
Abstract
BACKGROUND:
The growing use of telerehabilitation within the healthcare community has garnered substantial attention. In congruence with other healthcare fields, examining perceptions, barriers, and facilitators assumed paramount significance in the continuation and fortification of telerehabilitation practices among physiotherapists.
OBJECTIVE:
In this scoping review, we aimed to systematically map the literature on the perceptions of physiotherapists as well as the barriers and enablers of telerehabilitation in their daily practice.
METHODS:
The five-stage methodological framework recommended by Arksey and O’Malley (2005) was used for this scoping review. In the framework, eight databases were searched using key search terms such as “telerehabilitation”, “physiotherapists”, “readiness”, “enablers” and “barriers” All findings were organised into perceptions and readiness, enablers, and barriers.
RESULTS:
Fourteen articles met the inclusion criteria and were categorized as: (1) perception and readiness, (2) enablers, and (3) barriers. In the perception and readiness category, new trends in healthcare, advancement in physiotherapy practices and the benefits to clients were identified. The enablers identified included prior training, personal experience, familiarity with technology, functional equipment and space, and client selection. The barriers to the adoption of telerehabilitation in physiotherapy practice are pinpointed to poor technology, communication hurdles, limited availability, lack of familiarity, and client-related concerns.
CONCLUSION:
While initial evidence suggests a generally positive perceptions it is important to consider both facilitators and barriers when understanding adoption. This review’s findings revealed a wide research gap, with unequal weightage towards barriers compared to enablers, and highlights the need for further research. Developing telerehabilitation guidelines that cater to both physiotherapists and clients is necessary.
Introduction
Telerehabilitation encompasses the delivery of rehabilitation services, including assessment, intervention, evaluation, consultation, and education, through telecommunication technologies [1]. While the terms “telehealth”, “eHealth”, “telerehabilitation” are often used interchangeably [2, 3], the term telerehabilitation will be used in this paper to maintain consistency. This modality uses audio or video communication platforms that include phone-, image-, and/or sensor-based modalities, operating in synchronous or asynchronous modes. This setup allows the delivery of rehabilitation services in a home-based setting [4].
There is compelling evidence supporting telerehabilitation as an effective platform to provide physiotherapy services for various conditions, such as cardiac rehabilitation [5, 6, 7], musculoskeletal conditions [8, 9], and geriatric rehabilitation [10, 11]. Telerehabilitation’s impact extends further, demonstrating remarkable benefits such as improving pain and physical function [9], increasing the quality of life [12], reducing the rate of hospitalisation [5] and saving cost and money for those requiring rehabilitation services [13, 14].
The COVID-19 pandemic resulted in the suspension of face-to-face rehabilitation amidst fears of contact infection. However, the importance of the physiotherapy service during the pandemic was soon realized and prompted physiotherapists to turn to telerehabilitation as an alternative. With high levels of satisfaction reported among clients and physiotherapists [15, 16] an unprecedented surge in interest in telerehabilitation ensued among physiotherapists.
Despite the evident benefits of telerehabilitation, its adoption among healthcare providers can be attributed to a variety of issues, such as human [17, 18, 19], organizational [20] and technical factors [20, 21]. Acceptance among healthcare providers has been recognised as a key factor in the sustainability of adoption [22, 23]. These findings are consistent with similar observations among physiotherapists, where the uptake of telerehabilitation among physiotherapists may be influenced by their acceptance level [24].
Gaining insight into physiotherapists’ perceptions regarding telerehabilitation, therefore, could enhance its successful implementation. Several studies have discussed physiotherapists’ perceptions of telerehabilitation [14, 25, 26]. Overall, physiotherapists’ perceptions regarding the use of telerehabilitation were positive. Another study revealed that effective communication can facilitate the adoption of telerehabilitation [26]. This positive perception extends to developing countries, as evidenced by Krishnan, Cai and Muniandy [25] who found that Malaysian physiotherapists agree that telerehabilitation is a valuable approach for their clients.
Building on these perceptions, recent literature has highlighted key enablers influencing successful telerehabilitation implementation, among which familiarity with the technology has been advocated as an enabler to use telerehabilitation [27, 28]. Another key facilitator involves awareness campaigns that integrate educational components with the objective of increasing clients’ technological literacy levels [29]. In addition, effective communication has been identified as an enabler in facilitating telerehabilitation uptake [26].
Numerous significant barriers to the successful implementation of remote health care have been identified. These challenges encompass underdeveloped technology infrastructure coupled with limited Internet coverage [30, 31, 32, 33, 34, 35], and technology illiteracy [21, 31, 34]. Barriers extend to healthcare providers where clinical personnel exhibit undesired attitudes [36, 37, 38] and face challenges related to inadequate knowledge and experience [20, 38, 39]. Financial barriers, such as a lack of reimbursement for services [40], have also been identified as significant barriers. While constraints of the pandemic thrust the use of telerehabilitation upon healthcare providers, for it to continue to be sustainable, a greater understanding of the barriers and enablers is required to maintain the momentum created The objective of this review was to comprehensively map the existing perceptions of physiotherapists their readiness, and the enablers and barriers to the use of telerehabilitation and determine the gaps in the literature for further research.
Method and analysis
This scoping review was conducted between July and August 2023. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension (PRISMA) checklist was used to guide this review [41]. The study was approved by the Research Ethics Committee of Universiti Kebangsaan Malaysia (UKM PPl/111/8/JEP-2021-830).
Search strategy
The Population, Concept and Context (PCC) method was used to frame the review. The target population was physiotherapists, the concept was telerehabilitation and the contexts were perception readiness, enablers, and barriers.
The first author drafted and analysed the comprehensive search strategies based on PCC. The search terms: “telerehabilitation”, “perception”, “physiotherapists”, “readiness”, “enablers”, and “barriers were used during the search. Later, synonyms for each search were searched in the Medical Subject Headings (MeSH) and cross-checked by the second and third authors to ensure that all essential keywords were included in the search key terms. The Boolean operators “AND” and “OR”, truncation, and wildcards combined the keywords and phrases within each search.
Eight electronic bibliographic databases were search- ed to identify published articles in the Web of Science (WOS), Scopus, Emerald, the Cochrane Library, PubMed, EbscoHost Medline, Pedro, Ovid, and one from grey literature (Google). This review encompassed primary research studies from both published and unpublished sources. It was limited to English-language publications, without any restrictions on the date of publication. The selected literature was exported to the Rayyan software [42] for a second screening for duplication and eligibility. Additional hand searches were conducted to ensure the comprehensiveness of the search in this review.
Study selection
Two reviewers (LLS and JBMI) independently screened the titles and abstracts of all the retrieved studies. Two reviewers (LLS and JBMI) independently screened the full-text articles to determine relevant articles for analysis. Any disagreements regarding study selection were resolved by discussion between the two reviewers, and the persisting disagreements were resolved by consulting the researcher team (DKAS, SS, SK).
Preferred reporting items for systematic reviews and meta-analyses extension for scoping review (PRISMA-ScR) flow diagram.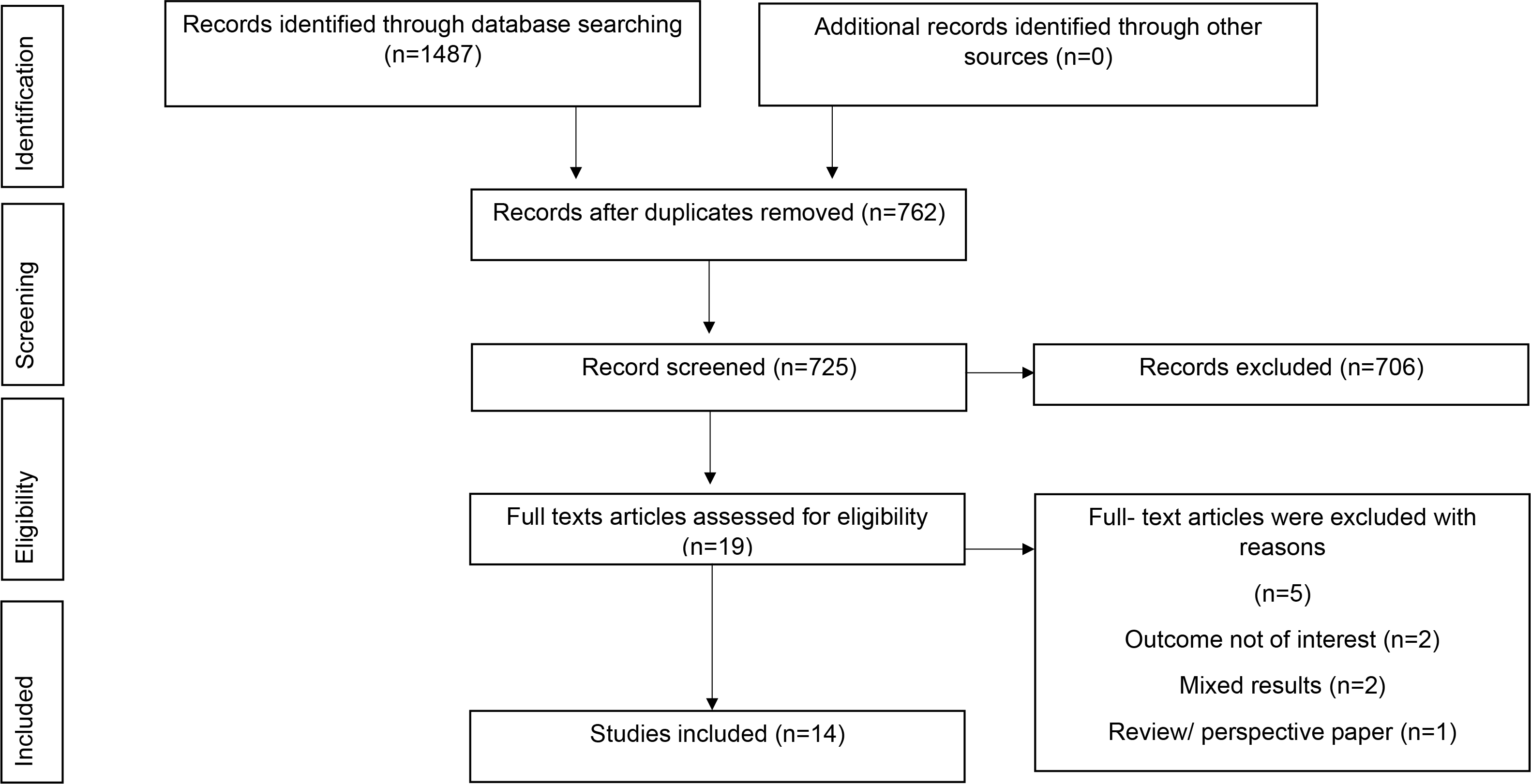
Figure 1 shows the selection of papers for this scoping review using the PRISMA flowchart. The stages of the peer-reviewed literature search are presented. One thousand four hundred and eighty-seven (1487) articles were identified in the initiated search, and 762 duplicated articles were removed. In total 725 articles were screened, of which 706 did not meet the inclusion criteria; the remaining 19 were screened for fulltext review. Five full-text articles were excluded for a range of reasons, including outcomes not aligned with the current research objectives (
Summary of included articles in review
A standardised data extraction form was created for this review (Table 1). All research team members reviewed the form to ensure comprehensiveness, and changes were made accordingly. The extracted data included author, year, country, title of the study study design, sample size (participant population, outcome types, and key findings.
Results
Description of studies (type of study)
Eight of the studies were quantitative [2, 19, 43, 44, 45, 46, 47, 48], five were qualitative [28, 49, 50, 51, 52], and one was a mixed-methods study involving online surveys and face-to-face interviews [18]. Most studies were conducted in Western countries (
Eight studies were conducted using online surveys [2, 19, 43, 44, 45, 46, 47, 48], one via an online semi-structured interview [51], one via an online focus group discussion (FGD) [49], and one utilised a combination of an online semi-structured interview and focus group discussion [52]. Two studies were conducted using face-to-face interviews [28, 50] and one study used a mixed method [18]. The numbers ranged from six to 273 [2, 18, 19, 28, 43, 44, 45, 46, 47, 48, 48, 50, 51, 52].
Perception and readiness
New trend in Healthcare
Eight studies provided insights into physiotherapists’ perceptions of telerehabilitation [18, 19, 44, 45, 46, 47, 50, 51]. Among these eight studies, two studies reported that telerehabilitation has a potential role in healthcare [18, 19]. Additionally, one study reported that telerehabilitation created new responsibilities for physiotherapists in their practice [44] and that the new trend in healthcare could create new opportunities to access physiotherapy services. For example, one study [45] recommended that telephone and video delivery care could allow more ways to access physiotherapy services. The study revealed that physiotherapists perceived e-health as providing novel opportunities to engage with a broader client tele, experiencing lower back pain [50].
According to the findings of a study [51], physiotherapists believed that a telephone-based approach could offer more opportunities for educating clients with knee osteoarthritis; a contrasting perspective emerged in another study conducted in Sri Lanka. The physiotherapists in their study expressed less interest in telerehabilitation through telephone-based methods [47]. While there was a general trend toward supporting telerehabilitation, one research [46] cautioned that telerehabilitation could not replace conventional physiotherapy.
Advancement in physiotherapy practice
Five studies reported that telerehabilitation improved physiotherapy services [18, 19, 44, 46, 51]. Two studies explored the potential of telerehabilitation in enabling physiotherapists to concentrate more effectively on communicating with their clients [44, 51]. One study’s findings emphasised the potential for physiotherapists to facilitate more personalised client interactions and improve treatment outcomes [51]. Physiotherapists acknowledge that telerehabilitation could enhance client communication [44]. Another study [46] found that telerehabilitation’s communication quality was comparable to that of in-person therapy sessions. Two previous studies [18, 19] suggested that telerehabilitation could reduce the workload of physiotherapists and senior physiotherapists stated that telerehabilitation could encourage their clients to perform exercises at home [18]. Another study supported the finding [19], as in a recent study, over fifty percent of physiotherapists believed telerehabilitation could decrease their workload.
Benefits to clients
Four of the studies [18, 19, 45, 51] addressed that telerehabilitation could benefit clients. Three of the studies [18, 19, 45] reported that telerehabilitation could save clients’ money and time. In both the Australian studies [45, 51] and a study from Sri Lanka [47] reported that client privacy is preserved, and clients’ confidence in the self-treatment of their illness can be strengthened.
Enablers
Five studies have reported the enablers of telerehabilitation [18, 28, 49, 51, 52]. Two research teams reported that training was an enabler for implementing telerehabilitation [49, 51]. One study [51] emphasised the significance of various enablers that improving telerehabilitation uptake such as communication training, pre- telerehabilitation screening, and availability of written materials such as video and exercises link. The influence of firsthand experience among physiotherapists is also highlighted as another factor that enables the shaping of their perception and fostering the implementation of telerehabilitation. Technology familiarity was reported as an enabler to empower physiotherapists to use telerehabilitation in two previous studies [18, 28]. One study [18] underscored the importance of selecting well-educated and cooperative clients as enablers in the uptake of telerehabilitation Another study’s finding [52] further emphasised that, especially in paediatric rehabilitation, appropriate technology equipment, sufficient space, and careful selection of the right candidates collectively contributed to the advancement of telerehabilitation.
Barriers
Eleven studies identified various barriers to telerehabilitation including those relating to technology, communication availability of equipment and familiarity with equipment related and client- related issues [2, 18, 19, 28, 43, 44, 47, 48, 49, 50, 52].
Technology-related issues
Seven studies identified barriers to telerehabilitation [18, 28, 44, 47, 49, 50, 52]. Six studies reported technology-related barriers such as unreliable Internet use in rural areas and poor Internet access in their workplaces [18, 44, 47, 49, 50, 52]. One study addressed poor design and outdated content in the application for telerehabilitation as technology-related issues [28].
Communication-related issues
Four studies reported communication-related issues as barriers to telerehabilitation [18, 19, 49, 52]. Insufficient information technology (IT) support provided by IT experts has been recognised as a prevalent barrier to the implementation of telerehabilitation, as indicated by three studies [18, 19, 52]. Physiotherapists noted that it takes longer to establish rapport with clients during telerehabilitation sessions [49, 52]. They also found that communication quality between parents and children is lower during telerehabilitation, leading to longer sessions compared to face-to-face interactions [52].
Availability and familiarity-related issues
Physiotherapists from Australia, Kuwait, Greece, and India highlighted the lack of suitable training in the use of equipment to practice telerehabilitation [18, 19, 48, 52]. Another barrier to the practice of telerehabilitation was a poor familiarity with the technology used [44, 48, 52]. In Ireland and Greece, physiotherapists identified the lack of private space for telerehabilitation as the most significant barrier [2, 48].
Client-related issues
Physiotherapists highlighted client’s technological illiteracy as a barrier to telerehabilitation [43, 47, 50]. In Sri Lanka, technical issues were the main barrier for clients [47]. Two additional studies pointed out that older adults can be barriers to telerehabilitation, citing challenges in persuading them to engage in telerehabilitation [43] and noting lower levels of technological literacy among this demographic [50].
Discussion
This study aimed to map the existing evidence on physiotherapists’ perceptions and readiness and address the enablers and barriers to telerehabilitation. It also highlights gaps in the literature for further research in the field of telerehabilitation. Despite the existence of some enablers, the review revealed multiple barriers including technological limitations, communication difficulties, restricted accessibility, reluctance to adopt, and factors specific to clients. This review found evidence that generally physiotherapists had a positive perception of the uses of telerehabilitation. This is consistent with a previous study, in which the majority of physiotherapists conveyed a favourable perception that telerehabilitation has the potential to be an effective approach for clients in various aspects, such as saving time and cost [14].
Notably, positive perceptions toward telerehabilitation extend beyond physiotherapists; occupational therapists and speech-language therapists also hold favourable perceptions towards telerehabilitation. For example, most speech-language therapists broadly accept telerehabilitation in their practices [53, 54]. Similarly, an online survey of occupational therapists revealed comparable results, indicating that most respondents perceived remote care as an effective and legitimate delivery method [55]. This is consistent with another finding that emphasised the importance of effective communication as a facilitator in enhancing physiotherapy services during telerehabilitation [26].
The existing literature on effective communication in telerehabilitation yields conflicting results, with some studies reporting positive outcomes and others presenting challenges among healthcare providers. Notably, the provision of online healthcare services can enhance communication between healthcare providers and homebound elderly clients [56]. In contrast, clinicians emphasised losing interpersonal connections with their clients during remote healthcare services as challenging to understand clients’ feelings [57]. Similarly, nurses expressed concern about the perceived loss of therapeutic communication through virtual healthcare services [58].
Maintaining a consistent bandwidth is vital for delivering effective virtual healthcare services and ensuring seamless, efficient client care, especially when conducting sessions in real-time Real-time or synchronous methods can facilitate immediate interaction [59], and closely resemble face-to-face sessions [60]. However, the most commonly reported barrier in this review was technology-related, namely unreliable internet signals, in the more rural areas. Nonetheless, these challenges can be addressed by utilizing asynchronous (store-and-forward) methods, which introduce a communication delay, often through pre-recorded videos [61], providing greater flexibility in scheduling for both therapists and clients [62].
While physiotherapists are generally positive toward telerehabilitation, physiotherapists also recognise the vital roles of enablers in the telerehabilitation implementation. The significance of enablers, such as training, is manifested in the success rate of telerehabilitation [51]. To achieve successful adherence with telerehabilitation it is crucial to provide comprehensive education and training to healthcare professionals, including nurses. In Brazil, nurses have underscored the importance of proper communication training to enhance their engagement with online healthcare services [63]. The provision of an option of either a writing format or online assistance is another enabler that could facilitate the utilisation of telerehabilitation [64, 65].
This review identified that despite positive perceptions and enablers, several barriers must also be addressed. The instability of internet signals was commonly reported as a barrier among physiotherapists [32, 35]. Studies have reported that these issues are not confined to physiotherapists; other disciplines have reported similar issues. For instance, difficulty with Internet access remains a common barrier in virtual healthcare services, as reported by speech-language therapists in a three-month trial [65].
Furthermore, more than 65% of medical practitioners highlighted common technology-related barriers such as a lack of technological literacy and limited Internet access in their online healthcare services [34]. These findings were supported by a systematic review, as technical literacy was the most reported barrier among older adults [31]. Paediatric palliative care clinicians faced a technological barrier, specifically the restricted visual field of a screen. This limitation was felt to curb their professional autonomy and lead to discomfort in relying on technology [66]. Another prominent barrier reported in this scoping review is the lack of experience in telerehabilitation [67]. Notably, a lower knowledge level of telehealth leads healthcare providers to have a lower comfort level when using telehealth [39].
The main discoveries of this study provide valuable insights that can guide future physiotherapy practices. These insights emphasize the significance of customized training in implementing telerehabilitation effectively. Furthermore, there’s an urgent requirement to establish telerehabilitation guidelines that cater to the requirements of physiotherapists and their patients. These guidelines should offer evidence-based suggestions for choosing suitable therapies to ensure the delivery of optimal care.
Strength, limitations, and recommendations
This review has multiple strengths, including the implementation of a rigorous and transparent search strategy that adheres to best practices in conducting and reporting research. This review mapped the process, analysed the available literature on physiotherapy, and attempted to identify gaps in the literature. To conduct a comprehensive literature search, the search method encompassed the right electronic databases and grey literature. A multi-layered approach was used in the scoping review to ensure the quality and reliability of the findings. Each article was reviewed independently by two reviewers Furthermore, a research team with significant expertise in synthesis and review evaluated the included studies.
This scoping review, however, was confined to studies published in English only with most of the included studies conducted in Western countries. Therefore, it is a possibility that relevant literature published in other languages and geographical areas may have been missed. The methodological quality of the included studies is unknown and what, if any, impact this may have on the findings reported from the included studies is unclear, as a critical appraisal was not conducted Therefore, further robust research on the use of and perceptions about telerehabilitation in the global context is required.
Conclusion
Our analysis delved into the viewpoints, facilitators, and barriers faced by physiotherapists regarding telerehabilitation. While initial evidence indicates a generally positive outlook among physiotherapists towards telerehabilitation, mere perceptions and preparedness do not fully elucidate the reasons behind its adoption. Exploring both the facilitators and barriers provides a more comprehensive understanding. Notably, our research revealed a disproportionate emphasis on barriers compared to facilitators, highlighting a research gap in comprehending the factors that promote the integration of telerehabilitation into physiotherapy services. Further studies are necessary, particularly in developing telerehabilitation guidelines that cater to the needs of both physiotherapists and their clients.
Author contributions
LLS conceived the original review. SS, DKAS collaborated with LLS to refine the review topic and developed the search strategy. Both LLS and JBMI independently screened the titles and abstracts and thoroughly reviewed the full-text articles to identify relevant studies for analysis.
SS, SK, and DKAS provided consultation and assistance during the critical appraisal, data extraction, and data synthesis stages. LLS, SS, SK, and DKAS all contributed to the development of this manuscript and approved the final version.
Data availability
Not applicable.
Ethical approval
This study was approved by the Research Ethics Committee of Universiti Kebangsaan Malaysia (UKM PPl/111/8/JEP-2021-830).
Funding
The authors received no funding to conduct this study.
Informed consent
Not applicable.
Footnotes
Acknowledgments
The authors declare that they have no conflicts of interest.
Conflict of interest
The authors declare that they have no conflicts of interest.