
Abstract
BACKGROUND:
Despite being used as a program of postoperative rehabilitation, few randomized controlled trials have compared the effectiveness of postoperative exercise based on gait analysis in patients with lumbar spinal stenosis (LSS).
OBJECTIVE:
To investigate the effectiveness of postoperative exercise based on gait analysis in patients with LSS and to compare it with the effectiveness of conventional exercise.
METHODS:
This was a double-blind, randomized clinical trial. Sixty-eight participants with LSS were randomly assigned to one of two groups. After receiving a standardized surgical procedure, the observation group received exercises based on 3-D gait analysis, and the control group received empirical physiotherapy containing 4 basic interventions. Both groups took a one-hour session twice daily for 2 weeks. The Oswestry Disability Index (ODI) scale and the Visual Analog Scale (VAS) were measured before and 2 weeks and 6 months after intervention. The gait indicators were measured before and 6 months after intervention.
RESULTS:
At baseline, there were no significant differences in the ODI, VAS or absolute symmetry index (ASI) of the gait variables between the observation group and the control group. However, at 6 months, pain intensity, walking, standing, social life and summary scores of ODI and VAS of the leg demonstrated significant differences (
CONCLUSIONS:
The postoperative rehabilitation scheme based on gait analysis resulted in significant short- to medium-term improvements in pain intensity, walking, standing, social life and the summary score of ODI, VAS of leg and symmetry of stride length, hip flexion, knee flexion and ankle dorsiflexion compared with empirical exercise in patients with LSS.
Introduction
Low back pain is one of the most common musculoskeletal symptoms combined with disability and is a leading contributor to disease burden in both developed and developing countries [1, 2]. It occurs when the dynamic equilibrium in the spinal structure becomes unbalanced, often in situations where spinal canal narrowing develops gradually because of enlarged osteophytes, thickened ligamenta flava, degenerative arthritis and disc herniation, which is defined as lumbar spinal stenosis (LSS) [3]. Radiographic findings of LSS are highly prevalent among people older than 60 years of age and can be as high as 80% in specific populations [4]. Because the pain generated from increased pressure on the nerves within the stenosed segment can be decreased by increasing the cross-sectional area of the spinal canal at the level of stenosis, lumbar decompression surgery may be recommended for patients with refractory symptoms [5]. Nevertheless, approach-related problems and spinal instability may occur that can negatively affect the results of open operations [6]. As a representative minimally invasive operation, the percutaneous endoscopic decompression (PED) technique has shown good clinical results for LSS, and the advantages of this technique have been documented, such as minimal paravertebral muscle damage, no need for excessive bone removal or general anesthesia, low cost and early return to daily life [7, 8, 9]. Clinical symptoms of intermittent claudication, pain in the buttocks or lower extremities and low back pain seem to be improved by PED based on less muscular interference [10, 11], but functional problems with imbalance, weakness of the muscles of the lower extremities, supermarket gait and sensory loss are still commonly left and easily ignored by surgeons [12]. Meanwhile, some studies have reported that surgical outcomes are not ideal and that a sizeable proportion of patients do not regain good function [8, 13]. This is because spinal stenosis is a chronic mechanical change that may cause many movement disorders, such as excessive spinal and hip flexion (this posture can expand the spinal canal and alleviate pain), lower limb weakness (less walking because of intermittent claudication), hypesthesia (compression of nerve root), asymmetry and instability during walking, and abnormal gait, and these disorders can also lead to low back pain [14]. This is clearly a vicious cycle that will negatively affect the treatment results on LSS if dysfunctions are overlooked.
Aiming for the above present dysfunctions, some therapists have put forward a number of exercise interventions to improve function and restore spinal stability [15]. However, objective indications and evidence are currently insufficient for therapists to determine the most suitable exercise projects, although clinical experience suggests that some form of exercise intervention may be beneficial for the postoperative effect on LSS [16]. To augment objectivity, gait analysis has been extensively employed in hemiplegic rehabilitation for exercise assessment and guidance [17, 18]. Nevertheless, no applications of gait analysis exist for evaluating and guiding lumbar postoperative rehabilitation. Therefore, this study planned to evaluate postoperative motor dysfunctions with 3-D gait analysis in patients with LSS and provide specific exercises to cope with these dysfunctions. We investigated whether exercise based on detailed evaluation was more effective than conventional exercise for patients with postoperative LSS.
Materials and methods
Study design
This study was a double-blinded, 2-arm, randomized controlled trial (RCT) comparing the effectiveness between postoperative exercise based on 3-D gait analysis (observation group) and conventional postoperative exercise (control group) in patients with LSS after PED. It took place between November 2017 and November 2019 and presented the main outcome of the Oswestry Disability Index (ODI) and the secondary outcomes of the Visual Analog Scale (VAS) and index of gait analysis.
Approval and registration
This trial was registered with the ClinicalTrials.gov database (ChiCTR-INC-17013401) and approved by the Ethics Committee of Navy General Hospital (2017011). Patients provided written informed consent prior to randomization.
Enrollment of participants and study flow.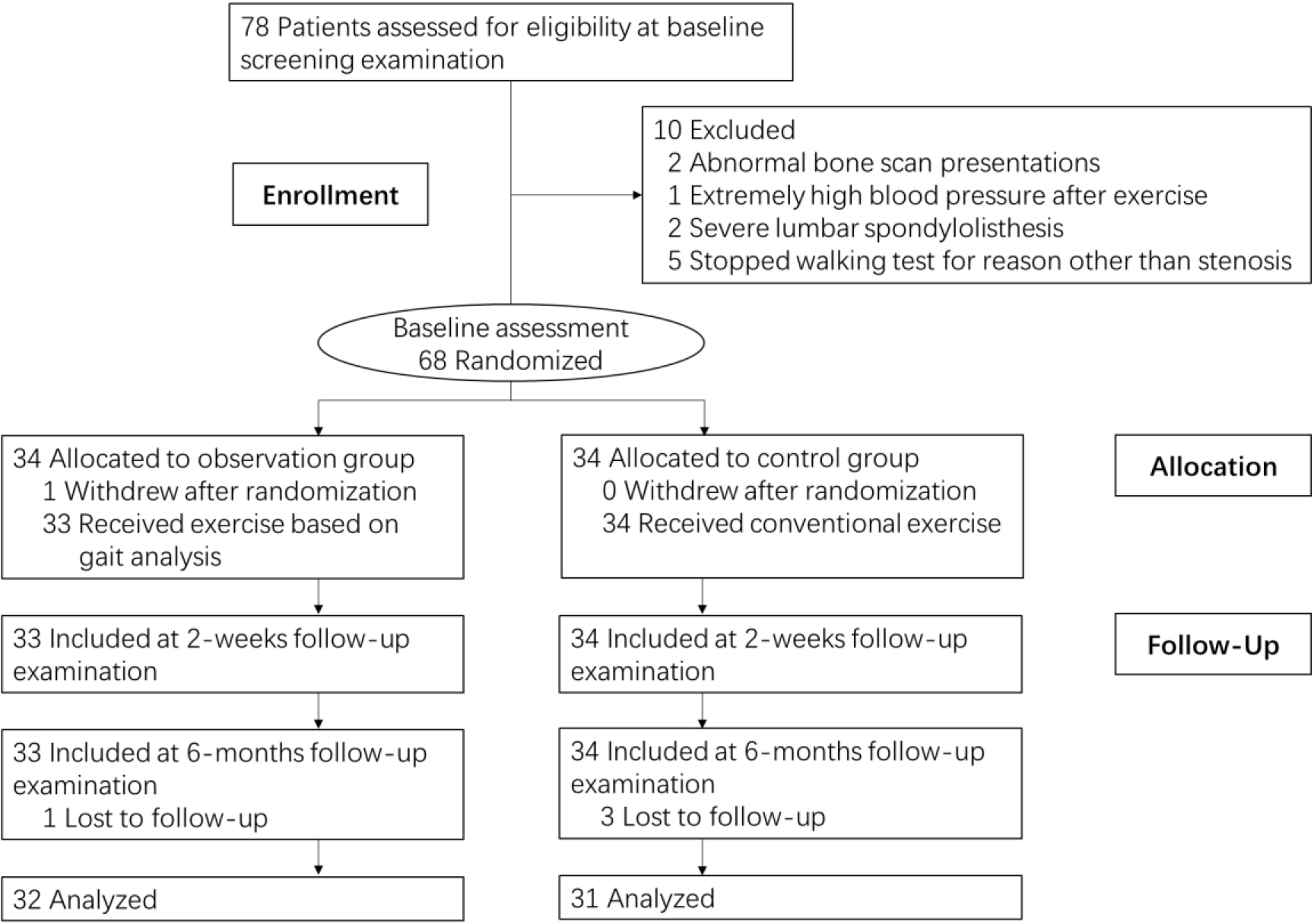
This trial was designed in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines for reporting randomized controlled trials [19]. The trial protocol is available in Fig. 1.
Participants
Patients with LSS were referred to the outpatient clinic in the Pain and Rehabilitation Medicine Centre of PLA General Hospital by general practitioners, rehabilitative physicians and orthopedic surgeons in the surrounding area. All participants were screened with radiographs, computerized tomography (CT) and magnetic resonance imaging (MRI) and underwent clinical examinations by a specialist in physical medicine and rehabilitation and an orthopedic surgeon.
Inclusion and exclusion criteria
All potential participants were screened to determine their eligibility according to the following inclusion and exclusion criteria. For inclusion, patients were 40–80 years of age (64.5
Exclusion criteria were previous surgery for spine, cauda equina symptoms, inability to complete the walking test, inability to engage in physical exercise, history of metastatic cancer, severe peripheral artery disease, severe spondylolisthesis and lower limb joint degeneration.
Randomization
Randomization was used with sealed envelopes prepared for each randomization block. A medical doctor who was not a contributor to the study performed the randomization process and assigned patients to either the observation group or the control group after screening for eligibility. Patients, the surgeons who performed the PED procedure and the two physiotherapists who performed the measurements at baseline and follow-up were unaware of the treatment allocation.
Treatment arms
All included patients received hospital treatments following the treatment protocol, which included perioperative nursing, PED surgical procedures, health education and postoperative drug therapy. Four physiotherapists were trained in the same treatment protocol, with each participant randomly assigned to 1 of these 4 physiotherapists. Patients in the control group received the above usual medical intervention and one-hour conventional physiotherapy sessions twice daily for 2 weeks containing 4 basic interventions: (1) muscle strength training for the low back and lower limbs, such as active back extension in the prone position, active hip flexion in the supine position and glute bridge exercise; (2) deep spinal muscle activation training, such as cat-camel and bird-dog exercise; (3) spinal stability training, such as seated active balancing exercise on a Swiss ball; and (4) joint mobilization, such as lumbar distraction mobilization.
Main exercises based on gait analysis in the observation group
Main exercises based on gait analysis in the observation group
Participants in the observation group underwent physiotherapy based on 3-D gait analysis twice daily for two weeks, with each exercise session lasting approximately one hour. All other procedures were identical to those of the control group, as detailed in Table 1.
Quality control was maintained through the WeChat app and outpatient follow-up after discharge, which included restrictions such as no massage for over three days, refraining from self-administered painkillers unless intolerable, limiting sitting to a maximum of half an hour, and avoiding gym exercises for six months.
Abnormal gait: Gait data deviated from the range of walking parameters observed in healthy individuals, with normal data obtained from relevant literature [20, 21].
The outcomes, including patient-reported outcomes and objective outcomes, were collected by blinded physiotherapists at baseline and 2 weeks and 6 months after inclusion (Fig. 1). The primary outcome was the ODI [22], and the secondary outcomes included VAS [23] of pain and gait indicators. The details of the measurement method are described by Wang et al [24]: a three-dimensional motion capture system with force plate measurement (KinemaTracer, Kissei Comtec Co., Ltd., Matsumoto, Japan) was utilized. A simplified set including 14 markers was placed on both sides of the shoulder, elbow, pelvis, hip, knee, ankle, and 5th metatarsal head. Before measurement, the patients walked on the treadmill to acclimate to treadmill gait for 1 min. After achieving a steady state, data were collected for 20 s, and data for at least five complete gait cycles were collected from each subject. Videos were recorded at a sampling frequency of 60 Hz and a measurement time of 20 s. Stride frequency, gait velocity, stride length and angle of hip flexion angle, knee flexion and ankle dorsiflexion were recorded during this period. Meanwhile, the asymmetry degree between the right (X
The ODI [22] was used to measure perceived functional disability levels due to chronic low back pain and demonstrated reliability [26]. This self-administered, reliable and valid questionnaire consists of 10 items, each having a score of 0 to 5. The total ODI scores range from 0 (no disability) to 50 (severe disability). This questionnaire was adjusted moderately in the study.
The VAS, demonstrated to be reliable [22, 27], has a horizontal, 100-mm-long line, with “no pain” recorded on the left side (score: 0) and “pain as bad as it could be” on the right side (score: 10). Patients were asked to place a mark on the line that corresponded to their current level of pain. The VAS score was then determined by measuring the millimeters between the left end point and the point marked by the patient.
Sample size determination and statistical analysis
The sample size was calculated based on the previously determined minimum clinically important difference (MCID) of 12.8 points for the main outcome measure (ODI) [28] and assuming a standard deviation of 2.72 [29]. With the power set to 0.8 and alpha at 0.05, a minimum of 31 patients per group was required to achieve significance using a two-tailed Student’s t test. Due to the possibility of dropouts, 78 participants were eventually recruited.
Statistical analysis was performed using SPSS software (IBM Crop., USA), version 20 for Windows. The demographic and baseline characteristics between groups were compared by one-way ANOVA for parametric variables and the chi-square test for nonparametric variables. The outcomes between groups were compared by Student’s t test for parametric variables and the Mann-Whitney U test for nonparametric variables. All statistics were conducted using per-protocol and intention to treat analyses. All statistical tests were two-tailed, and the threshold for statistical significance for all tests was
Results
In total, 68 participants were allocated to the observation group (34 [50.0%]) and control group (34 [50.0%]), and 63 participants were analyzed. The groups were relatively balanced on all characteristics except the history of NSAIDs (Table 2). The mean (SD) age was 64.3 (9.0) years, ranging from 48 to 81 years. Of 63 participants, 35 (55.6%) were male, 7 (11.1%) had a history of local injection and 9 (14.2%) had medical comorbidities, including hip (1 [1.6%]), knee (7 [11.1%]) and ankle osteoarthritis (1 [1.6%]). At baseline, the mean (SD) VAS scores were 6.6 (0.9) for the back and 5.3 (0.8) for the leg (Table 2).
Characteristics of participants
Characteristics of participants
VAS: Visual Analogue Scale, NSAIDs: Nonsteroidal Antiinflammatory Drugs.
At baseline, there were no significant differences in 10 items of ODI and VAS between groups (
Comparison of ODI and VAS between two groups at baseline, 2 weeks and 6 months
ODI: Oswestry Disability Index, VAS: Visual Analogue Scale.
Comparison of ASI of gait indexes between and in two groups at baseline, 2 weeks and 6 months
Note: ASI, Absolute Symmetry Index;
The ASI of stride frequency, gait velocity, stride length, hip flexion, knee flexion and ankle dorsiflexion before and after the intervention improved significantly in the observation group (
To the best of our knowledge, no randomized con-trolled trials (RCTs) have compared the effectiveness of postoperative exercise informed by gait analysis in patients with LSS. As shown in Table 3, this randomized, controlled trial, which included 68 patients with LSS, revealed a daily functional benefit 6 months after treatment of adding exercise based on gait analysis to PED. In addition, compared with conventional physiotherapy, the more accurately advanced physiotherapy with gait analysis plus PED was associated with better symmetrical joint motion but not with less ASI of stride frequency or gait velocity. Approximately
The concept of minimally invasive decompression surgery, such as PED, has been expanding over the past decade. Although it can minimize damage to deep musculature in the spine, longstanding movement disorders resulting from LSS still need to be solved by rehabilitation programs following surgery, and a considerable number of patients do not regain ideal function by surgery alone [30, 31]. Furthermore, some studies have suggested that exercise or rehabilitation intervention after surgery can be beneficial for the improvement of activity, and the need for such interventions may be even greater for elderly individuals who are more likely to have poor preoperative functional status [31, 32]. Dynamic lumbar stabilization exercises, deep muscle activation, muscle strength increase and joint motion exercises may be recommended to patients following spinal surgery due to their benefits in reducing pain, increasing mobility and stability and ensuring faster return to work periods [33, 34, 35]. Additionally, patients who engage in exercise after spinal surgery have better mental health and spine-specific recovery trajectories than those who do not [31].
However, the postoperative rehabilitation program following spinal surgery is variable, with major differences reported among medical institutions in the type and indication of rehabilitation provided, and little consensus has been reached on what constitutes an appropriate rehabilitation program, why a program should be used, how intense it should be, how long it should be delivered, or how frequently [37, 38]. Overall, at present, the design of rehabilitation prescriptions is still mainly based on clinical experience, and evidence is currently insufficient for therapists to determine the best rehabilitation program. Therefore, the present study conducted a rehabilitation program according to gait analysis and observed the above effects.
Judging from the ODI scores, it is apparent that the rehabilitation program according to gait analysis was more effective in improving pain intensity, walking, standing and social life than empirical rehabilitation at 6 months. On the other hand, in the observation group, the symmetry of stride length, hip flexion, knee flexion and ankle dorsiflexion were considered to be satisfied, but stride frequency and gait velocity did not decrease at ASI. It is quite possible that we tended to pay much closer attention to the range of motion and muscle strength in gait and ignored other indices that can be difficult to quantify, such as proprioception, core strength and endurance, weight transfer and walking rhythm. Thus, future work is needed in this area to factor in and quantify these issues, but this result showed that a precise and well-founded rehabilitation program may be of value in enhancing functional outcomes and walk stability for postoperative patients. The results also indicated that there were no significant differences in ODI and VAS scores between the two groups at two weeks postoperatively, but considerable differences emerged at six months postoperatively. This phenomenon can be attributed to two factors. First, gait analysis is more reliable than subjective scales. ODI and VAS are considered semi-quantitative evaluation scales, frequently employed in lumbar postoperative assessments, while gait analysis constitutes an objective evaluation tool, despite its equipment requirements. Second, the surgical wound may not have fully healed in the short term following surgery, potentially contributing to the poor results from ODI and VAS. However, two weeks after surgery, the objective gait analysis results revealed noticeable differences, suggesting that the pain may have originated from the wound itself and constituted a self-limiting issue.
Our study has three major limitations. First, it was conducted in a single center, which limits its generalizability. Second, a potential bias could have been present during the initial selection of patients, as the degree and type of intervertebral disc protrusion were different and could not be identified just by symptoms. Finally, the gait index used in this study was carefully chosen for convenient planning of the rehabilitation scheme and comparison among groups but did not entirely reflect patients’ walking capacity. Therefore, there is still a need for further trials to consider other important objective indicators in making rehabilitation plans and striving for consensus in postoperative lumbar exercises. Furthermore, this study didn’t have a blank group due to ethical issue.
Conclusion
In summary, in this randomized trial of patients with postoperative LSS, a rehabilitation scheme based on gait analysis resulted in significant short- to medium-term improvements in pain intensity, walking, standing, social life, the summary scores of ODI and VAS of the leg, symmetry of stride length, hip flexion, knee flexion and ankle dorsiflexion compared with conventional exercise. Therefore, postoperative patients with LSS can benefit from objective physical interventions. Future studies should focus on long-term outcomes and more objective indicators.
Ethical approval
The study was approved by the Ethics Committee of Navy General Hospital (2017011) and registered with the ClinicalTrials.gov database (ChiCTR-INC-17013401).
Funding
This study is supported by the innovaton fund of The Six Medical Center of Chinese PLA General Hospital (CXPY201917) and the fund of training injury prevention (21XLS35).
Informed consent
All participants signed an informed consent form.
Author contributions
Conceptualization and design: Ling Guan, Yuxian Zhong; Data collection: Yuxian Zhong, Guanghao Ma, Minyue Li, Yang Yu; Intervention: Yu Ding, Yuxian Zhong, Bensheng Fu, Guanghao Ma, Hongpeng Cui, Minyue Li, Yang Yu; Writing-original draft: Yuxian Zhong; All authors read and approved the final manuscript.
Footnotes
Acknowledgments
None to report.
Conflict of interest
The authors have no conflict of interest to report.