
Abstract
BACKGROUND:
The reason that participants develop pain episodes during the Sorensen test remains unclear. Lumbar lordosis and trunk muscle are important for dynamic stability of the spine; however, their role in pain episodes during the Sorensen test has not yet been discussed.
OBJECTIVE:
To investigate the effects of muscular morphology and lumbar curvature on pain development during the Sorensen test in patients with non-specific low back pain (LBP).
METHODS:
Ninety-one patients diagnosed with chronic non-specific LBP and underwent the Sorensen test were enrolled. Lumbar lordosis, cross-sectional area and fat infiltration rate of trunk muscle and centroid line of psoas major (dividing into three types: anterior arc, linear and posterior arc) were measured using ImageJ software. All recruited patients were grouped into pain episode and exhaustion groups and were matched for the confounders based on propensity scores. The above parameters were compared between groups and further adjusted for confounding bias.
RESULTS:
After adjustment , the mean differences in lumbar lordosis of 12.1
CONCLUSIONS:
Lower lumbar lordosis and linear and posterior arc types of the psoas major centroid line were possibly relevant to the pain episode during Sorensen test in patients with chronic non-specific LBP.
Background
The Sorensen test is a cost-effective and time-efficient clinical assessment of isometric extensor endurance with high reliability [1, 2, 3, 4, 5, 6]. It has important implications in distinguishing between participants with and without lower back pain (LBP), predicting the occurrence of LBP in the near future, and documenting the effect of specific rehabilitation programs to improve muscle endurance.
However, all participants, with or without LBP, are likely to experience pain during the test and may be unable to maintain their neutral posture. This limits the test’s applicability, particularly for patients with LBP [1, 4]. Nevertheless, the reason that patients with chronic non-specific LBP develop pain episodes during the Sorensen test remains unclear.
Maintenance of normal spinal posture within the cone of economy is dependent on the intrinsic balanced sagittal spinal alignment acquired by the coordinated actions of the passive subsystem and spinal trunk musculature [7]. A deficiency in one component of the spinal stability mechanism may lead to overall stabilizing system dysfunction and cause pain.
Numerous studies have revealed a potential relationship between the development of LBP and lumbar curvature [8]. Aspden has proposed that erector spinae may appear in the silent activation period early from the less lordotic initial posture during a lift, making it more difficult to bear the load by early torque and counteract the strain on the tissues [9].
Furthermore, paraspinal muscle degeneration, characterized by decreased muscle size and increased fatty infiltration, may compromise spinal stability and be associated with LBP [10]. A study examining a community population, without comments on LBP, determined that there was an increased risk of high-intensity pain in those with a high percentage of fat in the paraspinal muscles [11].
In addition, the psoas major may have functioned as a synergistic muscle during lumbar extension and are possibly associated with LBP. A biomechanical study reported that increasing lumbar lordosis was achieved by shortening the distances of the psoas major attachments in vertebrates to the iliopubic eminence, indicating that the contraction of the muscle was related to lumbar extension [12]. Another study exhibited that a smaller psoas major was present in patients with chronic LBP when compared to healthy controls [13].
However, the role of lumbar curvature and trunk muscular morphology in pain episodes during isometric trunk extension in patients with chronic non-specific LBP has not yet been discussed.
We hypothesized that the development of pain during the Sorensen test may indicate a failure to strengthen spinal stability during isometric trunk extension due to the deficiency in sagittal lumbar spinal alignment, such as reduced lumbar lordosis or due to the inability of spinal musculature to provide needed stability.
The current study aimed to investigate the effects of muscular morphology and lumbar curvature on pain development during isometric trunk extension to better understand the applicability of the Sorensen test in patients with non-specific LBP.
Materials and methods
Patient population
Flowchart. Patients diagnosed with chronic non-specific LBP and underwent the Sorensen test between June 2017 and December 2020 were retrospectively screened. All eligible patients were grouped into pain episode and exhaustion groups according to the reason for termination during the Sorensen test and matched based on propensity score.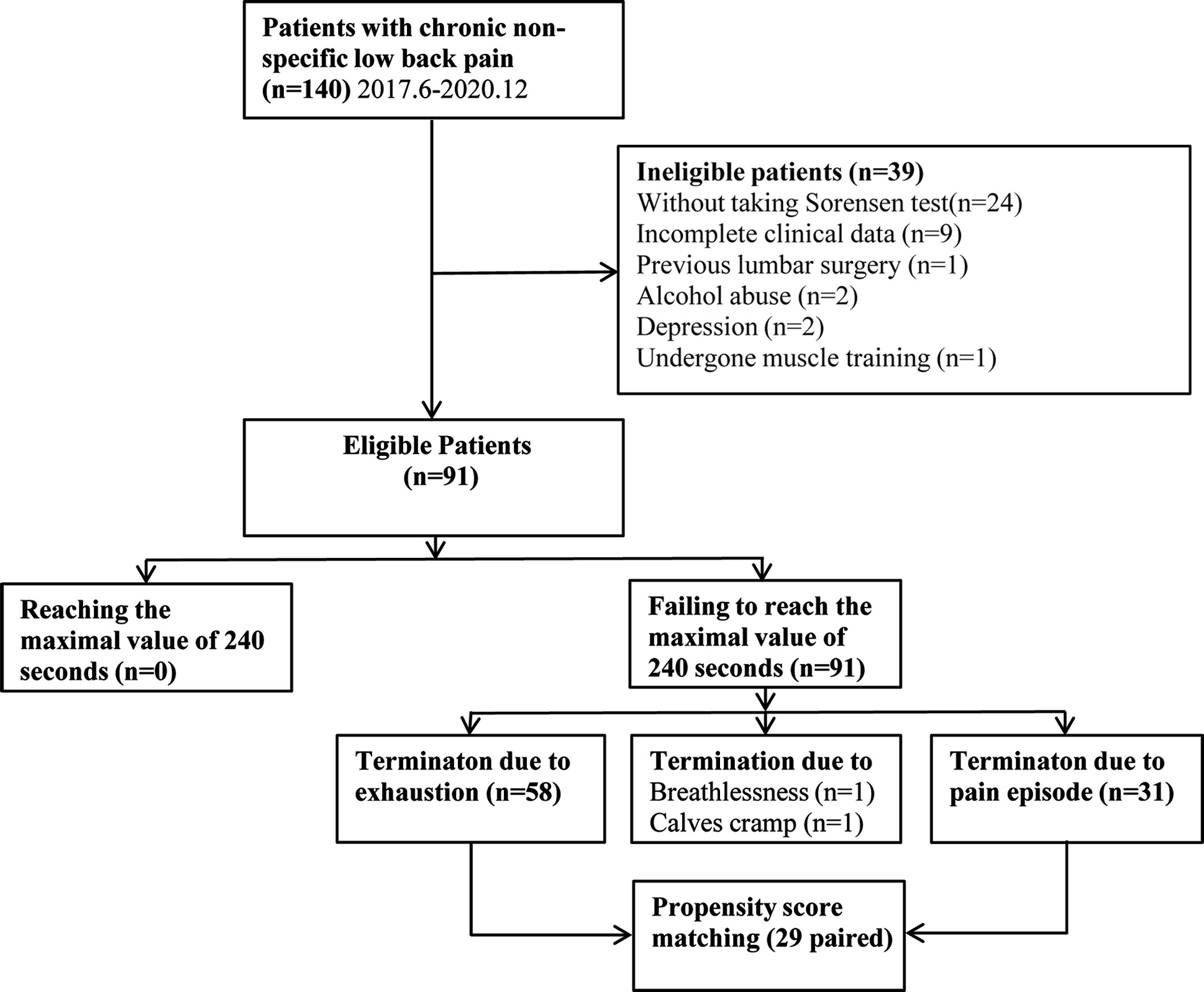
This retrospective observational study was conducted in compliance with the Declaration of Helsinki and approved by the local research ethics review committee. Patients diagnosed with chronic non-specific LBP in the orthopedic clinic of our hospital between June 2017 and December 2020 were retrospectively screened (Fig. 1). All patients who underwent the Sorensen test were candidates for enrolment in this study. Informed consent was waived due to the retrospective nature of the study design.
Chronic nonspecific LBP was defined as pain not attributable to specific pathologies, such as infection, tumor, trauma, osteoporosis, facet pathology, structural deformity, radicular syndrome, or cauda equina syndrome.
The exclusion criteria included incomplete clinical data or radiographic images, previous lumbar surgery, depression, drug or alcohol abuse, muscle training within the past year, and disorders likely to affect muscle function, such as Cruveilhier atrophy, polyneuropathy, skeletal dysplasia, and atherosclerosis.
Data on age, sex, body mass index (BMI), work status (prolonged sitting/prolonged standing/working with changing positions), symptom duration, visual analogue scale (VAS) scores for LBP, and the Mental Health Component of the Medical Outcomes Study 36-item Short-Form Health Survey (SF-36 MH) were recorded at their first visits to our clinic.
The Sorensen test is one of the optional physical examination items available at our institution that is used to understand the function of the back muscles of patients with non-specific LBP and patients were able to voluntarily accept this test. Contraindications to the test included patient refusal, patients who experienced pain episodes in the previous four weeks that had at least a serious impact on their work or housework, and patients who experienced severe pain (VAS
The procedure of the Sorensen test in the current study was consistent with that reported elsewhere in the literature (Supplementary Table 1). In circumstances where a patient could no longer maintain the horizontal posture, or reached the maximal value at 240 seconds, the test was terminated [1, 4]. Using Borg’s scale, patients were asked to rate their perception of the strain immediately after the test.
Radiological analysis
Measuring parameters. The lumbar lordosis (LL) was measured from the superior endplate of L1 to the superior endplate of S1. The vertebral body (VB) and the fascial boundaries of psoas major (PM) , multifidus muscle (MF) and erect spinae (ES) are marked on axial T2-weighted magnetic resonance image (MRI) to measure the muscular cross-sectional area (CSA) and centroid of psoas major. The fatty infiltration rate of the muscles is measured by using the threshold technique (a–f). The line connecting the projection of psoas major centroids measured on axial MRI from L1-2 to L4-5 segments in the sagittal MRI were depicted and divided into three types: the posterior arc type, in which the arc composed by the centroid line is located posterior to the center of the arc (g); the linear type (h); and the anterior arc type, in which the arc is in front of the center of the arc (i). 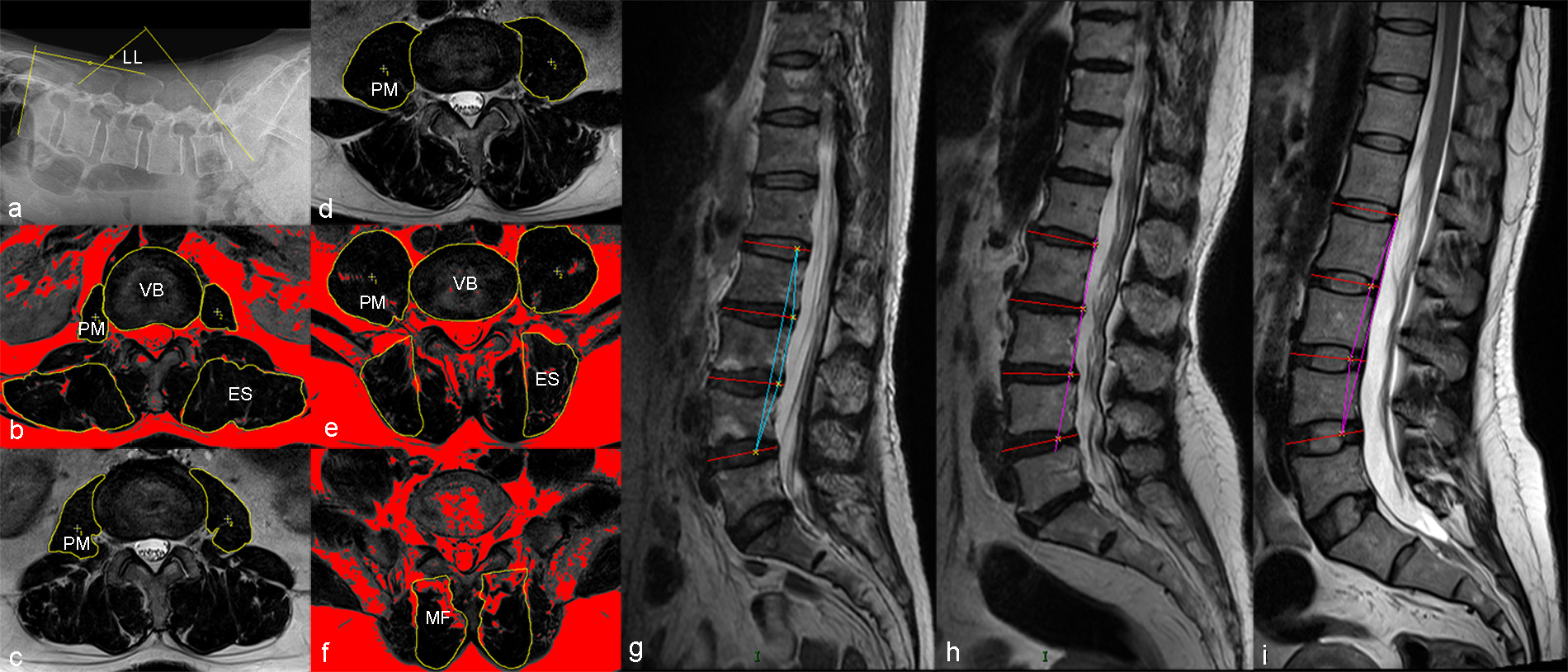
Radiographic images were retrieved from a hospital radiographic system (Picture Archiving and Communication Systems, GE Healthcare, IL, USA). Magnetic resonance imaging (MRI) was performed using a 3.0 Tesla System (GE Healthcare) with a standard spine array coil. Imaging protocols included the acquisition of axial and sagittal T2-weighted images (TR/TE 3500/106, matrix size, 208
Lumbar lordosis was measured from the superior endplate of L1 to the superior endplate of S1. The cross-sectional area (CSA) of the bilateral psoas muscle from L1-L2 to L4-L5 segments on axial MRI was measured at the superior endplate level of the lower vertebral body (VB) using ImageJ software (ImageJ, version 1.5, National Institutes of Health, Bethesda, Maryland, USA). The CSA and fatty infiltration rate of the bilateral erect spinae at the L1-L2 and L4-L5 segments and the bilateral multifidus muscle at the L5-S1 segment were also evaluated using the threshold technique. The CSA of the muscles was further divided by the CSA of the superior endplate of the corresponding lower VB to eliminate bias arising from variations in patient build (Fig. 2a–f). Mean bilateral muscle parameters were calculated for further analysis.
The centroid line between nodes of psoas major at each lumbar intervertebral level was delineated to indicate the line of action of the muscle in prior anatomy and imaging studies, and was the focus of the current study [12, 14, 15, 16]. We depicted the line connecting the projection of psoas major centroids measured on axial MRI from L1-2 to L4-5 segments using ImageJ software in the sagittal plane to represent the action line of the psoas major in the current study. The centroid line of the psoas major was divided into three types (Fig. 2g–i): the posterior arc type, in which the arc composed by the centroid line is located posterior to the center of the arc; the linear type; and the anterior arc type, in which the arc is in front of the center of the arc.
Two clinicians blinded to the patient data evaluated all morphological parameters, and repeated the evaluation in a different order, one month after the first measurement. Intraclass correlation coefficients (ICCs) were calculated to assess measurement reliability with respect to morphological parameters. The intra- and inter-rater reliabilities were in excellent agreement (ICC 0.81 and 0.93).
All recruited patients were grouped into pain episode and exhaustion groups according to the primary reasons for termination during the Sorensen test.
It was proposed that the determinant of individual physical performance was the perceived effort, defined as the conscious assessment of the strenuousness of the exercise; any physiological or psychological factors affecting the perception of effort may affect the participant’s physical performance [17, 18, 19]. Therefore, the perceived exertion and mental status were included in propensity score matching (PSM) analysis used to reduce related confounding bias.
Moreover, trunk morphology and lumbar curvature might be potentially impacted by age, sex, BMI, work status, symptom duration, and VAS score; these covariates were included when analyzing differences in targeted parameters between the two groups [20, 21, 22, 23, 24].
It was speculated that the psoas major centroid line might be greatly determined by the geometry of the psoas major and the muscle positions corresponding to the lumbar intervertebral joints based on the available data [12, 14, 15, 16]. Accordingly, we assumed that factors with a potential relationship with the psoas major morphology reported in the literature should also be included as covariates that may affect the psoas major centroid line in the current study.
Comparisons in clinical data between the termination due to pain episode group and termination due to exhaustion group before and after propensity score matching
Comparisons in clinical data between the termination due to pain episode group and termination due to exhaustion group before and after propensity score matching
BMI indicated body mass index, VAS indicated visual analogue scores.
Comparisons morphological parameters between the two groups before matching (
LL indicated lumbar lordosis, PM indicated psoas major, CL indicated centroid line of psoas major, ES indicated erect spinae, CSA indicated cross-sectional area, FIR indicated fatty infiltration rate, MF indicated multifidus muscle, VB indicated vertebral body. The mean difference between 2 groups were adjusted by Age, Sex, BMI, Work status, VAS back pain, Symptom duration, SF-36 Mental health, Borg’s scale.
All data analysis was carried out using SPSS version 24.0 (IBM Corp., Armonk, NY, USA). Statistical significance was set at
Propensity score matching. Propensity scores of the enrolled patients (a) show that 29 pairs of patients from the pain episode and the exhaustion groups were matched based nearest-neighbour scores. Histograms with overlaid kernel density estimates of standardized differences before and after matching showed standardized differences in covariates after matching concentrate near “0” which indicates excellent matching effect (b).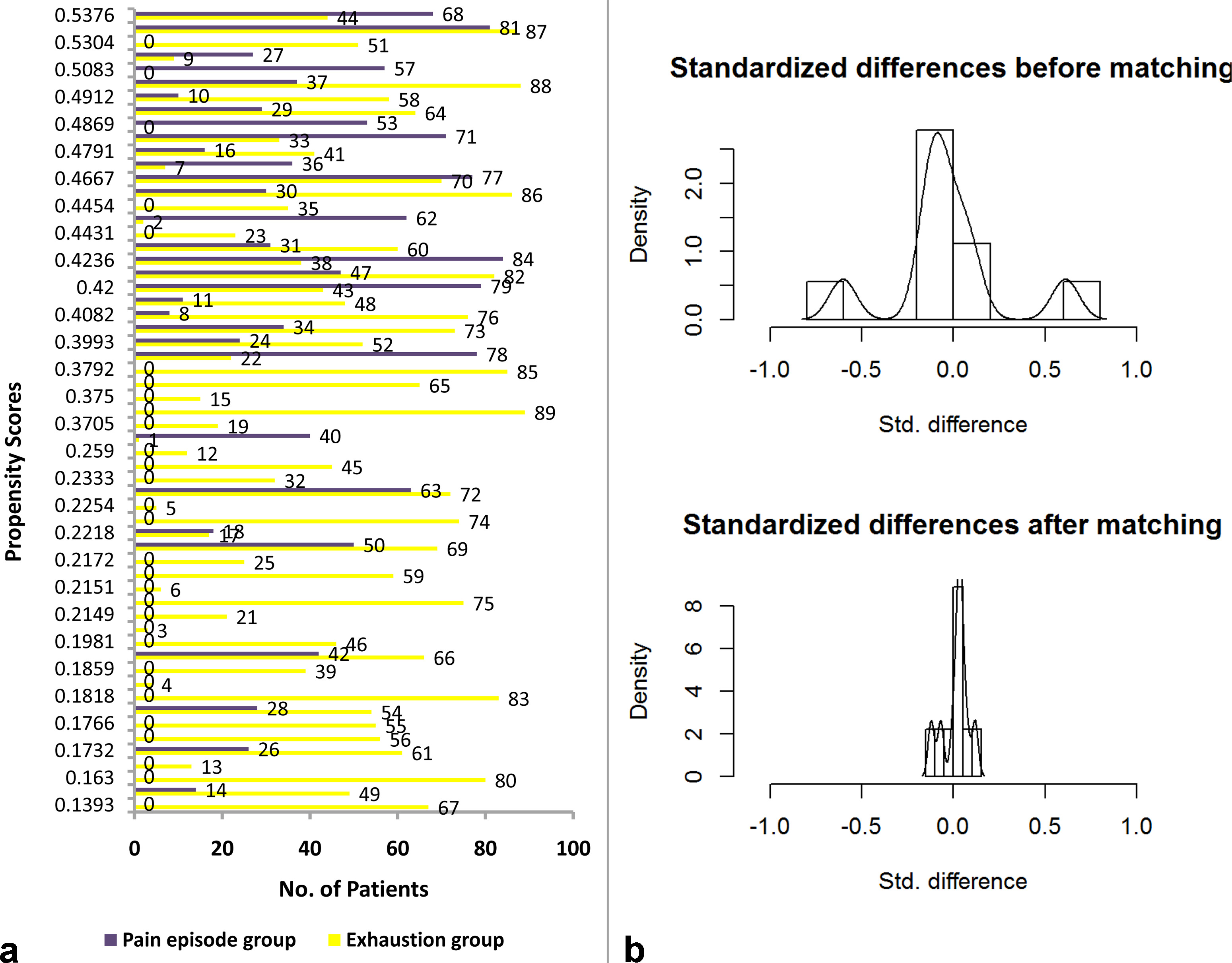
Ninety-one patients (mean age 47.8
Before matching, there were fewer male patients in the pain episode group than in the exhaustion group (Table 1). The above covariates were entered into the logistic regression model to determine propensity scores. Twenty-nine pairs of patients were then matched according to the nearest-neighbor matching scores, taking the caliper value of 0.15 (Fig. 3a). After matching, the standardized differences were concentrated near “0” (Fig. 3b), no covariate exhibited a significant imbalance (
Comparisons between groups
Comparisons morphological parameters between the two groups after matching (
58)
Comparisons morphological parameters between the two groups after matching (
LL indicated lumbar lordosis, PM indicated psoas major, CL indicated centroid line of psoas major, ES indicated erect spinae, CSA indicated cross-sectional area, FIR indicated fatty infiltration rate, MF indicated multifidus muscle, VB indicated vertebral body. The mean difference between 2 groups were adjusted by Age, Sex, BMI, Work status, VAS back pain, Symptom duration, SF-36 Mental health, Borg’s scale.
Comparisons the parameters between the two groups. Lumbar lordosis in the pain episode group was significantly lower than that of the exhaustion group in both the complete and matching cohorts (a). The mean difference in lumbar lordosis between the two groups in the complete and the matched cohorts remained significant after adjustment (b). There was no significant difference in other muscular parameters between the two groups in either cohort after adjustment.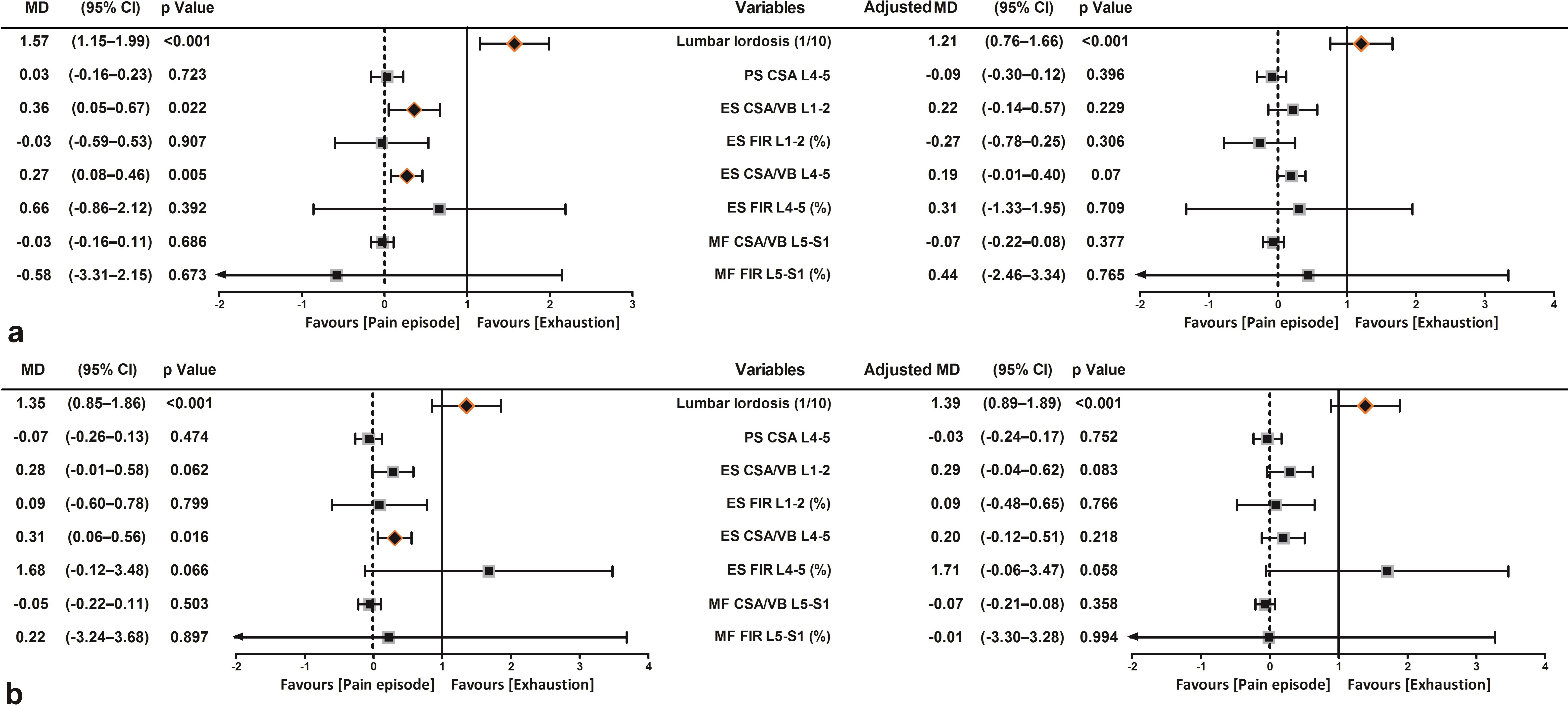
Lumbar lordosis in the pain episode group was significantly lower than that of the exhaustion group, in both the complete and matching cohorts (Table 2), and the mean differences (MD) between the two groups were 15.7
The erector spinae CSA/VB L1-2 was statistically significantly smaller in the pain episode group than in the exhaustion group only in the complete cohort; although the MD between the two groups did not remain significant after adjustment (Table 2, Fig. 4). In both cohorts, erector spinae CSA/VB L4-5 was statistically significantly smaller in the pain episode group than in the exhaustion group, whereas the MD between the two groups were insignificant after adjustment in either cohort (Tables 2 and 3, Fig. 4). In addition, no significant differences were noted in other variables between the two groups in either cohort, regardless of adjustment (Tables 2 and 3).
The pain episode group had a significantly greater risk of the psoas major centroid line appearing as a linear and posterior arc than in the exhaustion group in both cohorts. After adjustment, the exhaustion group had a 0.22-fold and 0.08-fold risk of presenting as linear and posterior arcs, respectively, compared with the pain episode group in the complete cohort (
Binary logistic regression model for pain episode (
91)
Binary logistic regression model for pain episode (
BMI indicated body mass index, VAS indicated visual analogue scores, PM indicated psoas major, CL indicated centroid line of psoas major, ES indicated erect spinae, CSA indicated cross-sectional area, FIR indicated fatty infiltration rate, MF indicated multifidus muscle, VB indicated vertebral body, OR indicated odds ratio.
Comparison of psoas major centroid line between the two groups. The pain episode group had a statistically significant greater risk of appearing as the linear type and posterior arc type than the exhaustion group in either of the cohorts regardless of adjustment (a,b). 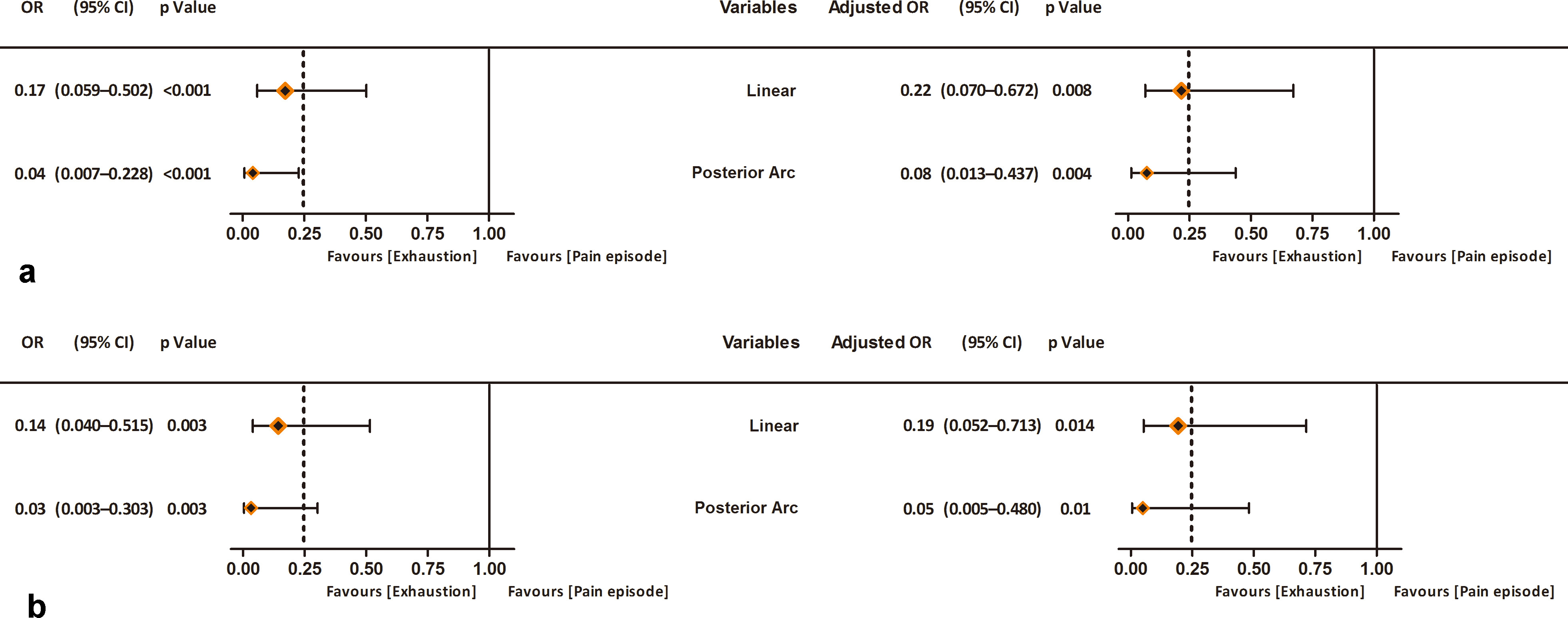
Sex, lumbar lordosis, psoas major centroid line, ES CSA/VB L1-2, and ES CSA/VB L4-5 demonstrated statistical significance in the univariate regression analysis for pain episodes during the test. However, only lumbar lordosis was an independent protective factor (odds ratio [OR]
Available data argue in favor of the Sorensen test for evaluating the isometric endurance of the trunk extensor muscles, the deficiency of which may be associated with chronic LBP [1, 4, 5, 6, 25]. Cumulative evidence has demonstrated that the position-holding time during the Sorensen test was significantly lower in patients with non-specific LBP than in that of healthy volunteers [1, 4].
The Sorensen test has been proven as a rapid, simple quantitative clinical assessment of individual potential deficiency in isometric endurance of the trunk extensor muscles for patients with non-specific LBP and asymptomatic participants who may have LBP in the future, as well as for evaluating the effectiveness of training strategies aimed at strengthening the trunk muscular endurance [25, 26].
However, the fact that pain episodes could lead to early cessation constitutes one of the major shortcomings of the test. Reports on pain episodes as a major reason for terminating the Sorensen test in patients with non-specific LBP are limited [1, 2, 3, 4, 5, 6, 19, 26].
Sorensen firstly revealed that among participants, with or without previous LBP, who failed to achieve the maximal holding time of 240 seconds, 35% of men and 25% of women stated back pain as the reason for termination. In patients with a history of previous pain occurrence, up to 74% of men and 54% of women stopped the test early, although the reasons for termination were unclear [1]. Tekin and Simmonds reported that no participants reported pain episodes while performing the Sorensen test; however, patients who experienced LBP recently were excluded from these two studies because of concerns that patients with LBP might experience pain aggravation during the test or were requested to execute the tasks at a level that would not increase their pain, which may have been a psychological motivation to avoid symptoms [19, 26].
In the few studies that reported termination of the holding posture as a result of pain episodes, approximately 32.5% of patients with LBP who began the test, discontinued due to pain episodes. However, the reason for the pain episodes is yet to be clarified.
As mentioned in the literature, dynamic spinal stability may be determined by passive tissue stiffness, spinal posture, external load magnitude, and trunk muscle activity. Recent evidence demonstrated that lower lumbar lordosis, which is unlikely to afford a mechanical advantage by shortening the lever arm of the erector spinae, tends to cause muscle fatigue during the extension task, which may increase spinal instability and fail to protect the inert ligamentous structures [27, 28, 29]. In addition, Gibbons reported that the smaller CSA of the psoas major at the L3-4 segment was associated with a shorter holding time during the Sorensen test in healthy volunteers [29]. However, little attention has been paid to the relevance of lumbar lordosis and trunk muscles and pain episodes during isometric trunk extension.
The current findings show that approximately one-third (31/91) of the patients terminated the test due to pain episodes. It was interesting to note that lumbar lordosis in the pain episode group was significantly lower when compared to that in the exhaustion group in either the complete cohort (MD
These findings support a part of our hypothesis and indicate that less lumbar lordosis and psoas major acting line may be associated with pain episodes during the Sorensen test in patients with non-specific LBP. However, these findings must be interpreted with prudence.
There is consensus that less lumbar lordosis prolongs the working length of the extensor groups, which is unfavorable for optimizing erector spinae recruitment and motion input [28, 29, 31]. While its biomechanical advantage is limited, the erector spinae is more prone to fatigue and may result in a reduced role in maintaining spinal stability [33, 34]. A subsequent increase in strain on passive stabilizing structures may augment the synergistic activation of the psoas major required to engage in lumbar extension via a proprioceptive reflex mechanism to enhance spinal stability [34, 35].
Schematic illustrations of variation of patients with different psoas major centroid line during Sorensen test. In sagittal plane, besides the compression force generated by psoas major (F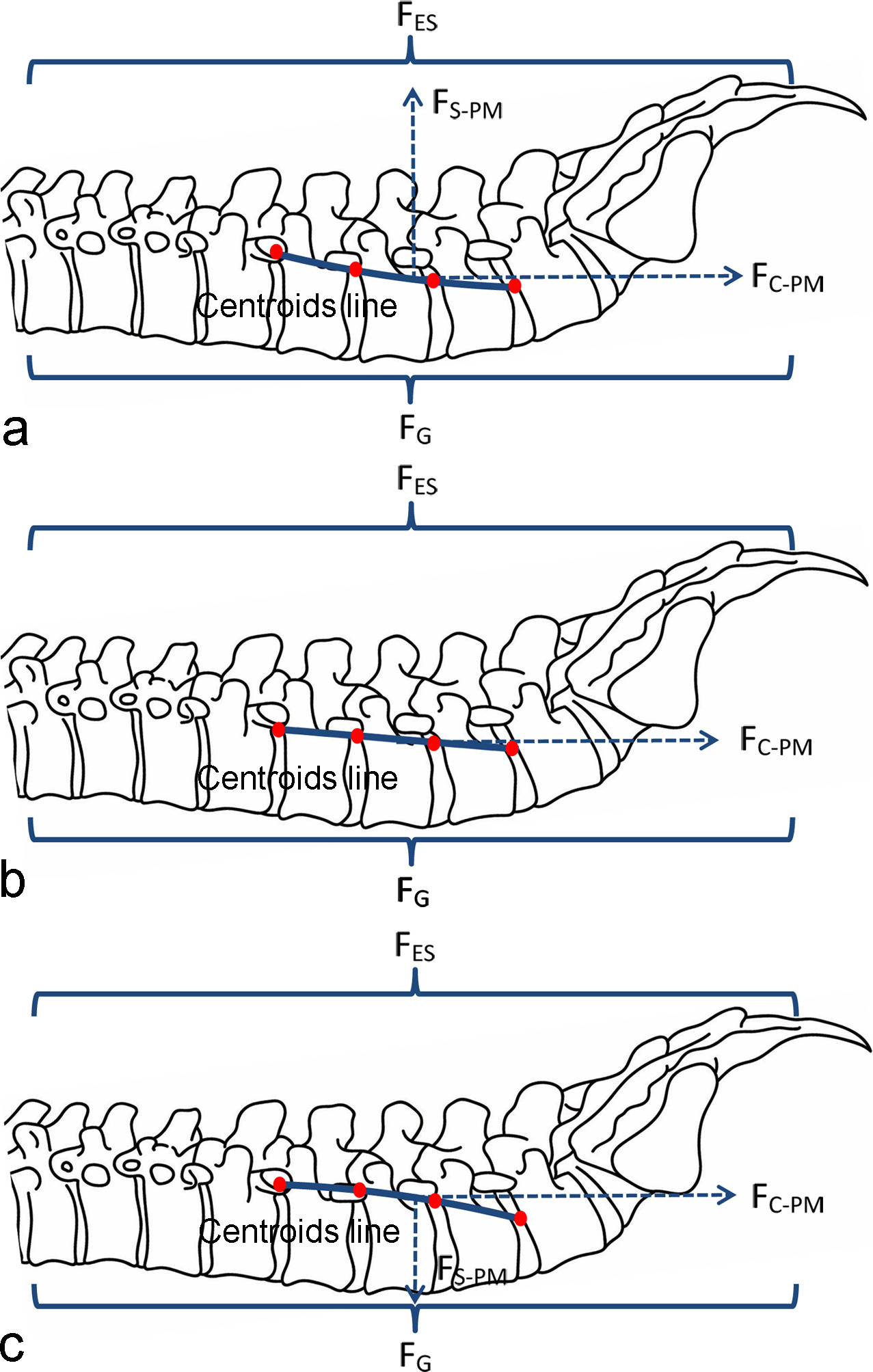
When the psoas major centroid line is of the anterior arch type, the psoas major may generate a force in the sagittal plane in the opposite direction of gravity, which is conducive to sharing the gravity load with the erector spinae and other extensors and reduces instability. Therefore, the need to increase intervertebral stiffness to maintain intervertebral stability by psoas major contraction may be minimal (Fig. 6a). With respect to the linear type, the psoas major was unlikely to provide a direct force against gravity, and the need to increase intervertebral stiffness to maintain stability by psoas major contraction might increase (Fig. 6b). As far as the posterior arch type, the psoas major may produce force in the same direction as gravity, which would aggravate the instability and cause pain episodes. Meanwhile, the need to increase intervertebral stiffness to maintain intervertebral stability by psoas major contraction might significantly increase (Fig. 6c).
The substantial compression load on the lumbar motion segments exerted by the psoas major as priced paid for lumbar stability, together with the axis load arising from the erect spinae, may excessively increase the stiffness of the innervated spine tissues and have the potential to contribute to pain episodes by irritation of the nociceptors in the intervertebral joint [36, 37, 38, 39]. Mechanical injuries related to compression loading lead to exceeded tissue tolerance limits until the termination of the task because of pain episodes [40]. Our study does not lend support to the correlations between the erector spinae and multifidus muscle and pain episodes during the test. The reason why pain in the Sorensen test was not related to the morphology of the erector spinae and multifidus muscles is not clear, and their role in the pain episode during the Sorensen test warrants further elaboration.
The study has some limitations. Each set of trunk extensors corresponds to a spine compression load that is not only proportional to its size and lever arm, but also to the activation level during the isometric extension task, which warrants further elucidation.
Although lumbar lordosis is less likely to change with the horizontalization of the sacral position, given that the positive correlation between sacral orientation and lumbar lordosis may not be affected by posture variation in the absence of extrinsic torque [41, 42], the real-time lumbar curvature during isometric extension tasks remains unclear; therefore, more data are required to understand the effect of living lumbar sagittal alignment in the prone posture on pain episodes during the Sorensen test.
In addition, prospective investigations that enroll patients at a larger scale with comprehensive potential covariates should be launched to validate the current findings, and should include healthy controls and calculated spinopelvic radiographic parameters to provide valuable insights into the influence of lumbar lordosis and psoas major centroid line on participants’ performance during the Sorensen test.
It is worth noting that the current study’s hypothesis stemmed from the consideration of the application of one assessment method commonly used in daily clinical practice without excessive exogenous intervention strategies, thus likely to reflect the real world. Moreover, it is important to balance the confounders using PSM and to adjust the effect size in a generalized linear model to close a controlled design.
Implications
Given that individuals with linear and posterior arc types of the psoas major centroid line and less lumbar lordosis may be at increased risk of pain episodes during the isometric extension task, it might also be possible to evaluate the applicability of the Sorensen test by measuring the two variables prior to the test to estimate the possibility of termination due to pain episodes during the procedure, especially for patients who plan to undergo the electromyography test synchronously. Improving the participant’s tolerance to the test itself and test applicability by placing targeted extensors in a better biomechanical position to maximize motor input or by avoiding unexpected effects from synergist muscles deserves further consideration.
Furthermore, in light of the biomechanical similarity between lifting required in many daily activities and trunk extension [43], further clarification of the relevance of lumbar sagittal alignment and trunk muscle morphology in their contribution to pain attacks during the Sorensen test might improve the existing understanding of pain development during lifting tasks.
Conclusions
Lower lumbar lordosis and linear and posterior arc types of the psoas major centroid line were possibly relevant to pain episodes as a reason for termination during the Sorensen test. A better understanding of the applicability of the Sorensen test by evaluating lumbar curvature and psoas major morphology may facilitate the assessment of trunk extensor performance in patients with chronic nonspecific LBP.
Ethics statement
This was a retrospective study aimed to investigate the relevance of lumbar lordosis and trunk muscle morphology to the pain episode during the Sorensen test in patients with non-specific low back pain All methods were carried out in accordance with relevant guidelines and regulations. Informed consent was waived due to the retrospective nature of the current study design The Research Ethics Review Committee of Beijing Electric Power Hospital of State Grade reviewed and approved this study (20180306).
Availability of data and materials
The original operation reports, imaging studies, and inpatient clinic record are retained as per normal procedure within the medical records of our institution.
The datasets generated during and analyzed during the current study are not publicly available due to the local regulations but are available from the corresponding author upon reasonable request.
Funding
None to report.
Author contributions
Yang Liu: Conceptualization Investigation, Writing – Original draft preparation, Writing – Review & Editing. Jingdong Hao: Investigation, Writing – Review & Editing. Mingkui Du: Investigation. Sanbao Hu: Conceptualization Writing – Review & Editing.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/BMR-220298.
Footnotes
Acknowledgments
We are grateful to Beijing Electric Power Hospital of State Grade for providing reliable imaging data.
Conflict of interest
None of the authors have any potential conflict of interest. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this manuscript.