
Abstract
BACKGROUND:
With lifestyle changes, the prevalence of flatfoot is increasing year by year, with a prevalence of 29%. Flatfoot will lead to an inevitable injury and reduce the quality of life. Short foot exercises can enhance the strength of the intrinsic muscles of the foot and improve the symptoms of flatfoot. However, there is controversy regarding its specific efficacy.
OBJECTIVE:
This meta-analysis quantitatively evaluates the effect of short foot training on patients with flatfeet and provides evidence to inform the clinical approach to short foot training in patients with flat feet.
METHODS:
A total of eight databases were searched, including CNKI, WANFANG, VIP, and CBM in Chinese and PubMed, Cochrane, Web of Science, and Embase in English. The timeframe for searching the literature was March 2023 for each database build. English database search terms and search formulas were: (flat foot OR talipes valgus OR talipes calcaneovalgus) AND (short foot exercises OR physical therapy OR neurophysiotherapy).
RESULTS:
The current pooled results show no significant difference in the improvement of the navicular drop test and foot posture index with short foot exercises compared to controls; only short foot exercises greater than 6 w showed a significant improvement in the navicular drop test, and sensitivity analysis showed a significant improvement in the foot posture index with short foot exercises.
CONCLUSION:
This systematic review and meta-analysis showed that short foot exercises need a larger sample size to find their effect on improving flat feet; the duration of the intervention is a factor. As most studies are currently unclear whether the participants were patients with flat feet or asymptomatic individuals with flat feet the disease syndrome in patients with flatfoot may also be a factor.
Introduction
Flatfoot is a common foot condition with a prevalence of 11.2–29.0% in adults [1], and is characterized by partial or complete collapse of the medial longitudinal arch (MLA), hindfoot valgus, and weight-bearing forefoot abduction [2, 3]. Common diagnostic criteria for flat feet include Navicular drop (ND)
The most widely used conservative treatments for flatfoot are orthotic therapy [14] and exercise therapy [15], but a 2018 meta-analysis showed that orthotic therapy has a limited impact on patients with flatfoot, providing only temporary relief rather than a fundamental change in the muscular dysfunction present in flatfoot [16]. Exercise therapy strengthens the muscles of the foot to provide dynamic support, and it also has the advantage of supporting and stabilizing the MLA [17], so there is a consensus in favor of strengthening the foot function of patients with flat feet through exercise therapy. The human foot is maintained by bones, muscles, ligaments, and joints [18], and if there is a problem in any of these areas, the muscles inside and outside the foot compensate to improve foot balance, which may lead to arch collapse and flat feet [19]. It has been shown that in patients with flat feet, the internal muscles of the foot can support the MLA [20] (in particular, the abductor magnus, which can be contracted to change the angle of the MLA accordingly [21]) and can alter the kinematics of the foot during walking and that strengthening these muscles can prevent or treat overuse injuries to the lower limb due to flat feet [22].
Short-foot exercise (SFE),an exercise method that actively contracts the intrinsic muscles of the foot so that the metatarsal heads are directed toward the calcaneus without flexing the toes or contracting the extrinsic muscles of the foot [23, 24], strengthens the intrinsic muscles of the foot [17, 25] and has been used to intervene in flat feet. Studies have shown that SFE can reduce FPI in patients with flat feet [26], increase ankle stability, and effectively strengthen the MLA of the foot [17, 27]. In a recent study, Sahan et al. showed that short-term short-foot training combined with virtual reality was effective for both balance and navicular drop in patients with flat feet [28]. Most of the current studies have shown SFE to be effective in improving FPI and MLA (elevation of the medial longitudinal arch) in patients with flat feet, but most are small sample studies, and it is unclear whether changes in intervention factors affect outcomes. SFE as a method for training plantar intrinsic foot muscles also has some controversy. Recently, Willemse et al. found plantar intrinsic foot muscles (such as short foot exercise) had very low-certainty evidence to improve foot function and dynamic balance [29]. However, Wei et al. found that intrinsic foot muscle training can improve dynamic postural balance [30]; Hoang et al. [27] and Huang et al. [9] pointed out the importance of foot exercise for flat feet. The above results may be due to differences in frequency and include people. Hara et al. found that SFE can improve MLA for flatfeet when exercise frequency exceeds 5 weeks, but they did not perform a meta-analysis of three studies, which may influence the results [27]. Therefore, we conducted this study to examine the effect of short foot exercises on patients with flat feet and the desired frequency of treatment, which will provide reference evidence for the clinical treatment of flat feet.
Materials and methods
Search strategy
A total of eight databases were searched, including CNKI, WANFANG, VIP, and CBM in Chinese and PubMed, Cochrane, Web of Science, and Embase in English. The timeframe for searching the literature was March 2023 for each database build. English database search terms and search formulas: (flat foot OR talipes valgus OR talipes calcaneovalgus) AND (short foot exercises OR physical therapy OR neurophysiotherapy). The study was registered in INPLASY under number INPLASY2023120095.
Search terms
Search strategy for PubMed
Search strategy for PubMed
“Flatfoot OR Splayfoot OR Flatfeet OR Flat Foot OR Pes Planus OR Talipes Valgus OR Vertical Talus OR Rigid Flatfoot OR Rocker-Bottom Foot OR Pes Valgus, Congenital Convex OR Congenital Vertical Talus OR Talus, Congenital Vertical OR Convex Pes Valgus OR Convex Foot OR Talipes Calcaneovalgus OR Acquired Adult Flatfoot Deformity OR Flexible Flatfoot” and “short foot exercises”. The PubMed search strategy is listed in Table 1.
Inclusion criteria (PICOS):
People (P): Patients with flat feet (ND Intervention (I): SFE, or SFE combines other treatments. Control (C): Other forms of intervention or without intervention. Outcome (O): The primary outcome was the ND, and the secondary outcomes were the FPI. Study (S): The type of study must be a randomized controlled clinical trial.
Exclusion criteria:
People with other foot problems (such as ankle instability) OR systemic conditions i.e. neuropathy, diabetes, rheumatological conditions. Incomplete data or article content. Significant risk of bias (Methodological flaws in the design, behavior, or analysis). Systematic overviews, secondary analyses, and conference abstracts. Repeat literature.
Data extraction and outcome measures
Firstly, we imported the collected literature into Endnote’s literature management system. Secondly, after reading the titles and abstracts, a rigorous screening process was carried out based on inclusion and exclusion criteria. After the initial screening, potentially relevant original texts were downloaded for reading. After reading the full text, literature that met the criteria was included. Data extraction from the included literature was carried out by two independent researchers and summarized in Excel. Data extracted: first author, country, patient, sample size, mean age, intervention type, frequency, training outcomes, and outcome indicators. The primary outcome indicator was the navicular drop test (NDT), and the secondary outcome indicator was FPI.
Flowchart of the study search and selection process.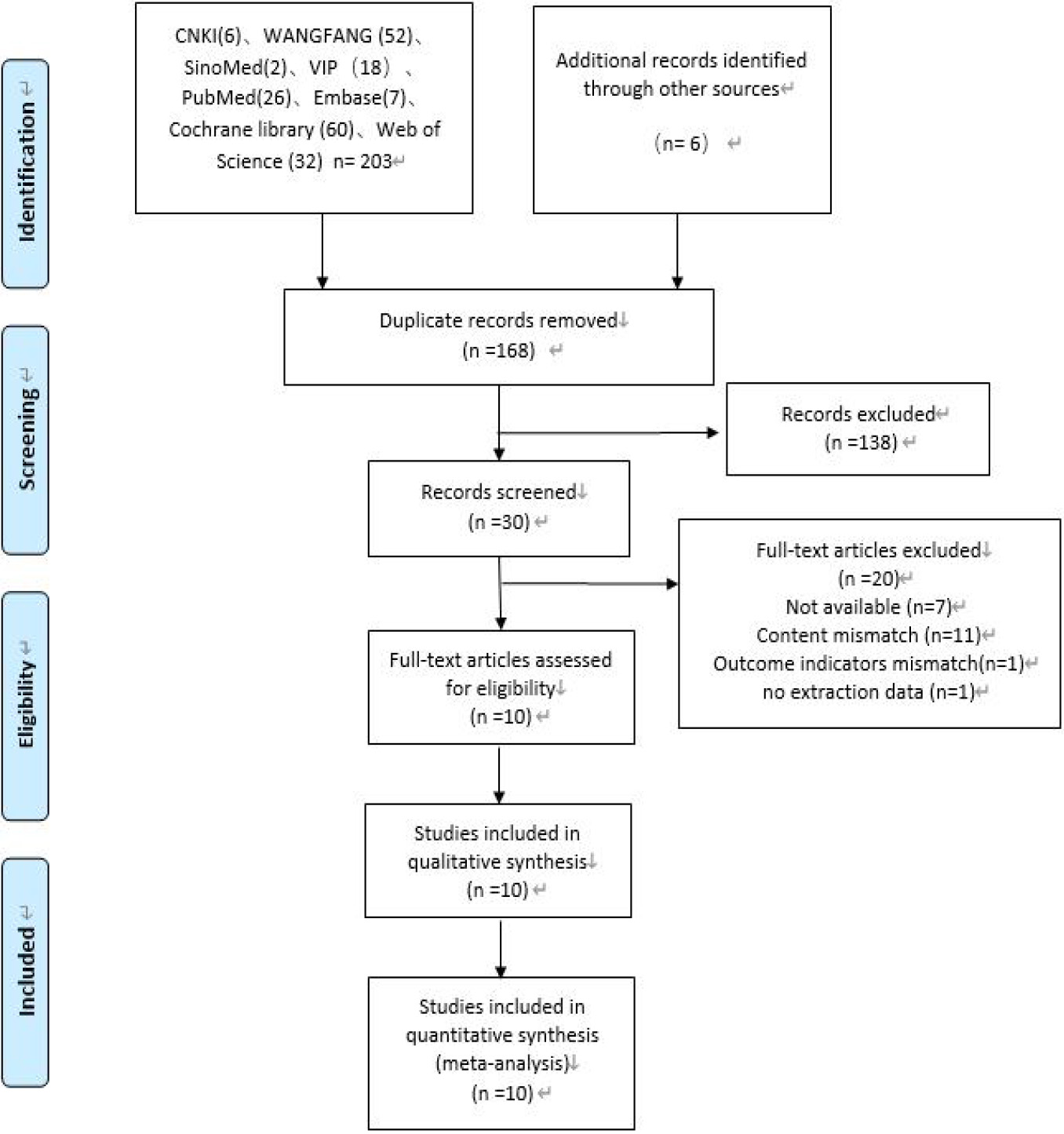
The risk of bias for each study was assessed by two investigators using the Cochrane Handbook for Systematic Reviews of Interventions, with two other investigators consulted to resolve any disputes in seven areas, including random allocation protocol, allocation protocol concealment, investigator and subject blinding, outcome assessment blinding, completeness of outcome data, selective reporting bias, and other sources of bias. Each potential bias was categorized as high-risk, unclear, or low-risk. All results were recorded through RevMan 5.4.
Statistical analysis
The meta-analysis was performed via Review Manager (RevMan) version 5.4 software. The data were continuous variables, so we used mean differences (MD) and 95% confidence intervals (CI) for the analysis. If heterogeneity was found to exceed 50%, a random effects model was used in the meta-analysis. Corresponding subgroup or sensitivity analyses were performed to explore sources of heterogeneity. In addition, funnel plots were used to assess the publication bias of the studies.
In this systematic review and meta-analysis, most of the RCTs that included reported data on parameters of the left and right foot, and considering the avoidance of population bias (left or right flatfoot), data on both the left and right foot were included for the meta-analysis.
Results
Search results
Eight databases were searched for this review, and Fig. 1 shows the selection and search process. 209 papers were searched, leaving 168 after removing the duplicate paper and leaving 30 to be read in full after reading the titles and abstracts. After downloading and reading the full text, 20 papers were excluded, thus in total including 10 papers.
Characteristics of included studies
Basic characteristics of the included literature
Basic characteristics of the included literature
Abbreviations: ND: Navicular drop; NDT: Navicular drop test; BMI: Body Mass Index; F: Female; M: Male; FPI: Foot Posture Index; CSA: cross-sectional area; MLA: medial longitudinal arch; AbdH: abductor hallucis; FH: flexor hallucis; RCSP: resting calcaneal stance position; CAIT: Cumberland ankle instability tool; PFP: Patellofemoral pain.
Basic characteristics of the included literature (how the strengthening interventions are used)
Abbreviations: SFE: short-foot exercise, F: Female, M: Male, FO: foot orthosis, FOSF: foot orthosis and short-foot exercise, ASI: arch support insoles, TCE: towel curl exercise, NBFE: non-biomechanical function exercise, VRE: Virtual reality exercises, SMT: sensorimotor training, PNF: proprioceptive neuromuscular facilitation, y: year, w: week; min: minutes; d: days; t: times.
The 10 studies were published between 2011 and 2021 and included 10 articles from 4 countries, five from Korea, 3 from Turkey, 1 from Spain, and 1 from Japan, and their basic characteristics are shown in Table 2. A total of 344 patients, aged 19–44 years, were included in this meta-analysis. As can be seen in Table 2, only 2 of all studies were studied in symptomatic flat foot, such as CAI and PFP. The other group identified a critical value for flat, flexible or flat foot based on patient characteristics. Other studies have not been reported in detail. Two publications did not describe gender, while 129 male subjects and 155 female subjects were included in the other eight publications. Eight studies performed SFE specifically in the intervention group, one combined sensorimotor training, and one combined foot orthosis. The control group in all studies received different interventions, except for three studies that did not have any interventions. The basic characteristics of the included literature are shown in Tables 2 and 3.
Risk of bias summary: review authors’ judgments about each risk of bias item for each included study.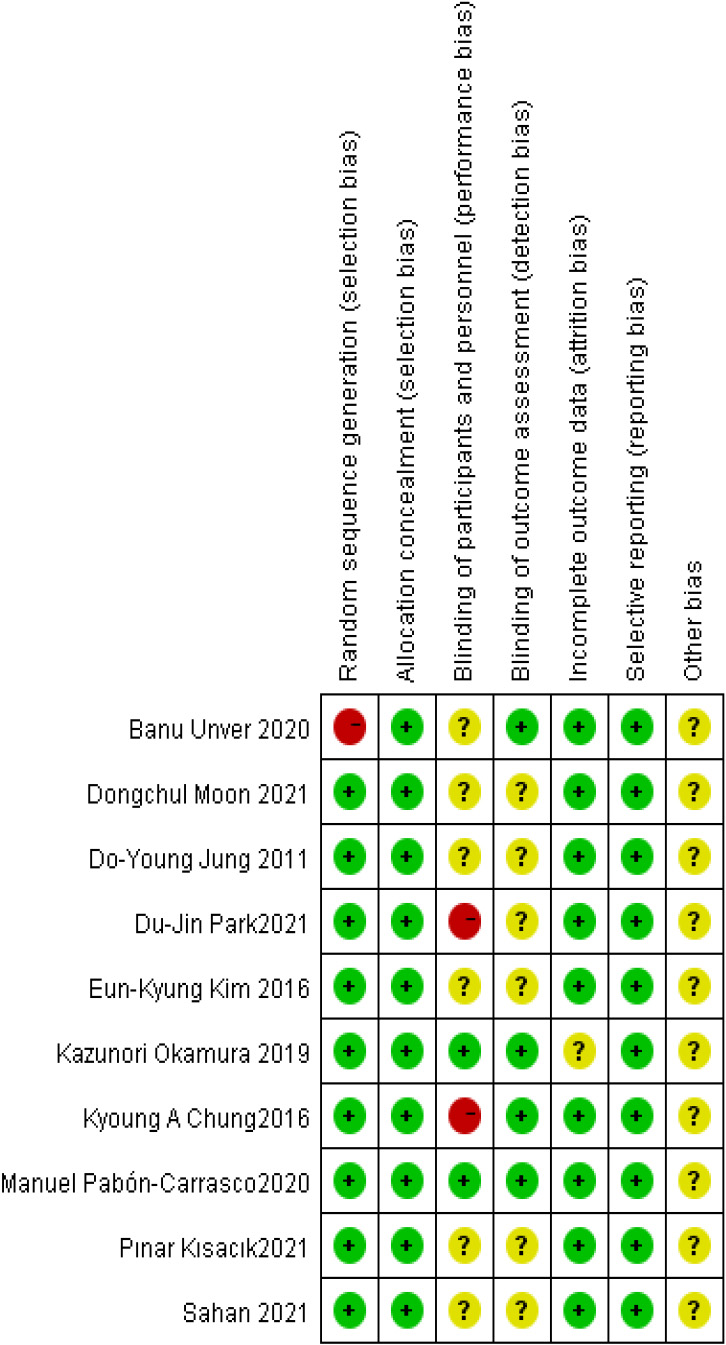
Risk of bias graph: review authors’ judgments about each risk of bias item presented as percentages across all included studies.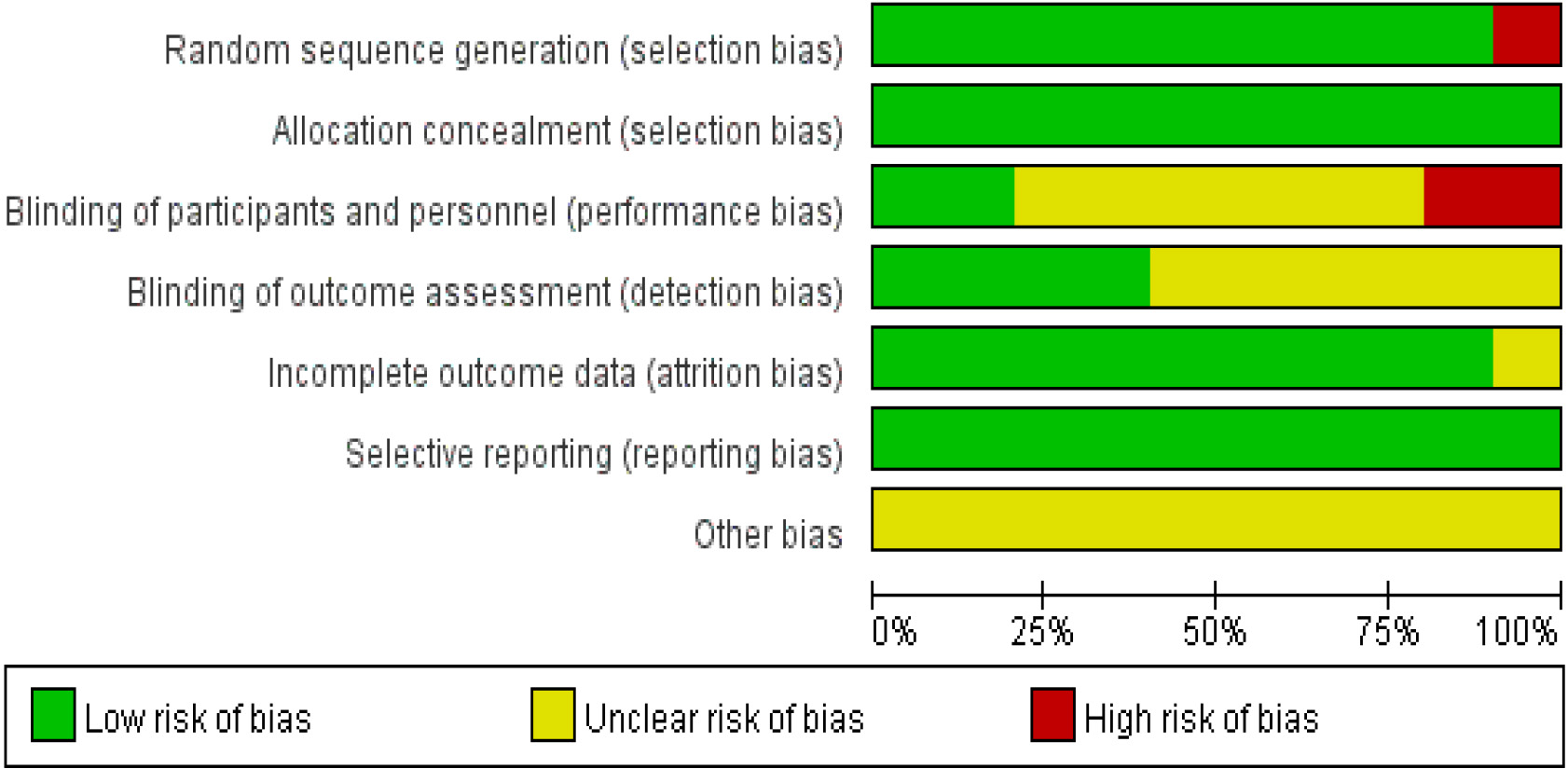
The publication bias of all studies was determined by funnel plot.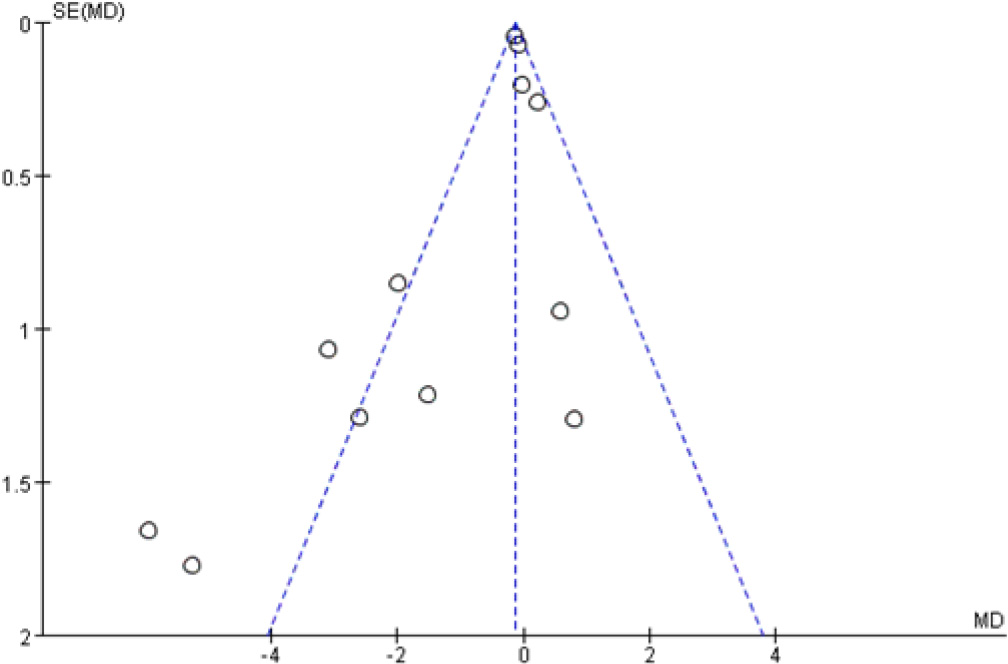
We assessed the risk of bias in the included literature according to the Cochrane Handbook for Systematic Reviews of Interventions, and the results are shown in Figs 2 and 3. Seven RCTs described in detail the method of random sequence generation; one grouped patients according to patients’ preferences. Ten studies reported that allocation concealment was used; only two studies indicated that double-blinding was used; and in four studies, the grouping was unclear to the assessor. Strict blinding of participants was difficult due to the characteristics of the SFE. All studies reported outcomes, and few other significant biases were found. From the funnel plot (Fig. 4), we can see that the spot is separate and does not have a symmetric distribution. They included studies with publication bias that may be related to different sample sizes. It is unclear whether most participants are patients with flat feet or asymptomatic individuals with flat feet. This could be one of the potential causes of bias.
Effect of SFE on navicular drop
Meta-analysis forest plot of the effect of short-foot training on reducing navicular drop.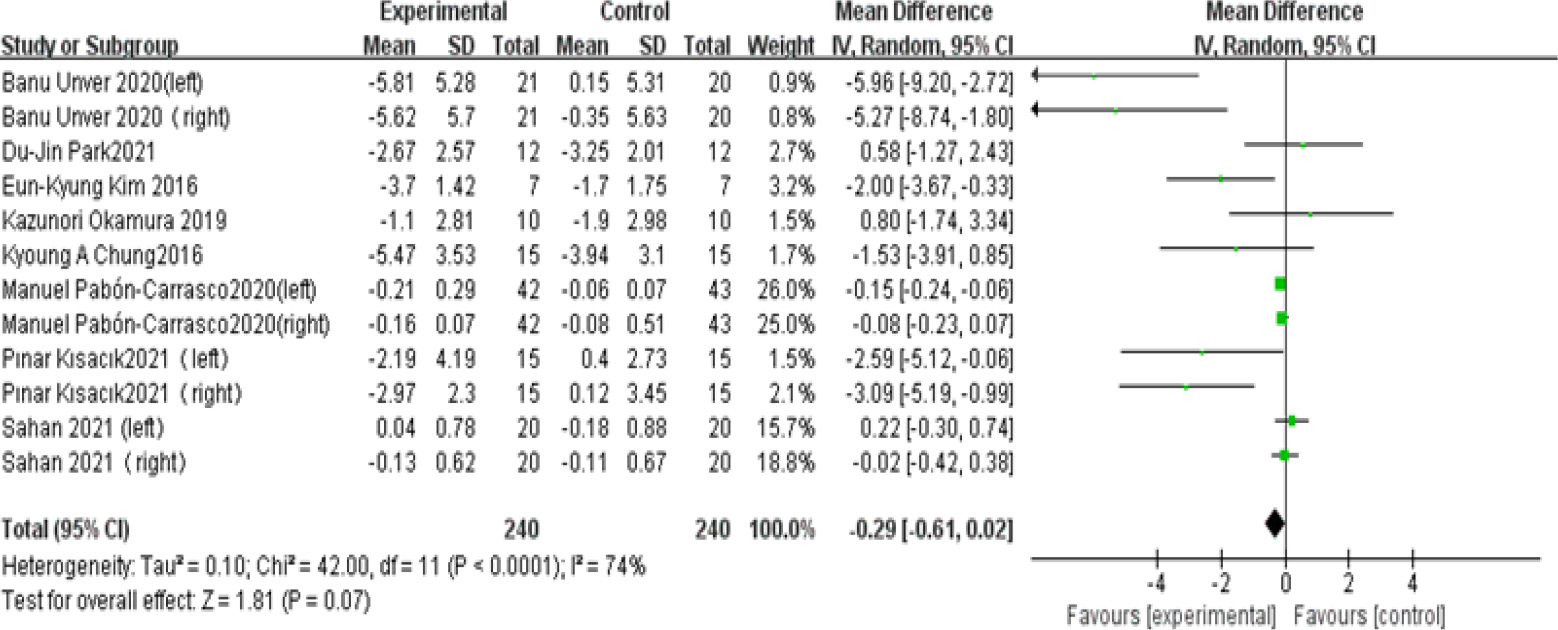
The height of the navicular drop was assessed by the NDT in 8 studies. 4 studies assessed both feet of each participant, and the other 4 studies tested only one foot. Change scores were extracted from the 8 studies, and no effect of SFE was found to reduce navicular drop height compared to controls (MD
Subgroups of different intervention times analyzed forest plots.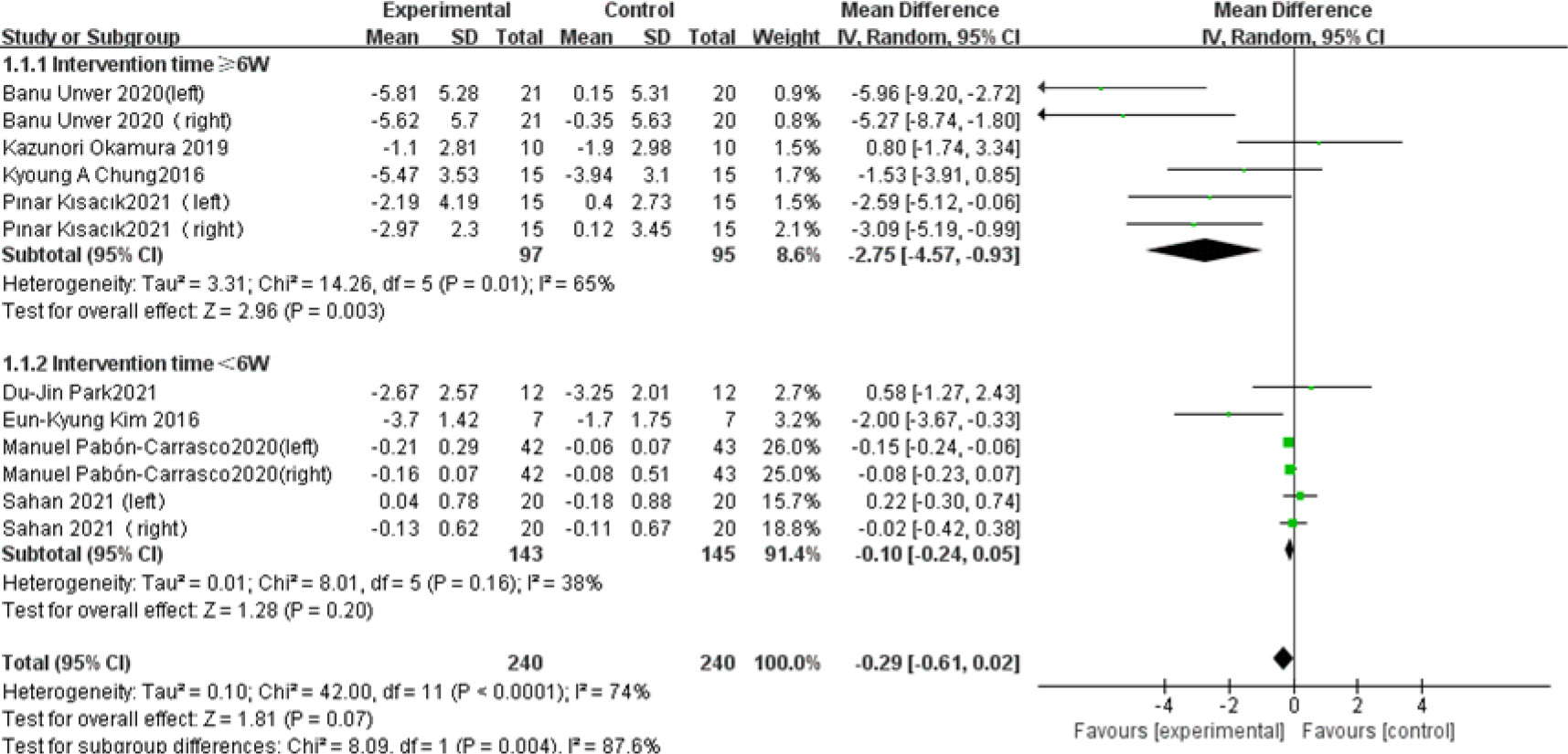
A subgroup analysis of these eight studies is shown in Fig. 6. Heterogeneity was smaller in the intervention group with
Meta-analysis forest plot of the effect of short-foot training on foot posture index.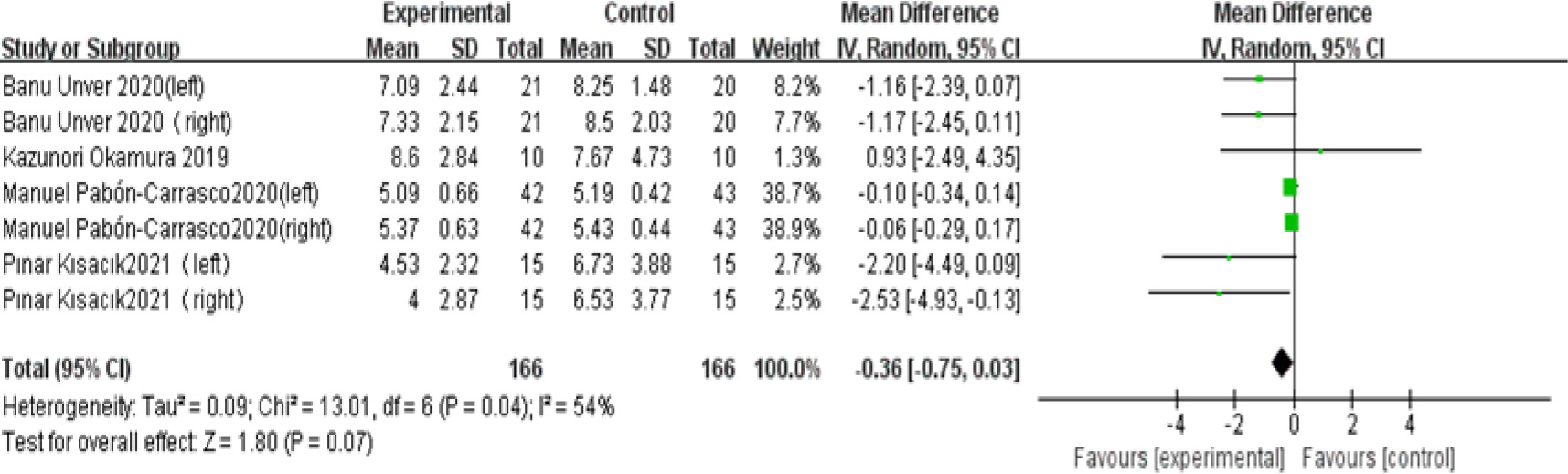
Meta-analysis forest plot of the effect of short-foot training on Foot Posture Index after deleting one study.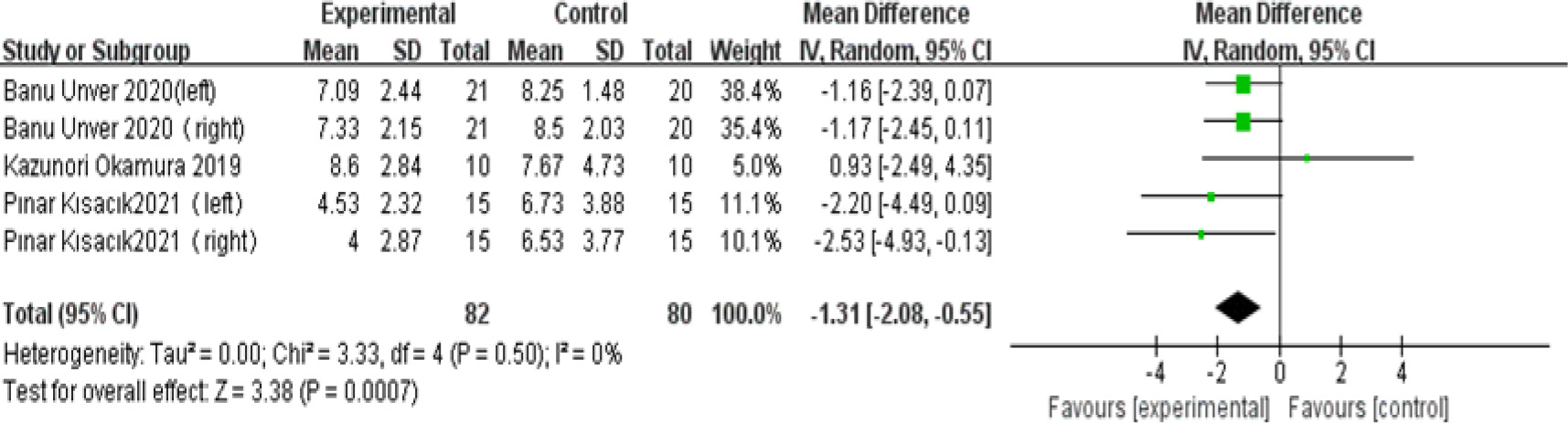
Four studies assessed the patient’s foot posture by the FPI, three studies assessed both feet of each participant, while the other study tested only one foot. Meta-analysis results showed no significant reduction in the FPI in the experimental group compared to the control group (MD
This study aimed to confirm the effect of SFE on NDT/FPI in patients with flatfoot. The results of the current study suggest that the duration of the SFE intervention was greater than 6 weeks before it showed an improvement in NDT in patients with flat feet. SFE also improved the flat FPI and thus improved the range of discomfort symptoms in patients with flat feet. We also found that study heterogeneity led to negative results, that the duration of SFE affected the efficacy of NDT, and that the quality of the study would be directly related to the efficacy results, which has important implications for the clinical application of SFE. It is suggested that future studies need to standardize study quality, minimize study bias, and have sufficient SFE training time for patients with flat feet.
SFE was initially often used as a training exercise to strengthen the intrinsic muscles of the foot and enhance the longitudinal and lateral arches. Jung et al. found that short foot exercises were effective in activating the abdominal muscles and preventing a decrease in MLA [21], but the mechanism of improvement in the MLA is unclear and may be related to the fact that SFE strengthens the medial muscles of the foot. Treatment of flat feet is divided into conservative and surgical treatments. Flat feet without painful symptoms in the foot can be treated conservatively. There are two types of conservative treatment: one is the use of supportive insoles, and the other is the performance of foot muscle exercises, which commonly include sitting on tiptoe, toe gripping towels, and foot rollers. SFE has recently become popular in patients with flat feet [24], and there is evidence that SFE enhances dynamic balance control and somatosensory function compared to other common exercises [39] and better activates the intrinsic muscles of the foot.
The effect of short foot training on ND in patients with flat feet
The most typical symptom of flatfoot is a reduction or collapse of the MLA, and the ND test is a valid and reliable method of assessing the MLA [40], as measured by measuring the difference in height of the navicular bone between the subject in sitting and standing positions (with the subtalar joint in neutral position). Subjects were defined as having flat feet when their ND exceeded 10 mm [41], so the effectiveness of the intervention could be evaluated by the change in ND score, with a decrease in ND score indicating effectiveness. Okamura et al. showed that after 8 w of SFE, the time to reach a minimum navicular height in patients with flat feet was reduced, indicating that the windlass mechanism (protection of the MLA) of the foot was enhanced [26]. Unver et al. found a significant reduction in ND scores and a significant increase in maximum plantar pressure in the midfoot after 6 w of SFE [31], suggesting that SFE is an effective solution for improving medial arch collapse. In a recent study, Amira. et al. concluded after 4 months of SFE that exercise of the internal muscles of the foot was significant in improving the internal rotation of the foot and strengthening the foot structure [42]. The results of the analysis of 8 of the 10 included in this study showed that SFE improved ND in patients with flat feet. Kısacık et al. found that SFE can increase the score of NDT [38], but the patients are injured (patellofemoral pain), which may influence the result. Our meta-analysis synthesized the results of the eight available studies and showed that SFE training duration greater than 6 months showed sufficient efficacy for ND, and SFE was ineffective for training duration less than 6 months.
The effect of short foot training on FPI in patients with flat feet
The FPI is a common method of assessing foot posture during static weight bearing [43] and is reliable in clinical use [44]. The FPI consists of six items, including palpation of the talar head, superior and inferior lateral flexion of the outer ankle, heel valgus, protrusion of the talonavicular region, height and consistency of the MLA, and abduction and adduction of the forefoot about the hindfoot, each of which is scored between
The outcome indicators in the literature included in the meta-analysis were mainly NDT and FPI, but some of the literature also evaluated the function of SFE from other perspectives. In an experiment conducted by Namsawang et al. in 2019, it was noted that the cross-sectional area of the thumb abductor muscle increased after 4 w of SFE and that the activity of the muscle was higher after training [46]. The effect of SFE also did not diminish over longer training cycles. Jung et al. showed a significant increase in the cross-sectional area of the abductor hallucis muscle in patients with flat feet after 2 months of SFE [33], although this could of course be related to the different severity of flat feet in the subjects in each experiment. In addition to the internal muscles of the foot, the lateral muscles of the foot have also been investigated in patients with flat feet. Park et al. found that the peroneus longus muscle was less active in patients with flat feet than in normal feet and could not be activated for a short period [47]. Kim et al. tested dynamic balance by YBT in a study and showed that balance was significantly improved in the SFE and ASI groups (orthotic insoles) after the intervention, and the improvement was more pronounced in the SFE group, possibly due to SFE improving ankle stability. Sang Kim et al. [48] found that SFE under conditions where visual feedback was received enhanced balance and accuracy in patients with flat feet when performing knee. In a recent study, Sahan et al. showed that short-term SFE and VR were effective for both balance and navicular drop in patients with flat feet [28]. Therefore, SFE can be combined with other interventions to improve the symptoms of flatfoot.
limitation and outlook
This study provides a more comprehensive analysis of the effects of SFE in patients with flat feet; however, the number of current studies remains inadequate, many with different outcome indicators and different intervention durations, which limits the persuasiveness of the evidence, and existing studies have not been conducted in larger populations and are mostly limited to younger populations. It is not clear in existing studies that most of the participants are flat feet or asymptomatic individuals with flat feet. This may lead to bias, the universality of the findings may be weakened, and our conclusions need to be treated with caution. Larger samples and multicenter, high-quality randomized controlled trials are needed in the future. Further optimization of intervention intensity and duration for different age groups of flat feet is needed to facilitate analysis of the age groups to which arch plasticity or recoverability applies.
Conclusion
Unlike existing clinical randomized controlled studies, the current meta-analysis of evidence does not yet prove that SFE is fully effective in improving NDT and FPI in patients with flat feet. Since it is not clear from the current study whether the majority of participants were patients with flat feet or asymptomatic individuals with flat feet, we must clarify that disease syndromes in patients with flat feet may be a contributing factor. More studies are needed to continue to explore this in depth. However, the results of our subgroup analysis showed that only SFE with an intervention duration of more than 6 w seemed to be effective in improving ND in patients with flat feet. Intervention duration is a factor that influences the effectiveness of interventions and needs to be focused on in future studies.
Author contributions
DH and JC contributed to the conception and design of the study, searched and screened the articles, and performed the data analysis. ZL and YH resolved, after consultation, some controversial issues. YH provided the funds. ZL and JC helped check the grammar and resolved data problems. JC and JQ were responsible for the quality assessment of the content. DH and ZL wrote the final revision of the article. All authors approved the final version of the manuscript.
Data availability statement
Details of the raw data are available in PubMed. The datasets used and analyzed in the current study are available from the corresponding authors upon reasonable request.
Ethical approval
Not applicable.
Funding
This study was funded by the Rehabilitation College of Gannan Medical University.
Informed consent
Not applicable.
Footnotes
Acknowledgments
The authors would like to thank the teachers of Gannan Medical University for their help and all authors for their hard work.
Conflict of interest
The authors declare no conflict of interest regarding the authorship and publication of this article.