
Abstract
BACKGROUND:
Many older adults are at risk of sarcopenia, a gradual loss of muscle mass affecting muscle strength and physical function, which can lead to adverse health consequences deteriorating their independence. However, the detection could be delayed due to the requirement of many measures, including a complex imaging modality. Thus, an exploration for a practical community- or home-based measure would be helpful to identify at-risk older adults and begin the timely management.
OBJECTIVE:
To explore the ability of the upper limb loading during a seated push-up test (ULL-SPUT) to determine the presence of sarcopenia in community-dwelling older adults.
METHODS:
Older adults (
RESULTS:
Data from standard measures indicated that 44 participants had sarcopenia. The ULL-SPUT index of
CONCLUSION:
The ULL-SPUT index could be used to screen and monitor older adults with sarcopenia in various clinical, community, and home settings. This practical measure may be accomplished using a digital bathroom scale on a hard, even surface. Outcomes would identify an adult who should undergo further confirmation of sarcopenia through standard measures or the initiation of timely management to promote treatment effectiveness.
Introduction
Sarcopenia can be found in up to one-third of older adults. It is a condition characterized by the loss of skeletal muscle mass (SMM), as determined using the appendicular skeletal muscle mass (ASM) index, combined with low muscle strength and/or poor physical performance due to several factors, including advancing age [1, 2, 3, 4]. The loss of these three components results in an increasing risk of physical disability, falls, osteoporosis, metabolic syndromes, and immune deterioration. Thus, apart from the effects of age-related body system decline, sarcopenia additionally enhances the risk of major adverse health consequences affecting mobility, morbidity, independence, hospitalization, and mortality, as well as quality of life of older people [5, 6, 7, 8]. Therefore, it is highly recommended that the presence of sarcopenia be identified early, while people are still functioning independently, to enable timely and effective interventions and periodic follow-up to prevent or minimize adverse health consequences and disability, particularly in this upcoming super-aged society [3, 9].
The Asian Working Group for Sarcopenia (AWGS) reported in its 2019 consensus update on sarcopenia diagnosis and treatment that the detection of sarcopenia involves the assessment of the aforementioned three components [3]. Some of these assessments require a complex imaging modality, such as dual-energy X-ray absorptiometry (DXA), magnetic resonance imaging, and computed tomography; other measurements for muscle strength and physical performance including the handgrip strength test (HG) and the 10-meter walk test (10MWT) [3, 4]. The former three imaging tests are often accessible only in a hospital setting, whereas the ability to administer the latter two tests may be limited in settings without the necessary equipment and available space. Therefore, a practical alternative measure to enable the detection of sarcopenia is needed, especially in the current era of the paradigm shift toward community- and home-based healthcare services.
Recent studies have found the benefit of the upper limb loading during a seated push-up test (ULL-SPUT) to reflect components that are involved in determining sarcopenia, including the SMM, muscle strength, and mobility of clinical populations and older adults [10, 11, 12, 13]. The present researchers hypothesized that the ULL-SPUT could be used to identify older adults with sarcopenia. However, with different rates of aging-related system decline between the sexes [12, 14], the present researchers further hypothesized that male and female participants would have different criteria for sarcopenia detection. Therefore, this study explored the ability of ULL-SPUT to identify older males and females with sarcopenia as verified using data from standard measures.
Materials and methods
Participants
This cross-sectional study was conducted in com-munity-dwelling adults aged 65 years and older via direct contact with community leaders. The inclusion criteria were a body mass index (BMI) of
Research protocols
Eligible participants were interviewed and assessed for their demographics (age, bodyweight, height, and underlying diseases, if any). Then they were assessed for the outcomes of the study using standard measures for sarcopenia (i.e., HG, 10MWT and DXA) and the ULL-SPUT.
Handgrip strength test
The HG strength test is a valid measure that is commonly used to reflect global muscle strength and functional mobility (
10-meter walk test
This test is an excellent test-retest reliability measure (intraclass correlation coefficient
Dual-energy X-ray absorptiometry
In this study, DXA, a standard excellent reliability (intraclass correlation coefficient
Data from these three measures (HG strength, walking speed, and ASM index) were used to identify participants with and without sarcopenia according to the criteria from the 2019 AWGS updated consensus as showed below [3]:
The upper limb loading during a seated push-up test protocol. (A) Starting position; (B) Position while lifting the body upward.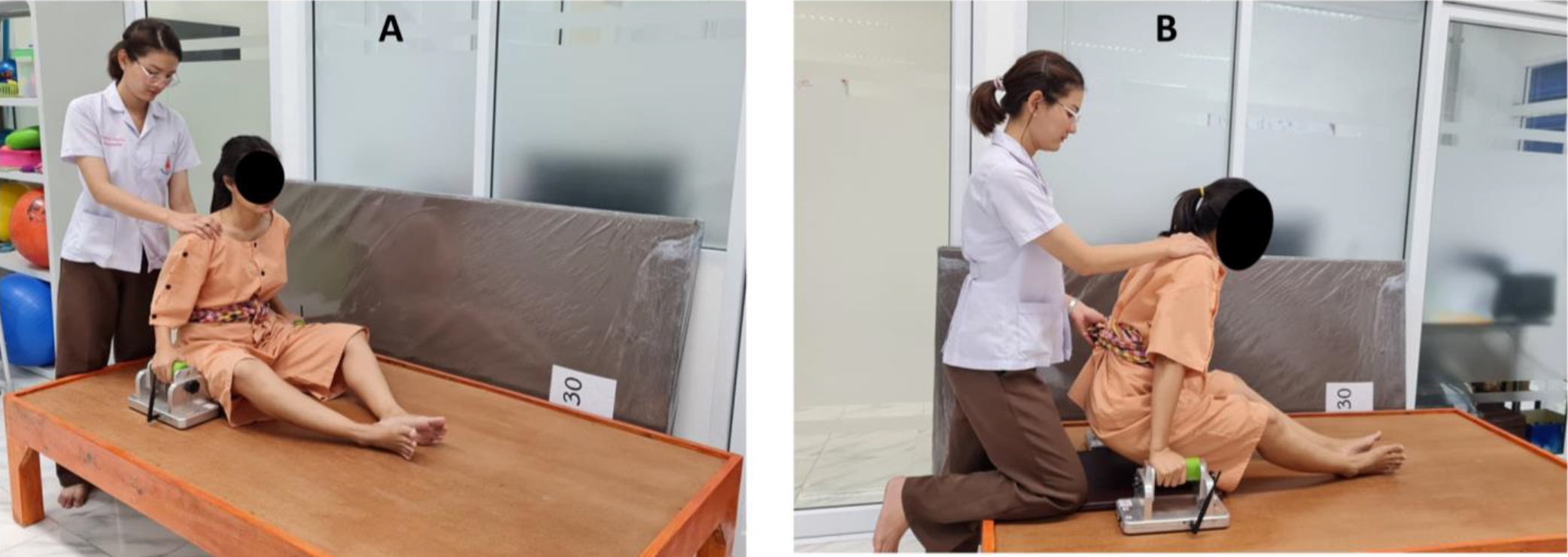
Previous studies reported that the ULL-SPUT of older adults significantly correlated with lean body mass (LBM;
Statistical analysis
Descriptive statistics were used to explain the participants’ demographics and findings of the study, separately for male and female participants. Participants with no sarcopenia and possible sarcopenia were assigned to the non-sarcopenia group, and those with sarcopenia and severe sarcopenia were assigned to the sarcopenia group. The differences between the groups of each sex were compared using the independent samples
| Variable | Female participants ( |
|
Male participants ( |
|
||
|---|---|---|---|---|---|---|
| Non-sarcopenia ( |
Sarcopenia ( |
Non-sarcopenia ( |
Sarcopenia ( |
|||
| Age (years)a | 73.2 |
80.4 |
|
74.9 |
78.1 |
0.053 |
| Weight (kg)a | 53.1 |
41.4 |
|
62.6 |
53.9 |
|
| Height (m)a | 1.5 |
1.5 |
0.122 | 1.6 |
1.61 |
0.272 |
| Body mass index (kg/m2)^a | 23.9 |
19.2 |
|
24.4 |
20.7 |
|
| Walking deviceb | 0.032* | 0.454 | ||||
| No | 36 (81.8) | 10 (55.6) | 20 (90.9) | 25 (96.12) | ||
| Yes | 8 (18.2) | 8 (44.4) | 2 (9.1) | 1 (3.9) | ||
| Cane | 8 (18.2) | 6 (33.3) | 2 (9.1) | 1 (3.9) | ||
| Walker | 0 (0.0) | 2 (11.1) | 0 (0.0) | 0 (0.0) | ||
| Medical conditions: number (%) | 0.175 | 0.961 | ||||
| No | 23 (52.3) | 6 (33.3) | 10 (45.5) | 12 (46.2) | ||
| Yes (1–4 medical conditions) | 21 (47.7) | 12 (6.7) | 12 (54.6) | 14 (53.9) | ||
| Medication useb | 0.212 | 0.976 | ||||
| No | 25 (56.8) | 7 (38.9) | 9 (40.9) | 11 (42.3) | ||
| 1–3 | 18 (40.9) | 9 (50.0) | 10 (45.5) | 12 (46.2) | ||
| 4 and more | 1 (2.3) | 2 (11.1) | 3 (13.6) | 3 (11.5) | ||
Outcomes of male and female participants with and without sarcopenia
Participants
A total of 110 community-dwelling older adults (62 females) with an average age of approximately 77 years and a normal BMI completed the study (Table 2). Data from standard measures indicated that 40% of participants (
The data distribution, cutoff score, sensitivity, specificity, and areas under the receiver operating characteristic curves (AUC) of the upper limb loading during a seated push-up test (ULL-SPUT) index of the participants.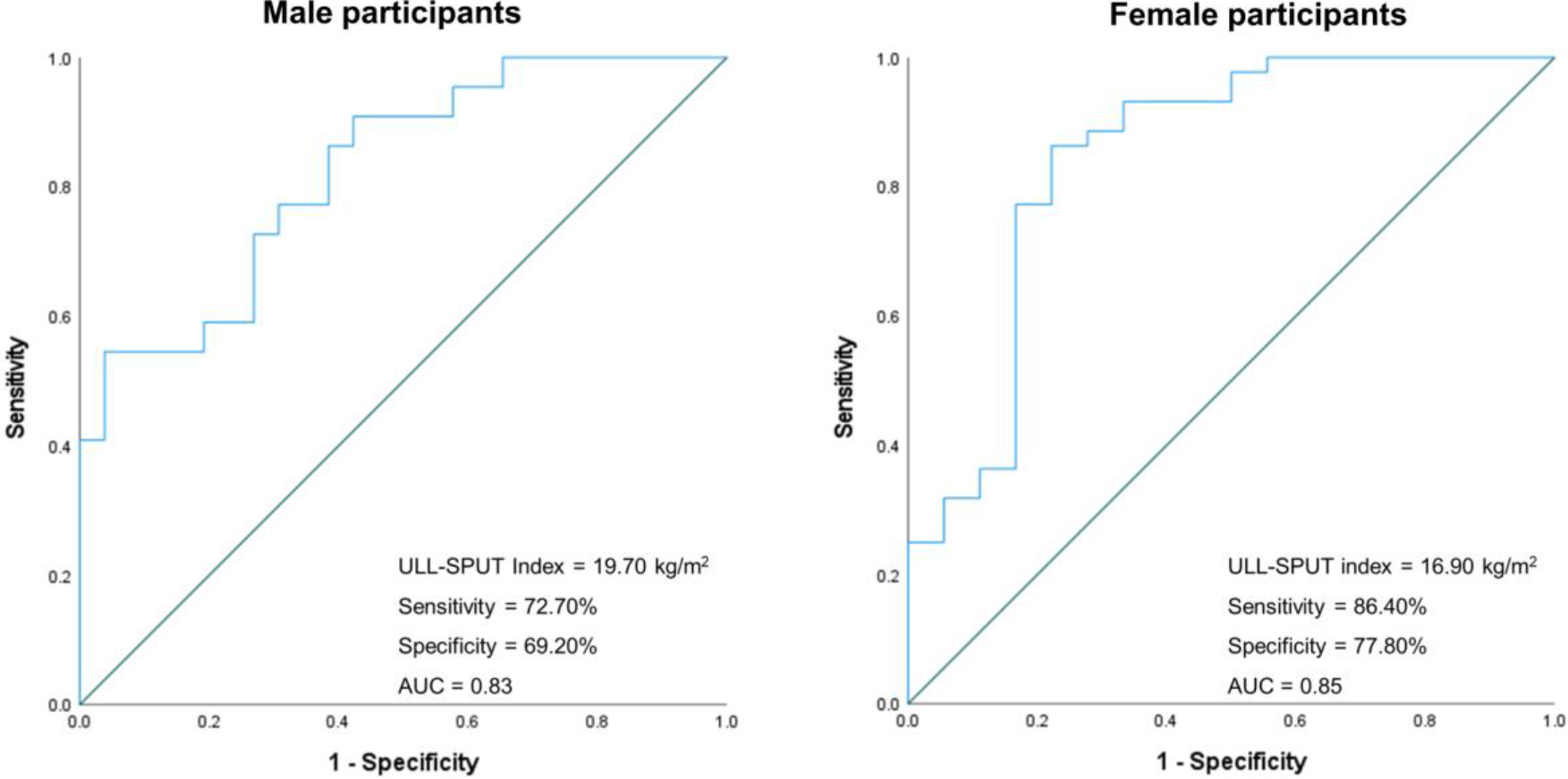
The ROC analysis indicated that the ULL-SPUT index of
Discussion
In light of the current healthcare paradigm shift toward providing standardized community and home healthcare services, this study investigated the ability of a practical measure, namely the ULL-SPUT index, to identify older adults living with sarcopenia. The findings indicated that nearly half of the participants (40%) had sarcopenia, according to the data from standard criteria. These participants were significantly older, with LBM, BMC, and body fat mass lower than those without sarcopenia (
The findings reflect natural characteristics of individuals with sarcopenia, a condition of age-related SMM loss affecting ASM, muscle strength, and/or physical performance [29, 30, 31]. These characteristics were particularly evidenced in female participants, all of whom had low muscle strength, ASM index, and body composition along with slow walking speed (Table 2). Lean body mass is important for protection against frailty, physical dysfunction, and adverse health conditions [31, 32, 33]. Appendicular skeletal muscle is needed for protein synthesis of the body’s organs and force generation for mobility and independence [31, 33, 34]. Low BMC is associated with the presence of osteopenia, osteoporosis, deformity, and fractures. These findings were important particularly when the participants were well-functioning but the findings suggest the internal deterioration that could further affect their health and independence. These people are also accounted as having a high risk of fall and subsequent injury, and up to 75% of older adults who sustained a hip fracture after falling did not regain their prior level of function [14, 23, 32]. Furthermore, older adults who are admitted to a hospital because of a fall are likely to experience subsequent disability and nursing home placement [35, 36]. Cesari et al. [37] also reported that older adults with a usual walking speed slower than 1 m/s were those with a high risk of poor health-related outcomes. Therefore, these findings confirm the need for a strategy to identify those with sarcopenia early to prevent or minimize the adverse health consequences and disability associated with this condition.
The present findings suggest that the ULL-SPUT index of
With the involvement of bodyweight while lifting the body upward, the ULL-SPUT data in this study were additionally adjusted for each participant’s height, similar to that of the ASM index as proposed by previous reports [3, 27], so the data would be comparable among the participants. The findings are in agreement with previous reports that found the association between the ability to perform the ULL-SPUT and muscle strength, body composition, and mobility of older people with and without sarcopenia [10, 12, 13, 42].
Handgrip strength is a well-investigated measure to assess the small muscles of the upper limb that are susceptible to decline with age. Global physiological changes enable its outcomes to reflect overall muscle strength and detect abnormalities in older adults [43]. However, execution of the HG strength test in an open-kinetic chain manner (i.e., squeezing the tested hand maximally without the involvement of the bodyweight) could reduce its challenge, therefore reducing the ability of the outcomes to reflect body composition when the rate of age-related reduction in muscle strength is three times greater than the rate of SMM decline [44, 45, 46]. Therefore, the HG strength test must be used in combination with the other body composition and physical performance measures to detect sarcopenia [3].
With the need of a practical standard strategy to distribute effective community- and home-healthcare services, the present findings suggest the use of the ULL-SPUT index as an alternative practical measure, perhaps accomplished using digital bathroom scales, to identify sarcopenia in community-dwelling older adults. Then standard measures can be further implemented to confirm the abnormality and early interventions initiated to promote treatment effectiveness.
Nonetheless, this study has some limitations needed to be concerned for clinical implication. Older adults with sarcopenia commonly have low BMI; thus, this study recruited participants with a BMI
Conclusions
With the need for practical measures to promote standard community and home healthcare services, the present findings suggest the use of the ULL-SPUT index of
Author contributions
All authors were responsible for the research conceptualization, study design, and final approval of the manuscript. PC, PP and RI were involved in data collection. PC was engaged in statistical analysis, data interpretation, and drafting the manuscript. SA and TT were responsible for funding application. SA worked on research management, data interpretation, and finalized the manuscript. All authors read and approved the final manuscript.
Data availability statement
All relevant data are included within this manuscript and raw data are archived by the corresponding author.
Compliance with ethical standards
All procedures of the study were in accordance with the standards of the Ethics Committee for Human Research (HE 622255). Eligible participants completed a written informed consent form before participation in this study.
Footnotes
Acknowledgments
This research was supported by the Fundamental Fund (2024) and Research and Graduate Studies, Khon Kaen University (RP64016), Khon Kaen University, Thailand.
Conflict of interest
The authors declare no potential conflicts of interest.