
Abstract
BACKGROUND:
Extracorporeal shock wave therapy (ESWT) combined with Kinesio Tape (KT) for plantar fasciitis (PF) is lacking in the literature.
OBJECTIVE:
This study aimed to investigate the effect of ESWT combined with KT on foot pain and function in patients with PF based on ultrashort wave therapy and stretching.
METHODS:
A total of 91 patients with PF were randomly divided into the ESWT group (ETG,
RESULTS:
The groups were compared after 4 weeks and the results showed that the VAS scores of ETG, KTG and CTG were significantly smaller than that of CG (
CONCLUSION:
Based on ultrashort wave therapy and stretching, ESWT and KT therapy could improve the foot pain and function of patients with PF, and the combined modality therapy is more effective. ESWT and combined treatment has a positive effect on patients’ PFT. However, single KT treatment has a limited effect on PFT.
Introduction
Plantar fascia originates from the fibrous tissue of the medial calcaneal tubercle and extends forward to the proximal phalanx of each toe [1, 2]. It acts as a bowstring; maintains and supports the longitudinal direction of the foot arch; and assists in dynamic shock absorption, which plays an important role in maintaining the normal biomechanics of the foot [3, 4]. Plantar fasciitis (PF) is a local aseptic inflammation caused by chronic injury of the plantar fascia caused by multiple factors, such as excessive exercise, excessive weight bearing or foot arch structure and biomechanical abnormalities [5, 6]. PF is a common cause of heel pain [7]. Up to 10% of the population may present with heel pain in their lifetime. Prevalence rates of PF among a population of runners are between 4% and 22% [8]. The main symptoms include evident heel pain after getting up in the morning or starting from a sedentary stand and then gradually becoming light but with a long time of walking or standing, the pain worsens again [9].
The current treatment methods primarily include exercise treatment [10], extracorporeal shock wave therapy (ESWT) [11, 12], Kinesio Tape (KT) [13, 14], stretching [15, 16], drug injection [17, 18], foot orthoses [19, 20] and surgery [21, 22]. Nevertheless, various treatment methods have different therapeutic effects, most of which are combined modality therapy and some have long treatment cycles, high costs and a certain risk of complications [23, 24]. Amongst them, ESWT is an effective and convenient method recommended to treat patients with chronic PF with poor efficacy [11, 12]. Meanwhile, KT is widely used in musculoskeletal diseases. It effectively relieves muscle spasm pain, improves joint stability and promotes motor sensory input; it also relieves pain symptoms of patients with PF [13, 14]. Two previous studies compared the efficacy of ESWT and KT in treating PF and both treatments improved the pain levels and quality of life in patients with PF [25, 26]. However, another study compared the treatment difference between ESWT combined with KT and ESWT and found that the two treatment methods did not provide a significant benefit on pain and heel tenderness caused by PF [13]. Nevertheless, no relevant literature has been reported on whether or not the additional ESWT and KT treatment and the separate ESWT or KT treatment have a better effect based on ultrashort wave and stringing treatments.
Therefore, this study aimed to explore the clinical effect of ESWT combined with KT in treating PF based on ultrashort wave therapy and stringing to provide a reference for PF treatment. Thus, ESWT combined with KT was hypothesised to be more effective in treating PF than a single treatment.
Materials and methods
Participants
The study was approved by the Human Experimental Ethics Committee of Southwest University of Science and Technology (XKD-2020.12). Confirmed PF patients were treated in the Rehabilitation Department of the Affiliated Hospital of the authors’ school from January 2021 to May 2022.
Inclusion criteria
Patients were included in this study if they comply with the clinical diagnostic criteria of PF. Patients typically report that is often worse with their first steps in the morning or after a period of inactivity. With the gradual increase in activity, the pain tends to lessen but worsens towards the end of the day with an increased duration of weight-bearing activity. There is often a localised area of maximal tenderness over the anteromedial aspect of the inferior heel [5, 6, 8]; their disease course is
Exclusion criteria
Patients were excluded from the study if their ankle and lower leg had a history of surgery, trauma and arthritis; they have serious medical diseases (such as haemorrhagic diseases, cardiovascular and cerebrovascular dysfunctions and multiple neuropathies), foot skin ulcer, soft-tissue infection or skin damage; and their skin is allergic to KT.
This study considered 4 (number of groups)
Basic information of the study participants
Basic information of the study participants
Note: ETG: Extracorporeal shock wave therapy group, KTG: Kinesio tape group, CTG: Combination treatment group, CG: Control group.
Participant selection flow diagram. Note: ETG: Extracorporeal shock wave therapy group, KTG: Kinesio tape group, CTG: Combination treatment group, CG: Control group.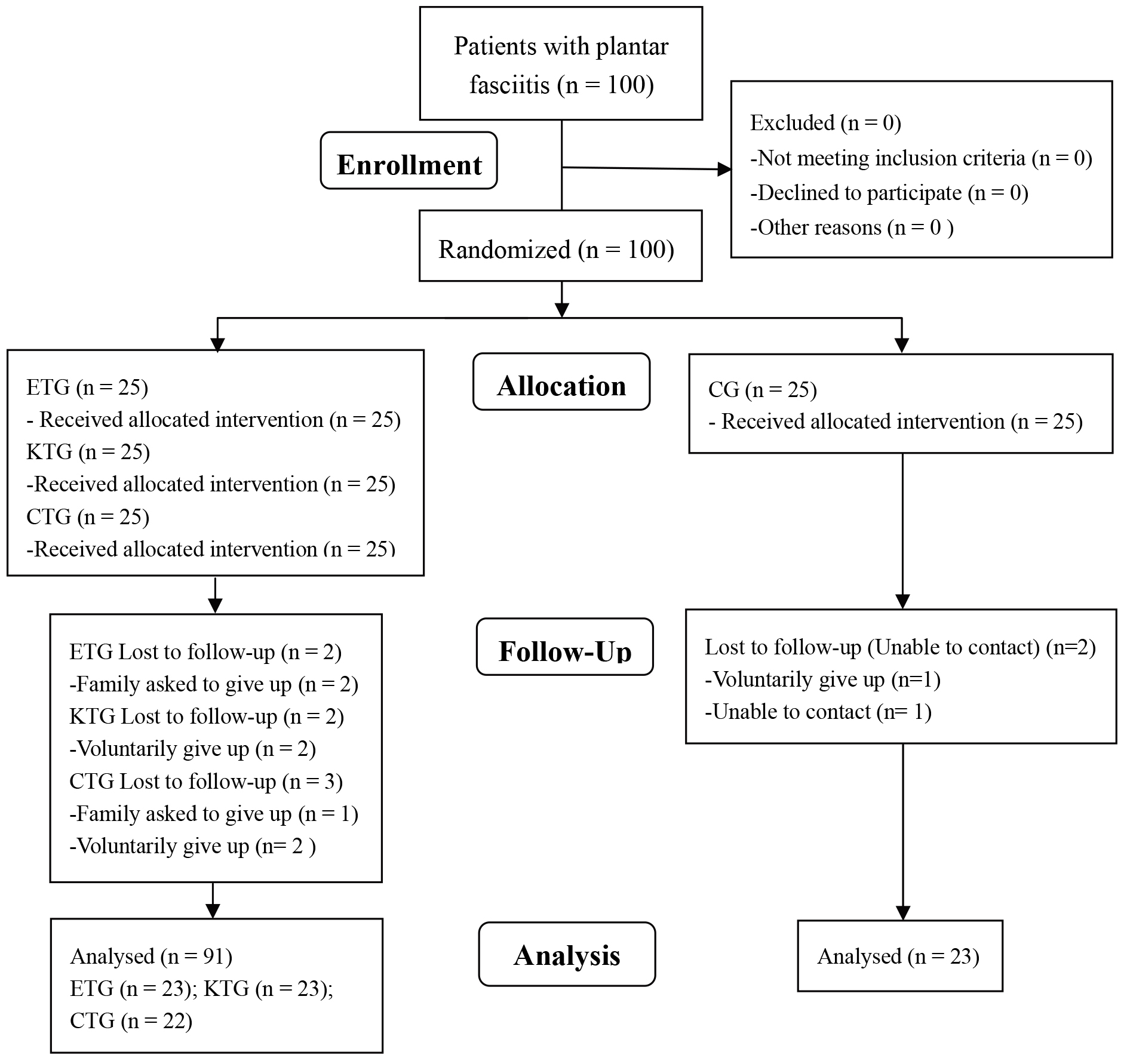
All patients with PF received unified treatment (ultrashort wave therapy, stretching and the same health education). CG only received unified treatment. Meanwhile, ESWT and KT, as well as ESWT and KTT combined modality therapy were additionally provided in ETG, KTG and CTG, respectively. During the treatment, the groups did not receive additional treatment (such as oral analgesics and therapeutic insoles). Ultrashort wave (Dajia Company, Shantou, China; model: DL-C-M). Two electrodes were placed relatively 2–3 cm away from the foot. The dose was adjusted to grade II micro-caloric and the single treatment lasted for 15 min [3].
Referring to the previous treatment plan for stretching [27, 28], the therapist assisted the patients to perform plantar fascia traction and triceps stringing. (1) For plantar fascia stringing, the patient was placed in a prone position and the affected knee joint was bent at 90
In addition, for ESWT (Swiss EMS, Nyon, Switzerland; model: Dolor Clast, 10 mm radial probe), the patient was placed in the prone position, with feet extended over the examination table and knee and hip joints in a neutral position. Then, the extracorporeal shock wave probe was applied to the lower segment of the calcaneus using the ultrasonic gel as a coupling medium. The target area was the maximum tenderness area in the medial calcaneus, without local anaesthesia. The parameters for a single treatment were as follows: frequency of 11 Hz, pressure of 2–3 bars and the number of shocks of approximately 2000 [29]. The treatment was conducted two times a week, eight times in total.
For the first layer (sensory input and spatial taping) of KT (Flitter Company, Chongqing, China; model: F10702/3, 5 cm
Kinesio tape treatment.
Visual analysis scale (VAS): After 4 weeks of treatment at baseline, all patients with PF were assessed for the pain degree of the plantar at the first step when they got up in the morning. A 100 mm line was printed on white paper and the patients were informed that 0 mm and 100 mm indicated painless and painful, respectively. The subjects drew a vertical line on the horizontal line based on their subjective feelings and the corresponding length was the pain score (0–10 points). The higher the score was, the more evident the pain. This measurement method has been confirmed in previous studies [31, 32].
Plantar fascia thickness (PFT): The same experienced ultrasound doctor (3 years of relevant clinical treatment experience) used the Voluson E6 ultrasonic instrument (GE, USA; 11L-D high-frequency probe) to measure the PFT of all patients with PF. The patient was placed in a prone position, with the foot hanging down to the bed edge and the ankle joint in a neutral position. The probe was placed on the medial side of the foot calcaneus and slightly moved along the long axis of the foot for adjustment to display the plantar fascia. The joint of the calcaneus and plantar fascia was the measurement site [33]. Three pictures were taken each time to reduce error and the average value was taken. The higher the score was, the more evident the symptoms.
Changs in the four groups at different points
Changs in the four groups at different points
Note: ETG: Extracorporeal shock wave therapy group, KTG: Kinesio tape group, CTG: Combination treatment group, CG: Control group; VAS: Visual analogue scale, PFT: Plantar fascia thickness, AOFAS: American orthopaedic foot and ankle society. Intra-group comparison at 0 weeks and 4 weeks:
American Orthopaedic Foot and Ankle Society (AOFAS) score: The foot function of all patients with PF was evaluated, including nine items of patient self-filling and physician’s examination as follows: pain, function and autonomous activity, support, maximum walking distance, ground walking, abnormal gait, fore and aft activity (flexion and extension), hind foot activity (varus and valgus) and ankle hindfoot stability (varus, varus and valgus) and foot force line, with a total score of 100 points [34]. The higher the score was, the lighter the symptom.
The baseline and 4-week test data of the four groups were processed on SPSS 20.0 and expressed as mean
Results
The test data of the four groups are shown in Table 2. A Shapiro-Wilk test showed that all measured indicators were normally distributed (
Then, a comparison between groups was conducted 4 weeks later.
Comparisons within groups were performed at weeks 0 and 4.
Discussion
This study aimed to explore the clinical efficacy of ESWT combined with KT in treating PF based on ultrashort wave therapy and stringing to provide a reference for PF treatment. Results showed that ESWT and KT could improve the foot pain and function of patients with PF and the combined modality therapy was found to be more effective. Moreover, ESWT and combined treatment showed a positive effect on patients’ PFT. However, KT had limited influence on PFT.
ESWT
This study showed that the VAS score and PFT were significantly reduced by 41.7% and 8.4%, respectively, and the AOFAS score was significantly increased by 32.9% when ESWT was added based on ultrashort wave therapy and stringing. As a treatment method, ESWT provides high-amplitude sound waves on the required parts of the human body. Hence, it is widely used in treating PF and its efficacy has been confirmed [11, 12, 25, 26, 37, 38]. Mishra et al. [37] conducted ESWT intervention on 60 patients with PF and found that it could effectively improve the pain, PFT and functional activities of patients. Chew et al. [38] also found that ESWT significantly improved the VAS score, PFT and AOFAS score of patients with PF. The findings of these studies are consistent with those of the present study. However, some studies revealed different opinions. A double-blind randomised controlled trial found that a moderate dose of ESWT seems to have no therapeutic effect on patients with PF [39]. In addition, a systematic evaluation and meta-analysis found that ESWT is beneficial to the treatment of plantar pain, however, its efficacy is limited [40]. The reason for these varying results may be the different intensities or times of ESWT intervention.
Extracorporeal shock wave therapy positively affects PF treatment and its mechanism may be as follows: when EWST enters the human body, different mechanical stresses are generated at the interface of different acoustic impedance tissues because of the different media it contacts, manifested in different tensile stresses and stress effects on tissues [41]. Amongst them, tensile stress could induce interstitial loosening and promote microcirculation and the stress effect could promote cell elastic deformation and increase cell oxygen uptake [41]. Nevertheless, the negative wave band pressure of the pulse tail of the shock wave could cause a cavitation reaction, which is conducive to unblocking occluded micro-vessels and loosening the adhesion of joint soft tissue [42]. Local high-intensity EWST could produce super stimulation on nerve endings, block the transmission of painful information to the cerebral cortex and cause changes in free radicals around cells to release pain-inhibiting substances, thereby achieving an analgesic effect [42]. Shock waves could promote local blood circulation and change the permeability of the local cell membrane of the tissue by promoting the generation of relevant growth factors, thereby speeding up tissue metabolism, reducing the inflammatory reaction of the affected area and accelerating tissue healing [43]. In addition, the plantar fascia may be considered a tendinous structure. Tenocytes may convert mechanical stimulation into a biochemical response, thereby leading to the release of growth factors and cellular adaptation. After ESWT treatment, the tendon was remodelled or degenerated by regulating anabolic and catabolic genes. Therefore, EWST could have a good therapeutic effect on the pain tissues of patients with PF
Kinesio tape
This study showed that in addition to ultrashort wave therapy and stretching, KT therapy could significantly reduce the VAS score by 35.8% and increase the AOFAS score by 22.6%. However, it showed no positive effect on PFT.
KT is a special tape that could produce a constant shear force [21]. In treating the soft-tissue injury with KT, the location, direction and tension of the ligation are often selected based on the principles of motion analysis and biomechanics. The direction of tension is generally parallel to the muscle fibre and the strength of tension depends on the intensity of the stimulus required and the restrictions on the activities of muscles, tendons and ligaments [17]. Nevertheless, at present, no uniform standard is available for KT binding method but the positive effect on patients with PF has been confirmed [22, 23, 24, 25, 45, 46]. Results of the present study showed that the heel pain and function of patients with PF were improved by KT treatment. Podolsky et al. [45] found that KT effectively treated patients with PF in the short term. In addition, Van et al. [46] found that KT could reduce the pain of patients with PF in a jumping test. The findings of these studies are consistent with the results of the present study. However, some studies provided different opinions. In a systematic evaluation, KT showed a slight effect on the treatment of patients with PF, which may have no clinical significance [47]. Thus, this finding may be related to the individual differences of patients and the different methods of ligation.
Moreover, KT has a positive effect on the treatment of PF and its mechanism may be as follows: given that KT is flexible, it could increase the gap between skin and muscle, promote blood circulation to relieve pain [13, 14] and control the tension on the plantar fascia through the retraction force of the patch towards the heel [18]. The plantar fascia of PF patients is supported by the width of KT and large tension and the stress attachment point of plantar fascia moves forward to avoid further damage to reduce the degree of pain after daily activities and improve the foot function status [14]. In addition, KT relaxes tense muscles, increases local sensory input, improves proprioception, stimulates skin mechanoreceptors with pressure and tension on the skin and enhances joint position sense and motion sensing, thereby improving joint stability [5, 26].
Combined treatment
This study showed that the effect of combined treatment in CTG’s pain degree and AOFAS score was significantly improved as compared with that before treatment; it was better than that of the single treatment (in ETG, KTG and CTG, the VAS scores decreased by 41.7%, 35.7% and 58.0%, respectively, whereas the AOFAS scores increased by 32.9%, 22.6% and 51.3%, respectively). In addition, combined treatment decreased PFT by 12.9%.
Stringing improves the flexibility of the Achilles tendon and plantar fascia of the affected foot and expands the range of ankle dorsiflexion [27]. With assistance from ESWT treatment, stringing could further relieve pain and improve joint activity. However, ESWT causes micro damage to local tissues through acute and rapid mechanical action and then induces reconstruction to increase blood supply. The affected part may have local ecchymosis, hematoma, acid swelling and other discomforts. Meanwhile, increasing KT could cause skin wrinkles, change the space between local skin and muscle by pulling, promote lymph and blood circulation and alleviate the swelling of subcutaneous soft tissues [28, 29], thereby helping to improve the adverse reactions after ESWT treatment. Furthermore, it demonstrated a better therapeutic effect on pain and motor dysfunction caused by PF.
Ultrasound examination results often indicate specific changes in patients with PF, such as PFT increase and calcification [13]. In the present study, the PFT of the affected foot of the four groups significantly increased before treatment, consistent with the result of a previous study [14]. A notable detail is that KT had no statistically significant effect on patients’ PFT, whereas ESWT and combined treatment had a positive effect. This finding indicated that the treatment of 4 weeks may be a better strategy than KT.
However, this study has some limitations. Firstly, the intervention time was only 4 weeks and the period was short, which may have limited the research results. Secondly, a personalised treatment plan based on the patient’s age, weight, disease course and foot structure characteristics was not formulated. Finally, changes in biomechanical parameters, such as plantar pressure and gait, were not evaluated. Thus, this limitation is expected to be studied in the near future.
Conclusions
Based on ultrashort wave treatment and stretching, ESWT and KT treatment could improve the foot pain and function of PF patients and combined modality therapy was found to be more effective. ESWT and combined treatment had a positive effect on patients’ PFT, whereas single KT treatment had a limited effect.
Ethics statement
This study was approved by the Human Experimental Ethics Committee of Southwest University of Science and Tchnology (XKD-2020.12). Before the assessment, every participant received the same detailed information about the testing procedure. Every participant signed the informed consent.
Funding
This research was funded by a grant from the Key Projects of Humanities and Social Science of Sichuan Provincial Department of Education (Jing Zhao, 18SA0271).
Author contributions
Conceptualization and design: J. Z., Y. F. J.; Data Collection: J. Z., Y. F. J.; Interpretation: J. Z., Y. F. J.; Writing-original draft: J. Z., Y. F. J.; All authors read and approved the final version of the manuscript.
Footnotes
Acknowledgments
The authors are particularly grateful to everyone who helped them with the article.
Conflict of interest
No conflicts of interest have been reported by the authors or by any individuals in control of the content of this article.