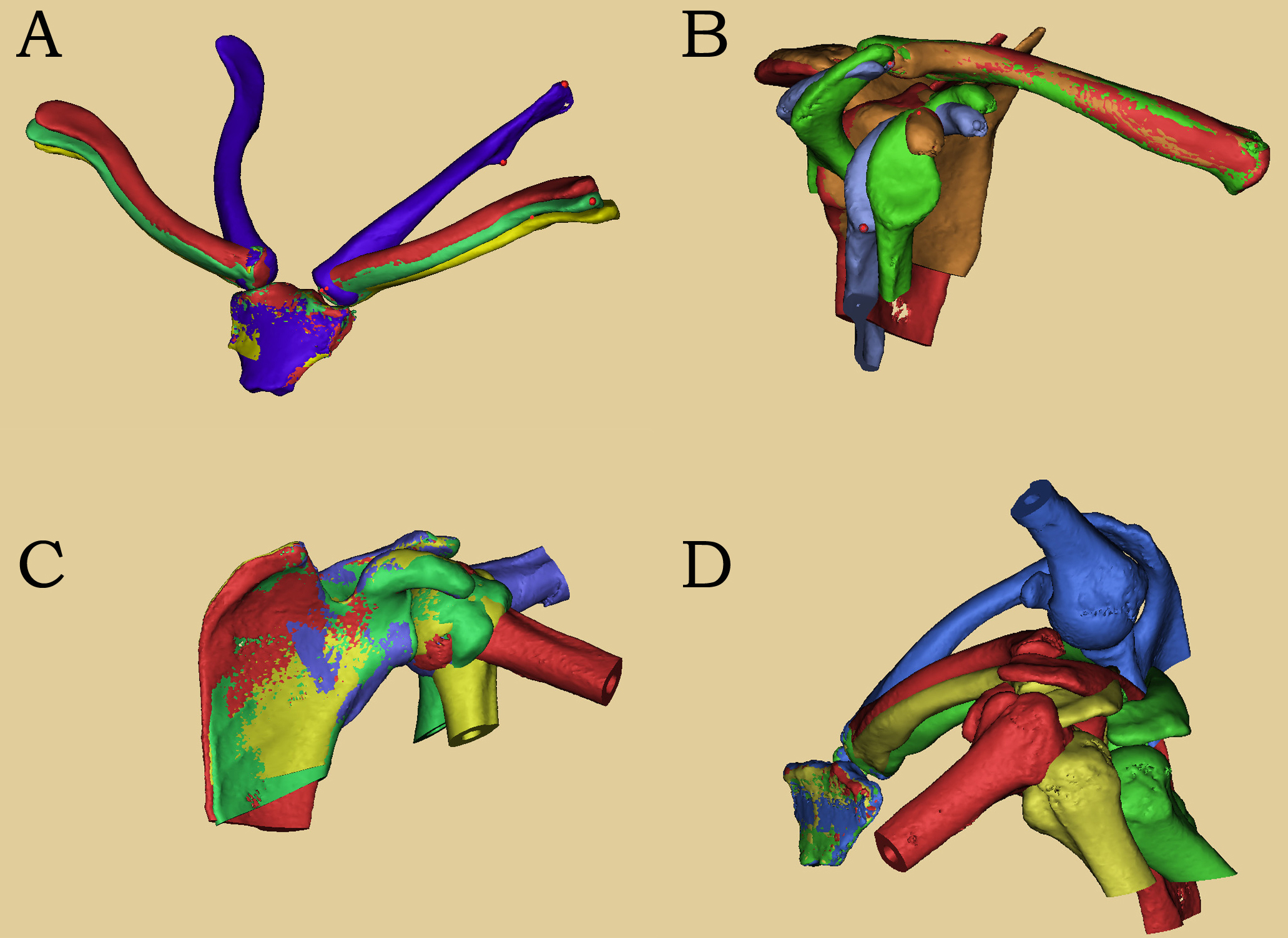
The data collection process was as follows: The ISB-recommended bony reference points of the sternum, clavicle, scapula, and humerus were labeled at corresponding positions in the 3D images. The rotational motion of the sternoclavicular joint was studied, and the 3D coordinates (X, Y, Z) of the marker points of the clavicle of the posterior and inferior upper limbs were collected as measurement data. The rotational motion of the acromioclavicular joint was explored, and the 3D coordinates (X, Y, Z) of the marked points on the scapula of the upper extremity were collected as measurement data. The rotational motion of the glenohumeral joint was studied, and the 3D coordinates (X, Y, Z) of the marked points on the scapula of the upper extremity were collected as measurement data. Finally, the rotational motion of the sagittal plane of the humerus was examined, and the 3D coordinates (X, Y, Z) of the humeral markers were collected as measurement data.
For data processing, the coordinate of the marked point in the virtual 3D space and the coordinate after skeletal rotation were identified. The pose transformation equation of the skeleton in the 3D space was obtained via the coordinate transformation of the 3D space, which was represented by the rotation vector. The pose angle included the rotation angle from the resting position to the horizontal position of the upper limb, the rotation angle from the horizontal position of the upper limb to the posterior and upper positions, and the rotation angle from the resting position to the posterior and lower positions of the upper limb.
The calculated data result provided the rotation angle irrespective of the rotation axis. Since the rotation axis was independent of the calculation of the scapulohumeral rhythm, the rotation angles were comparable.
The data included 26 shoulder complexes, 104 joints, and 312 angular results of the postures of the 13 voluntary participants in this study.
According to the dominant side, the volunteers’ bilateral shoulder complex model was first divided into dominant and non-dominant sides. The rotation angles of the dominant and non-dominant sides (i.e., four joints, each with three postural variations) of the same volunteers were analyzed statistically using an independent-samples
Comparison of the rotation angles between the dominant and non-dominant sides of the four joints in the three postures
Comparison of the rotation angles between the dominant and non-dominant sides of the four joints in the three postures
Statistical method
The sternoclavicular joint, the acromioclavicular joint, the glenohumeral joint, and the humeral motor angle in the dominant and non-dominant groups were analyzed. Statistical analyses were performed on the same postural change angle for the same joint, and paired
Sternoclavicular joint: rest-horizontal group, horizontal-posterior and upper group, rest-posterior and lower group. Acromioclavicular joint: rest-horizontal group, horizontal-posterior and upper group, rest-posterior and lower group. Glenohumeral joint: rest-horizontal group, horizontal-posterior and upper group, rest-posterior and lower group. Humeral motion angle: rest-horizontal group, horizontal-posterior and upper group, rest-posterior and lower group. The angles of motion of the sternoclavicular, acromioclavicular, glenohumeral, and humerus joints were described statistically. An ANOVA was performed between groups of different postures of the same joint (a
The horizontal resting position, the horizontal position of the upper back, and the resting position of the lower back were measured in the sternoclavicular, acromioclavicular, and glenohumeral joint groups. The contribution ratio of the rotation angle of the sternoclavicular, acromioclavicular, and glenohumeral joints to the range of the sagittal motion angle of the humerus in each posture was analyzed statistically using a Chi-squared test (A
The horizontal resting position was measured in the sternoclavicular, acromioclavicular, and glenohumeral joint groups. The horizontal position of the upper back and the resting position of the lower back were measured in the sternoclavicular, acromioclavicular, and glenohumeral joint groups. Linear regression analyses were performed on the rotation angles of the sternoclavicular, acromioclavicular, and glenohumeral joints corresponding to the motion angles of the sagittal plane of the humerus in each posture. Finally, the
The statistical analysis was conducted using SPSS 25.0 software. Measurement data were expressed as mean
The comparison of rotation angles of the dominant and non-dominant shoulder complex models in the sagittal plane of the upper limb in different motion postures in the same subject
The analysis of the results (see Table 1) showed that there was a statistically significant difference between the dominant and non-dominant sides in the rotation angle of the sternoclavicular joint when changing from the resting position to the posterior inferior position. The angle of the dominant side was approximately 1.1
Statistical description of the rotation angles of the sternoclavicular, acromioclavicular, humeral glenoid, and humeral axillary joints in different postures
Results of ANOVA of the rotation angles of the sternoclavicular, acromioclavicular and humeral glenoid joint in different postures
Results of ANOVA of the rotation angles of the sternoclavicular, acromioclavicular and humeral glenoid joint in different postures
Statistical results of the proportional contribution of the three joints of the scapular chain model in different motion postures
The analysis of the results (see Table 2) showed that in the sagittal movement of the upper limb, the sternoclavicular joint rotated at a maximum rotation angle of 23.55
The analysis of the results (see Table 3) showed that there were statistically significant differences in the proportional contribution among the three joints in all three motion postures in the composite motion.
Results of regression analysis of the sternoclavicular, acromioclavicular, humeral glenoid and humeral-axillary joints in different postures
Results of regression analysis of the sternoclavicular, acromioclavicular, humeral glenoid and humeral-axillary joints in different postures
The analysis of the results (see Table 4) showed that during the change of posture from the resting position to the horizontal position, there was a linear relationship in the motion angle between the humerothoracic and sternoclavicular joints, with a
Discussion
The sternoclavicular joint, acromioclavicular joint, and glenohumeral joint rotate at different angles in different directions simultaneously, which collectively completes the 3D rotational movement of the humeral axillary joint [10]. As the starting joint, the sternoclavicular joint is connected to the sternum and is influenced by movements of both respiration and the thoracic spine. The acromioclavicular joint is influenced by clavicular rotation, and the glenohumeral joint is affected by scapular rotation. Therefore, in composite movements, the rotation angles of the sternoclavicular, acromioclavicular, and glenohumeral joints are difficult to measure.
In recent years, many methods have been used to measure the rotation angles of shoulder-related joints, including X-ray stereophotogrammetry, non-invasive electromagnetic tracking device measurements, optical tracking systems [11, 12], and in vivo spiculation measurements [13, 14]. Among these methods, the most accurate measurement is considered to be obtained using a bone pin fixed on the scapula of a living body; however, this causes injury to healthy bones, and the associated pain and discomfort limit both extreme shoulder posture and natural movement. Optical tracking systems and electromagnetic tracking devices are non-invasive, painless methods that utilize skin markers [15]; however, the accuracy of the measurement results is affected by slippage between soft tissue and bone.
The 3D–2D model alignment technique is used for 3D measurement and evaluation using 2D fluoroscopic images. Initially, it was used to measure in vivo 3D kinematics in total knee arthroplasty, and several studies have reported shoulder kinematics using this measurement technique [16]. For example, Seo [17] conducted a dynamic measurement and assessment of the function of the rostral collateral ligament of the shoulder using the 3D alignment technique. Unlike invasive in vivo spiculation measurements or photoelectric/electromagnetic tracking methods, which are susceptible to the interference of the skin [9, 18], the 3D model alignment technique is a non-invasive method of measuring dynamic kinematics.
The scapulohumeral rhythm identified in an earlier study [5] was based on the 2D planimetric measurements obtained from X-ray imaging. Inman [5] reported that the effects of the movements of respiration and the thoracic spine on the measurement of angles could lead to certain measurement errors and that there were limitations in describing the rotation in 3D via angles on a 2D plane. De Groot [19] showed that the previously reported 2D scapulohumeral rhythm was obtained from a single 3D movement of the scapula and that the results were not accurate enough. Finally, Kojima [20] revealed that 2D measurements were invalid for 3D analysis.
The emergence of 3D motion analysis systems has made it difficult to express the scapulohumeral rhythm in the 3D space. In 2015, the ISB [7] recommended using a joint coordinate system using bony marker points as well as Euler angles to indicate rotation, the order of which was specified. However, in the same joint, the rotation order of the Euler angles is not consistent. A study by Phadke [21] showed that the YXY sequence recommended by the ISB was not suitable for describing the abduction of the glenohumeral joint, suggesting that the XZY sequence might be suitable for describing the elevation and other functional movements of the upper limb. Therefore, there is no ideal way to describe all the ranges and planes of the motion of the shoulder.
Usually, the study of scapulohumeral rhythms using Euler angles starts with two angles defined from the rotation matrix of the adjacent bones in the shoulder complex that correspond with clinically described bone movements; this is also used for analysis [21]. Some researchers [11, 16, 23] have expressed the scapulohumeral rhythm in terms of the ratio between the elevation angle of the humeral axillary joint and the superior rotation angle of the glenohumeral joint during the dynamic measurements of the elevation of the upper limb. Although this approach is inconsistent with the original definition of the scapulohumeral rhythm [24], it appears to have become the most commonly used method. However, numerous studies [16, 25, 26, 27] have found that the order of rotation of the Euler angles has different effects on the measurement results, and the clinical significance is not easily understood.
The rotation is defined in terms of two values by the rotation vector: one is a vector, and the other is an angle around which the vector rotates. The rotation vector avoids the problem of the order of the three rotations of the Euler angles. Since there is only one rotation, the problem of mutual influence on subsequent rotations is effectively avoided. The main advantage of using rotation vectors is that there is neither singularity nor problems concerning the order [6]. Sangeorzan [28] investigated the use of the rotation vector in designing pre-surgical orthopedic protocols. Wu [29] studied its use in the computer-aided design of orthopedic devices, while Lee [30] suggested that the rotation vector could be used to represent the rotation of the joints.
In the rotation vector, a vector and a rotation angle are used to describe the rotational motion of an object in 3D. This rotation angle is unaffected by either rotation order or adjacent joints, which makes it suitable for the description and analysis of the scapulohumeral rhythm during 3D motion.
In the physical examination and diagnosis of disorders concerning the shoulder, abnormalities are usually detected by comparing the affected side with the healthy side. However, the symmetry of the normal shoulder complex movement in different planes of upper limb motion is still uncertain. Crosbie [10] found that in all planes of motion and in both unilateral and bilateral activities, there was more upward scapular rotation on the non-dominant side than on the dominant side. Conversely, Matsuki’s [16] comparison of dominant and non-dominant shoulders revealed that there was no difference in one rotational movement, while there were differences in two other rotational movements among the three rotations defined by the Euler angle. Compared with the non-dominant shoulder, the scapula of the dominant shoulder was more likely to rotate downward from the starting position, while the upward rotation increased more rapidly. Finally, Hosseinimehr [31] suggested that clinicians should be aware that scapular supination and asymmetry of the scapular rhythm might be common in athletes using overhead motions; as such, they should not be considered an indication of pathology but rather an adaptive change in the habits of the movement of the upper limb.
It is worth noting that in all the above studies, Euler angles were used to describe rotation. When studying the relationship between acromiobrachial rhythm and spinal movement, some studies [32] have reported that the sternoclavicular, acromioclavicular, and glenobrachial joints rotate in different directions and angles simultaneously, jointly completing the 3D rotation of the scapular chain. The sternum forms the sternoclavicular joint with the clavicle as the initial osseous base of the scapular chain. As the initial joint, the sternoclavicular joint is connected to the sternum, and its 3D rotational motion is affected by the respiratory movement of the thoracic cavity and the spinal movement of the thoracic vertebra. The clavicle is the middle link of the scapular chain, and its acromial end and the scapula form the acromioclavicular joint; its coracoid process and the conical tubercle of the clavicle are connected by the coracoid ligament and complete the relative movement of the clavicle and scapula. The 3D rotational motion of the acromioclavicular joint is affected by the rotational motion of the clavicle. The glenohumeral joint, as the final motion joint of the scapula chain, has the largest range of motion, which is affected by the rotation of the scapula. Therefore, the sternoclavicular, acromioclavicular, and glenohumeral joints together constitute the scapular chain, which completes the motion function of the scapular chain in the compound motion of the three joints. The rotation of the three joints in the scapular chain depends on, influences, and compensates the other joints, and rotation occurs simultaneously. In the 3D space, the rotation direction and rotation angle of the three joints are different, which makes it difficult to measure the rotation angle when studying the movement of a single joint.
The problems mentioned above were effectively solved by the use of image registration technology in this study.The analysis in the present study used the rotation angles in the rotation vector. The results showed that there were differences in the average rotational angle of the sternoclavicular joint during the transition from the resting position to the posterior inferior position between the dominant and the non-dominant sides; however, such differences were negligible in clinical practice. Therefore, during clinical examinations and outcome evaluations, the bilateral comparison method could be used by physicians to determine rotational function.
Generally, previous studies [33, 34] have concluded that the range of motion of the sternoclavicular joint in live specimens is upward of 30
The Euler angle is now commonly used in studies of the scapulohumeral rhythm. Sang [35] first defined three angles in the Euler angle corresponding to three rotations of the joint and selected one of these rotations to calculate the scapulohumeral rhythm, with a ratio of 1.7–2.0:1. Robert-Lachaine [22] investigated the 3D scapulohumeral rhythm and found that the calculation of the Euler angle by selecting one rotation angle systematically overestimated the contribution of the glenohumeral joint. Consequently, he proposed a method to evaluate the scapulohumeral rhythm by converting the three rotation angles of the Euler angle into one angle for calculation. Euler angles have been used in many different studies and have produced scapulohumeral ratios ranging from 40:1 to 0.90:1 [7, 32, 36].
Currently, there are many methods for detecting the position and posture of the scapula [29]. However, the measurement results produced by these methods are affected by the interference from respiratory movement and sternal position changes. Image registration is an effective solution to this problem. The principle of image registration is the correlation of spatial transformation between images, which can be transformed into mathematical parameter calculations via spatial registration.
For image registration with different modes, it is often necessary to convert the modes into images with the same mode [25]. Lawrence [27] pointed out in a comparative study that single-plane perspective and 2D/3D shape matching could accurately quantify the complex kinematics of the whole shoulder in a static position, thus proving that image registration technology can achieve the same accuracy as a single-plane perspective. In terms of the accuracy of image registration, three sets of standard medical image data sets and evaluation criteria were established by the Centre for Image Science at the University of Utrecht in the Netherlands. It provides the gold standard for the registration of 2D-perspective X-ray images to 3D MR/CT/3DRX images, including multi-modal image data sets (MR, CT, 3DRX), rotation centers and starting points, and evaluation criteria for experimental results. To ensure accuracy, the 3D–3D image registration conducted in the present study was checked using the visual inspection method based on the above research results. Matsuki [16] studied the 3D kinematics of dominant and non-dominant shoulders in coronal plane motion using 3D–2D registration technology. Seo [17] used 3D registration technology based on CT scan images to study the motion of the acromioclavicular joint at different positions and the changes in ligament length and tension. All of the above studies used visual inspection to evaluate the accuracy of image registration.
The major difference between the present study and previous research is that this study used a helical approach to describe the scapulohumeral rhythm; the helical approach could reflect the 3D rotation function of the joint and be suitable for describing and evaluating the scapulohumeral rhythm.
In the present study, the presence of the scapulohumeral rhythm in specific postures of the shoulder complex during 3D composite sagittal motion was demonstrated by a regression analysis. The results indicated that the glenohumeral joint is very important in the motion of each joint of the scapular belt. In the three postural changes, there was a corresponding relationship between the glenohumeral joint and the coronal plane of the upper extremity (
The present study found different ratios between the humerothoracic and sternoclavicular joints during the postural changes from the resting position to the horizontal position and from the horizontal position to the posterior superior position. Since the sternoclavicular joint is easily palpable on the surface of the body, its 3D rotational motion is easily assessed by physical palpation during the sagittal motion of the upper limb from the resting position to the posterior superior position. As the most distal joint of the shoulder complex, the glenohumeral joint has the greatest mobility in every posture and has the highest proportional relationship and best consistency with the humeral axillary joint. Therefore, a dysfunction of the glenohumeral joint would have the greatest impact on the overall function of the shoulder complex and would be the most easily detected and valued. However, there are two existing problems with this. First, there are few studies on the sagittal rotation of the scapular chain, and the measured data is not accurate due to the influence of respiratory and sternal movements. Second, there are few reports on the scapulohumeral rhythm, and there is no quantitative study on the correlation.
Studies have revealed that the 2D scapulohumeral rhythm previously reported in other literature was obtained from the single 3D motion of the scapula, but the results were not accurate enough. Another study [37] showed that 2D measurements were apparently ineffective against a 3D analysis. Therefore, the 2D scapulohumeral rhythm should not be used for comparisons between individuals. Currently, there is no consensus on the description method of the 3D scapulohumeral rhythm.
When the Euler angle is used to describe the 3D rotation angle in the study of the scapulohumeral rhythm, two Euler angles of adjacent bones in the scapular chain are usually selected for definition to make them correspond to the bone joint movement described clinically; then, they can be analyzed and studied [38]. Some researchers [30, 15] have used the ratio between the scapulothoracic wall joint elevation angle and the glenohumeral joint superrotation angle to describe the scapulohumeral rhythm in the dynamic measurement of upper limb elevation. However, the scapulothoracic upward rotation angle neglects some of the total contributions of the scapulothoracic joint; additionally, the scapula rotates backward during the movement, and this interaction directly influences the elevation angle of the upper limb. The change in the contribution of the scapulothoracic joint is noticed mainly in abduction, where the common method obtains approximately 14
Sang [35] first defined three Euler angles corresponding to three rotations of the joint and selected one rotation to calculate the scapulohumera rhythm, with a ratio of 1.7–2.0:1. Robert-Lachaine [38] studied the 3D scapulohumeral rhythm and found that the calculation method of using Euler angles to select a rotation angle systematically overestimated the contribution of the glenohumeral joint. He proposed the method of converting three rotation angles of Euler angles into one angle to evaluate the scapulohumeral rhythm.
In the present study, the 3D rotation angle was described by the rotation vector; since the acromiobrachial rhythm was evaluated by the rotation vector, no definition was required. This is one of the important innovations of this study.
Herein, CT 3D registration technology was used to exclude the influence of respiratory and sternal movement on the activities of each joint of the scapular chain and analyze the sagittal motion of the sternoclavicular, acromioclavicular, and glenohumeral joints. Rotation vector measurement technology was used to analyze the degree of rotation of the sternoclavicular, acromioclavicular, and glenohumeral joints in the sagittal position, and a correlation test was used to analyze the rhythm of the glenohumeral joint.
As the middle joint of the shoulder complex, the acromioclavicular joint plays a role in the conduction, connection, and compensation of the movement of that complex. Although there is no fixed proportional relationship of activity between the acromioclavicular joint and the humeral axillary joint, the acromioclavicular joint coordinates sternoclavicular and humeral glenoid movements, both compensating for and complementing the differences and deficiencies in the rotational function of the shoulder complex during composite movement. Due to the anatomical characteristics and special kinematics of the shoulder complex, the acromioclavicular joint is the most likely joint to be overlooked, and it is likely to be detected only during extreme movements.
Limitations of the study
This study has some limitations. The sample size of this study was small, which may have impacted the reliability of the research results. Although each volunteer in this study was approved by the hospital’s ethics committee and provided signed informed consent, some participants failed to complete the research. Due to the CT equipment used to collect the image data, the volunteers were exposed to radioactivity.
The standard reference position of the sample was the supine resting position; this was different from the initial position of the scapular chain under the upright resting position, which may have biased the results to some extent. When the data on the different postures of the shoulder chain were collected at the same time, the samples were all in the decubitus state. The three postures acquired at the same time were the active motions of the shoulder complex, which were imaged in a state of gravitational resistance. Since the shoulder chain was activated against gravity, some bias may be present in the results due to the influence of upper limb gravity and muscle strength.
Conclusion
The application of image alignment technology in the study of the movement of each joint in the shoulder complex had the advantages of accuracy and non-invasiveness and was able to measure the bony structures directly and accurately. The helical approach provided an accurate description that corresponded with clinical language, and the method was suitable for describing the scapulohumeral rhythm during 3D movements. In the clinical physical examination and therapeutic evaluation, the rotational function of each joint in the shoulder complex was determined by the bilateral comparison method. Finally, there was a scapulothoracic rhythm in the 3D sagittal composite motion of the shoulder complex, mainly between the humeral axillary joint and the glenohumeral joint; the ratio varied with the changes in motion postures, with the ratio coefficient ranging from 0.53 to 0.939.
Funding
This work was supported by the Scientific Research Project of Key Medical Disciplines in Shijingshan District, Beijing (2018).
Consent for publication
Written informed consent was obtained from the individuals for the publication of any potentially identifiable images or data included in this article.
Footnotes
Acknowledgments
The authors would like to acknowledge the hard and dedicated work of all staff that implemented the intervention and evaluation components of the study.
Conflict of interest
The authors declare that they have no competing interests.