
Abstract
BACKGROUND:
Proprioceptive neuromuscular facilitation (PNF) stretching exercises have been widely advocated for the management of patients with different musculoskeletal conditions. However, its effect on the treatment of temporomandibular dysfunction (TMD) in patients with forward head posture (FHP) has not been fully investigated.
OBJECTIVE:
To investigate the effect of PNF stretching exercises on the treatment of TMD in patients with FHP.
METHODS:
A prospective, randomized, double-blinded clinical trial. Twenty-four patients with TMD and FHP aged from 18–40 years were randomly assigned to PNF or control group. The PNF group composed of 12 patients received PNF stretching exercises of masticatory muscles in addition to routine physical therapy treatment (FHP correction exercises and ultrasound for the temporomandibular joint); the control group composed of 12 patients received routine physical therapy treatment only. Interventions were conducted twice a week for six weeks. Craniovertebral angle, pain threshold, pain intensity, temporomandibular joint ROM, and temporomandibular joint function were assessed for all participants before and after the intervention. The outcomes were analyzed using Two-way mixed MANOVA. For further multiple comparisons, post-hoc tests with the Bonferroni correction were performed.
RESULTS:
There was no significant difference between both groups pre-treatment (
CONCLUSION:
Adding PNF stretching exercises of masticatory muscles to routine physical therapy programs is an effective method for management of TMD in patients with FHP more than routine physical therapy programs alone.
Introduction
Temporomandibular joint disorders are an umbrella term for pain and dysfunction of the temporomandibular joint (TMJ) [1]. Alteration in the function of TMJ leads to poor quality of life for the individual as this joint is involved in basic activities like talking, eating, and laughing. The symptoms of TMJ disorders include headache, limited mouth opening, muscle spasm, tinnitus, fullness in ears, cervical spine dysfunction, and altered craniovertebral angle seen as forward head posture (FHP) [2, 3].
The TMJ within its muscular and ligamentous connection to the cervical spine forms a functional complex known as the ‘cranio cervical’ mandibular system [4]. It has been observed that there is a synergistic relationship between the cervical spine and masticatory muscles with jaw and neck muscles during normal activities involving chewing, talking, and yawning [5]. Therefore, head and neck position affects TMJ kinematics and any changes in head position change the position of the mandible [6, 7, 8].
The integrated approach of dental practitioners, physical therapists, and psychologists is often required for the successful management of people with long-standing temporomandibular dysfunctions (TMDs) [9]. According to the American Academy of Craniomandibular Disorders and the Minnesota Dental Association, physical therapy modalities (electrophysical modalities, therapeutic exercises, and manual therapy techniques), are an important treatment for musculoskeletal pain relief and inflammation reduction and restoration of oral motor function [10].
Proprioceptive neuromuscular facilitation (PNF) involves manual resistance using isometric muscular contraction followed by relaxation and stretching of the tight muscle; is used for the treatment of myofascial trigger points and as well as for the relief of any pain originating in these muscles [11]. PNF achieves these objectives by making use of two physiological phenomena: post-contraction inhibition and reciprocal inhibition [12]. It has been reported by Travell and Simon [13] that PNF techniques directed to each specific jaw muscle, namely the masseter, temporalis, medial pterygoid, and lateral pterygoid muscle can release trigger point tension in the tight jaw muscles.
It was pointed out by numerous researchers that pain in the upper quarter and masticatory motor system may be caused by cervical spine disorders and vice versa [14, 15]. In FHP, flexion occurs in the lower cervical spine C3-C7 with hyperextension of upper cervical spine C1 and C2, which generates tension in the infrahyoid muscles, lower and posterior traction on the hyoid, and traction transfer to the mandible, leading to retraction and opening of mouth [16]. In addition, FHP seemed to be associated with a decreased pain threshold and the development of active trigger points in the cervical and masticatory muscles [17, 18].
Although the literature has revealed a number of studies on PNF and its efficiency in the treatment of myofascial pain and associated dysfunction [19, 20, 21, 22, 23], to date no studies have shown the effectiveness of PNF for the treatment of TMJ dysfunction in patients with FHP. Hence, this is the first double-blinded randomized controlled trial to investigate the effect of PNF stretching exercises on the treatment of TMD in patients with FHP.
Materials and methods
The present study is a prospective, randomized, parallel-group, double-blinded clinical trial. The study was carried out from August 2022 to January 2023, and was approved by the Research Ethics Committee at the Faculty of physical therapy, Cairo University (P.T.REC/012/004165). All volunteers were provided with written informed consent to participate in the study after being fully informed of the study’s goals and procedures. The participants were recruited from the Outpatient Clinic at the Faculty of Physical Therapy, Misr University for Science and Technology. Every procedure was carried out in conformity with the Helsinki Declaration of 1964 and any subsequent changes. The study was registered in the ClinicalTrials.gov registry, registration number: NCT05709340.
Flowchart of study participants.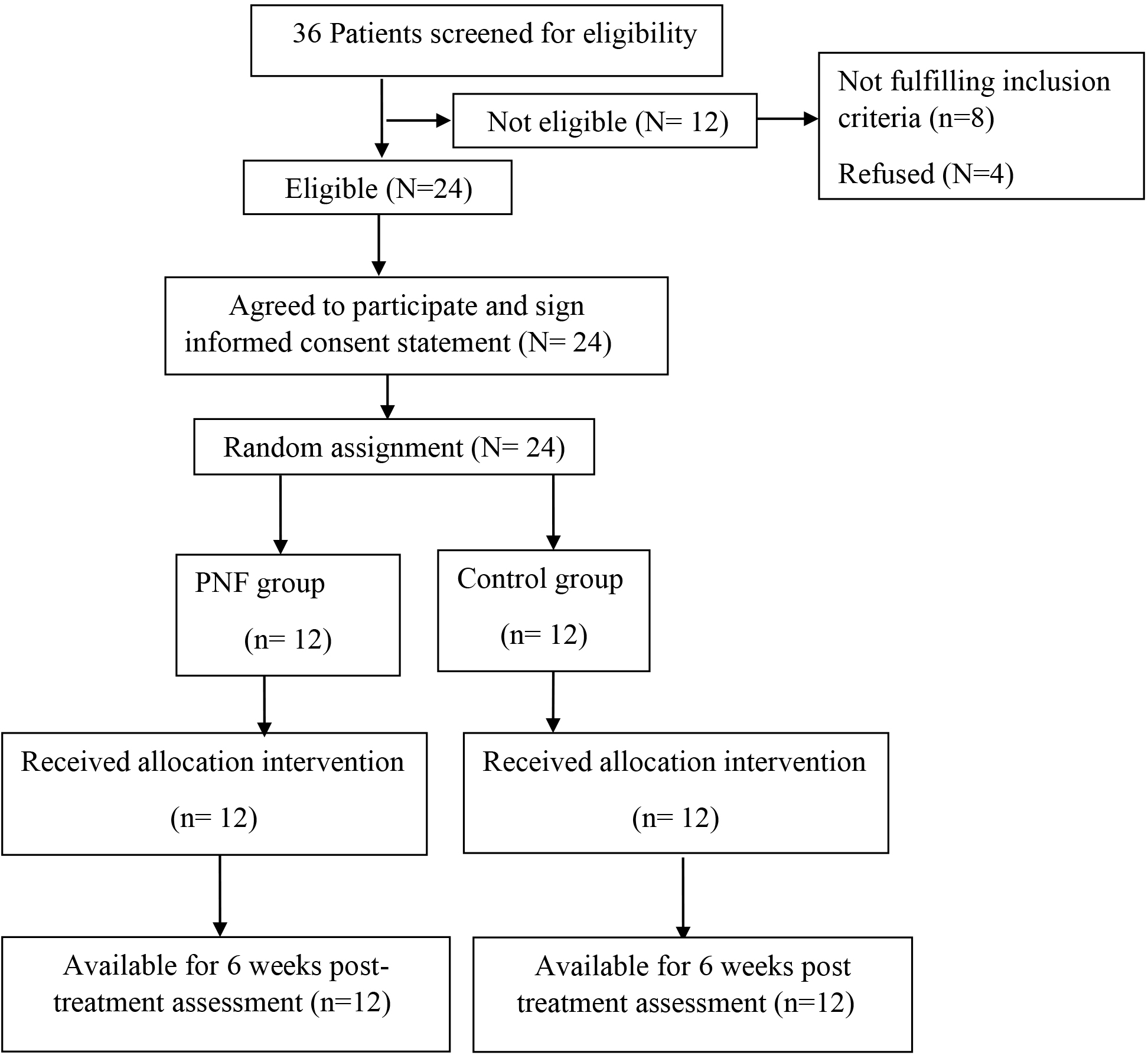
Twenty-four patients of both genders were enrolled in the current study in accordance with the following eligibility criteria: (1) The patient’s ages ranged from 18 to 40 years [24]; (2) having TMD symptoms sustained for at least twelve weeks duration established by expert physician or orthopaedician; (3) having FHP with CVA
Randomization
Using the online randomization application “Research Randomizer” (
Intervention
The same routine physical therapy program was given to each patient in both groups. This includes ultrasound therapy followed by Kendall exercises. Ultrasound therapy was applied over TMJ and masseter area with Mode 1:1, frequency of 1MHz, intensity of 1.5 W/cm2, and duration of 5 minutes [25]. Then, Kendall exercises were performed as follows: (a) Strengthening the deep cervical flexors: The patient was asked to do a flat-back, chin-down position and hold this position for 2–8 seconds, (b) Stretching the cervical extensors: The patient was asked to place one hand on the occipital area and other on the chin in a seated position, then a head-down, flexed neck position to stretch the cervical extensors, (c) Strengthening shoulder retractors: This exercise was done in order to move the shoulder blades towards one another while standing, the patient was instructed to wrap red (medium) Theraband around a stable item and then draw the band back as far as they could with both hands, (d) Stretching of the pectoralis major muscle: The therapist stood behind the patient and held both elbows and performed bilateral pectoralis stretching. To stretch the costal division, the arm should be elevated to approximately 135 degrees. For sternal division, the arm abducted to 90 degrees. For clavicular division, the arm was rested at the side. Every strengthening exercise was repeated for 12 repetitions and done for 3 sets and each stretching exercise was held for 30 seconds and repeated 3 times [26].
Comparison of subject characteristics between PNF and control groups
Comparison of subject characteristics between PNF and control groups
SD, Standard deviation;
Patients in the PNF group additionally received PNF stretching exercises for masticatory muscles. The procedures for applying the PNF exercises were done following the procedures that had been previously used by Travell and Simons [13] and Gray [19], and are detailed in the Supplementary Table 1. During PNF exercises, each contraction was held for 10 seconds, and each stretch (relaxation phase) was allowed to continue as long as the muscle tension continued to give away, for 5–10 seconds. The procedure was repeated three times for each affected muscle. Twelve sessions, two times each week for six weeks, were given to each patient in both groups.
For all patients, measures were taken twice: at baseline and after 6 weeks of treatment (the day after the last session). The assessment procedures include the following items:
Assessment of CVA using the photographic posture analysis method: Surgimap software ( Assessment of pain pressure threshold of masticatory muscles: The pain pressure threshold (PPT) over the temporalis and masseter muscles was assessed using an algometer with a 1 cm2 probe tip (FDIX Digital Force Gage; Wagner Instruments). The algometer has a good degree of reliability (ICC Assessment of temporomandibular joint ROM: Mandibular depression, protrusion, and lateral deviation were all measured with a caliper. The external auditory canals of both ears were covered with the fingers of both hands, and patients were instructed to open and close their mouths before moving their mandibular protrusion. The mandibular depression ranges between 34 and 44 mm. Up to 10 mm of active mandibular protrusion is considered normal. Equal distances from the midline should separate the mandibular lateral deviations. The usual range should be 10 mm when patients are requested to move their jaw to both sides without completely losing contact between their upper and lower jaw teeth. Assessment of the function of temporomandibular joints: Temporomandibular Disorder Disability Questionnaire was used for evaluating the temporomandibular joint function. It includes the following subsections: the Temporomandibular Disorder Disability Index, Temporomandibular Disorder symptom intensity scale, and Temporomandibular Disorder symptom frequency scale.
The Temporomandibular Disorder Disability Index (TMDDI) provides scores and information on many of the disabilities and symptoms with which patients with TMJ disorders can present. It consists of 10 questions, each with five possible answers with a score ranging from 0 to 4. The points of each question are then added and divided by the total number possible, and then multiplied by 100 to give the percentage. The Temporomandibular Disorder Symptom Intensity Scale (TMDSIS) and the Temporomandibular Disorder Symptom Frequency Scale (TMDSFS) are two visual analogue scales with seven parts each that assess the frequency and severity of a patient’s TMJ symptoms. The patient must rate the severity and frequency of their symptoms on a scale of 0 to 10 score levels. The score for each scale is added and then divided by the maximum score possible (7 sections Assessment of pain intensity using the Numerical Rating Scale (NRS): The 101 questionnaire was measured in written form, by asking the patient to mark a number between 0 and 100 on a horizontal line that best represented how much pain they felt at their worst and their least discomfort points. The patient’s average level of pain is represented as a percentage by the average of these two totals.
Sample size determination
Sample size was calculated using sample-size calculating software G
Data analysis
Descriptive statistics and unpaired t-test were conducted for the comparison of subject characteristics between groups. Chi-squared test was used for the comparison of affected side distribution between groups. The Shapiro-Wilk test was used to ensure that the data followed a normal distribution. To ensure group consistency, we used Levene’s test for homogeneity of variances. CVA, NPR, PPT, TMJ ROM, and TMJ function were examined using Two-way mixed MANOVA. For further multiple comparisons, post-hoc tests with the Bonferroni correction were performed. All statistical analyses were performed with a p-value of less than 0.05 considered significant. All statistical analysis was performed using SPSS version 22 for Windows (IBM Corp., Armonk, IL, USA).
Results
Baseline participant characteristics
Table 1 shows the subject characteristics of the study and control groups. There was no statistically significant difference between groups in age, sex, and affected side distributions (
Effect of treatment on CVA, PPT, NPR, TMJ ROM, and TMJ function
A significant interaction between treatment and time was discovered using mixed MANOVA (F
Mean CVA, NPR and PPT of masseter and temporalis muscles pre and post treatment of PNF and control groups
Mean CVA, NPR and PPT of masseter and temporalis muscles pre and post treatment of PNF and control groups
Mean; SD, Standard deviation; MD, Mean difference; CI, Confidence interval;
After treatment, the CVA, PPT of the masseter and temporalis muscles, and TMJ ROM (opening, protrusion, right and left deviation) of both groups increased significantly compared to pretreatment (
Between-group comparison
There was a significant increase in CVA (
Discussion
Mean TMJ ROM pre and post treatment of PNF and control groups
Mean TMJ ROM pre and post treatment of PNF and control groups
Mean; SD, Standard deviation; MD, Mean difference; CI, Confidence interval;
Mean TMJ function pre and post-treatment of PNF and control groups
Mean; SD, Standard deviation; MD, Mean difference; CI, Confidence interval;
Conservative treatment approaches for TMD patients are currently supported by evidence. It has been reported by Armijo-Olivo et al. [30] that physical therapy is one of the top 10 treatments for reducing neck and mandible pain and increasing ROM in TMD patients. However, there is still a gap in the literature about to what extent PNF stretching exercises for masticatory muscles could be effective for the treatment of those with TMD and FHP. So, the current study was conducted to examine the effect of PNF stretching exercises on pain intensity, ROM, CVA, pain threshold, and functional abilities in TMD patients with FHP. This study exhibits that the study group who obtained PNF exercises along with the routine physical therapy program demonstrated greater improvement than the control group who received routine physical therapy alone regarding pain intensity, pain threshold, CVA, ROM, and function in TMDs patients with FHP.
Algometer and NRS readings both measure a participant’s pain; one is an objective measure, the other subjective. In the existing study, the experimental group showed statistically significant differences in NPR, from 68.75
In between-group comparison, the significant improvement in pain intensity and pain threshold in favor of the PNF group comes in accordance with the existing evidence of Gray [19], who revealed that there was a statistically significant improvement in Masseter, Temporalis algometer readings favoring the PNF group for the treatment of masticatory myofascial trigger point-induced TMJ dysfunction. In addition, the results of this study come in agreement with Trampas et al. [20] who investigated the therapeutic effects of massage and stretching PNF on pain intensity and PPT at myofascial pain trigger points and found that the group receiving massage along with stretching therapy PNF techniques experienced a substantial improvement in pain and PPT. On the contrary, Freshwater and Gosling [31] reported that PNF exercises did not significantly decrease pain in TMD patients. This contradiction in the results between the two studies may be due to a difference in the inclusion criteria of the patients between the two studies. In the study of Freshwater and Gossling, both symptomatic and asymptomatic patients with a limited set of mouth openings were recruited; while in the current study, only symptomatic patients were recruited.
Regarding TMJ ROM, there was a significant improvement in both groups but more significant in the PNF group which is consistent with the findings of Malone et al. [32] advocate that “hold-relax” techniques are similar to Muscle Energy Technique (MET) for mandibular elevators (masseter, temporalis, medial pterygoid) in improving ROM, functional mobility. Besides, Calisgan et al. [23] demonstrated that PNF, myofascial releasing, and home exercises were found to be more successful in the treatment of bruxism than traditional treatment methods. Further confirmation of the superiority of PNF to improve joint ROM is provided by the data from previous studies applied to investigate its effect on different joints in the body. In a study conducted by Gonzalez-Rave et al. [33], the ROM of 51 patients’ hip and shoulder joints after using PNF procedures was examined, and they reported that joint ROM improved significantly more in the PNF group compared to the other groups (
Dysfunctions in the cervical paravertebral muscles have been linked to improper tension in the masticatory muscles, which has been linked to poor head position [36, 37]. So, when evaluating TMD patients, it is necessary to evaluate and treat the cervical spine and shoulder girdle in addition to the stomatognathic system in order to assist in relieving the complicated and persistent head and neck symptoms [2]. A possible explanation could be the biomechanical and neurophysiological relationships between the cervical spine and the TMJ [38]. So, the significant improvement in the CVA in the PNF group more than in the control group may be attributed to the significant improvement in the TMJ ROM, and PPT of the masseters and temporalis muscles in the study group than the control group. This explanation was confirmed by Halmova et al. [39] who investigated the causality between the myofascial pain in the head and neck and craniocervical dysfunction as well as the clinical value of physiotherapy, and they demonstrated the effectiveness of combining masticatory muscle therapy with cervical muscle relaxation and stretching exercises.
Further confirmation of the effect of PNF exercises on the alignment of the cervical spine by Lee [22] who concluded that a 4-week PNF exercise is an important component of treating the disc location at the TMJ by evaluating the correct alignment of the neck and the contraction of the upper cervical extensors. In addition, Maluf et al. [40] found that individuals with TMDs who stretched their superficial neck and masticatory muscles experienced a reduction in pain intensity and tension in their neck and craniofacial muscles. Overall the results of the current study confirm the superiority of PNF in addition to routine physical therapy programs compared to routine physical therapy programs alone regarding pain, PPT, ROM, and functionality in patients with TMDs with FHP.
There are issues in this study that need to be addressed. The first is that we don’t know how long the effects of treatment last because we haven’t done a follow-up examination after a long period after treatment was completed. Therefore, a study with a long-run follow-up period is needed. The second one is that our sample size was relatively small and the sample was restricted to patients aged 18–40 years; therefore, future studies are required for older patients with large sample sizes.
PNF stretching exercises of masticatory muscles with routine physical therapy programs improved CVA, PPT, TMJ ROM, and function of TMJ, and decreased pain in patients with TMD and FHP more than routine physical therapy programs alone. Therefore, in a clinical setting, the addition of PNF stretching exercises of masticatory muscles to routine physical therapy programs for patients with TMD and FHP is recommended.
Author contributions
M.S and W.M conceived the research idea and designed the study. M.S and W.M. recruited the study participants and performed the interventions. M.S, W.M, W.H, and E.M interpreted and analyzed the data. M.S and W.M drafted the manuscript. W.H and E.M critically revised the manuscript for important intellectual content. All authors contributed to revisions of the manuscript and reviewed the final version.
Data availability
The data that supports the findings of this study are available from the corresponding author upon reasonable request.
Ethical approval
The protocol was registered and received approval from the Ethics Committee at the Faculty of Physical Therapy, Cairo University (P.T.REC/012/004165).
Funding
The authors received no financial support for the research, authorship, and/ or publication of this article.
Informed consent
All patients signed a written informed consent form.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/BMR-230358.
Footnotes
Acknowledgments
The authors would like to extend their appreciation to all patients who participated in this study.
Conflict of interest
The authors declare no potential conflicts of interest with respect to the research, authorship, and/ or publication of this article.